Article Text

Abstract
Background Indigenous Peoples are subject to marginalisation, and experience systematic disadvantage in relation to health outcomes. Human development initiatives may help determine whether, and how, Indigenous Peoples are able to be agents of their own development and improve their health and well-being. This scoping review protocol outlines a process for synthesising the existing evidence that has applied the capability approach (CA) to Indigenous People’s health and/or well-being.
Methods and analysis A mixed-method scoping review is proposed including academic peer-reviewed publications and grey literature. Screening inclusion criteria will include Indigenous populations, using the CA approach to conceptualise health and/or well-being, and be available in English, Spanish, French or Portuguese. Publications that meet these criteria will undergo data extraction. Qualitative and quantitative data will be thematically and descriptively analysed and interpreted.
Ethics and dissemination The proposed scoping review does not involve collecting data directly from Indigenous Peoples but will be based on previous research conducted within Indigenous settings. The current protocol and the proposed scoping review incorporate aspects of community involvement to guide the research process.
This scoping review constitutes the first phase of a wider participatory action research project conducted with the Indigenous Kankuamo Peoples of Colombia. The findings of this review will be reported to local partners, published in a peer-reviewed journal and an executive summary will be shared with wider stakeholders. Within the wider project, the review will be considered alongside primary data to inform the development of tools/approaches of mental health and well-being for the Kankuamo communities.
- protocols & guidelines
- mental health
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This scoping review will synthesise existing qualitative and quantitative evidence that has applied the capability approach in the field of Indigenous People’s health and/or well-being.
This protocol provides a comprehensive list of indigenous search terms for the South American region.
This scoping review incorporates aspects of community involvement to guide the research process.
An inherent limitation of this scoping review is to provide breadth rather than depth of information.
Background
It is estimated that there are between 370 and 500 million Indigenous People across 90 countries worldwide.1 The United Nations (UN) states that ‘Indigenous Peoples are inheritors and practitioners of unique cultures and ways of relating to people and the environment. They have retained social, cultural, economic and political characteristics that are distinct from those of the dominant societies in which they live. Despite their cultural differences, Indigenous Peoples from around the world share common problems related to the protection of their rights as distinct peoples’.2 Given the diversity of Indigenous Peoples, an official definition has not been adopted by the UN (UN Permanent Forum on Indigenous Issues (UNPFII)).3 Instead, it considers the criterion of self-identification as a fundamental human right that gives primacy to invite communities to self-identify as Indigenous, rather than this being decided by others.3
Historically, Indigenous Peoples have faced significant exclusion and discrimination in terms of their basic rights to ancestral property, languages, cultures and forms of governance, in addition to a lack of access to basic services and material conditions.4 This remains a problem today, with the World Bank estimating that although Indigenous Peoples constitute roughly 6% of the global population, they also account for 19% of the extreme poor.1 Compared with non-indigenous groups, evidence suggests low levels of education, higher employment rates in lower paying jobs, lack of access to basic services such as water, sanitation and healthcare, and decreased access to food resources.5–7 These inequalities can impact on health and well-being, with available information showing that Indigenous Peoples exhibit significant health gaps in comparison with the majority population.2 8 Examples of this health gap include higher levels of diabetes, tuberculosis, malnutrition, maternal and infant mortality, HIV/AIDS, cardiovascular illnesses and other infectious diseases such as malaria.8 Research across communities also suggests higher suicide rates of Indigenous Peoples, particularly youth, compared with majority populations.9 Furthermore, Indigenous Peoples are more likely to experience disability, reduced quality of life and ultimately die younger, with life expectancy rates being up to 20 years lower as compared with their non-indigenous counterparts.6
Human development and the capability approach
Human development can be defined as improving the well-being of every individual within society by creating fair opportunities and choices for all people to live lives that they value.10 Owing to the high levels of exclusion and discrimination faced by Indigenous Peoples, there has been an increased focus on providing opportunities for Indigenous Peoples to identify and articulate their own development priorities. This was partially motivated by the recognition that conventional development paradigms have often perpetuated the exploitation and discrimination of Indigenous Peoples, rather than focusing on what they have reason to value.11 12 Such policies and programmes frequently overemphasised the material and economic aspects of development and well-being, while paying little attention to the social, political, cultural and ecological contexts.13 In response to this, in 2007 the Declaration on the Rights of Indigenous Peoples was created by the UN General Assembly,14 which allowed for states to formally recognise the distinct status of Indigenous groups and elaborates international obligations to protect and promote the human rights of Indigenous Peoples.15 Specifically, this declaration included the minimum standards required to ensure ‘the survival, dignity and well-being of the Indigenous Peoples of the world’ (article 43,14), and asserted that individuals and/or communities must be agents of their own development and set their own priorities.14
Over the last few decades, several initiatives have aimed to include Indigenous Peoples in the identification and articulation of their rights and development priorities. For example, in 2006 the UNPFII convened a series of workshops focusing on Indigenous Peoples’ conceptions of well-being and suggestions for how well-being might be measured across different settings.16 Specifically, they aimed to identify gaps in existing well-being indicators, examine the work being done to improve indicators, review linkages between quantitative and qualitative indicators, and propose a core global and regional list of well-being indicators that address the specific concerns of Indigenous Peoples.16 Another example is in New Zealand, where the state government is collaborating with Māori communities in developing a framework to address health inequities and deliver high-quality and effective services that support Māori aspirations for health and well-being.17 Policy initiatives and organisations have also aimed to reduce the social and economic disadvantage experienced by Indigenous Peoples, for example, The Transformative Change Accord (2005) in Canada.18 Attempts at identifying and articulating development priorities and indicators of well-being for Indigenous Peoples are also found in academic research from Australia19 20, Canada and the USA,21 and the North of Russia,22 among others.
Ideas about how human development is understood, designed and implemented plays an important part in determining whether and how Indigenous Peoples can be agents of their own development. Specifically, approaches that engage with the lived experiences of the communities themselves are recommended.23 The capability approach (CA) has been proposed as a useful framework for interpreting Indigenous rights, framing Indigenous policies and articulating what it means to live a good life.23 The CA is a people-centred normative framework that provides an alternative to welfarist or utilitarian resource-based evaluations of well-being. Instead, it proposes that what matters for well-being and human development should be considered in terms of the real opportunities or capabilities, that people have to live the lives that they have reason to value.24 25
The CA, first articulated by Amartya Sen, uses the concepts of ‘capabilities’ and ‘functionings’ to describe well-being and development. According to Sen, functionings are the valuable ways that people behave and the things that they do (‘beings and doings’) through which well-being manifests; whereas capabilities are the alternative combinations of functionings that a person can potentially achieve if they choose to.25 Therefore, functionings are achieved states whereas capabilities are the set of possible states one can potentially achieve. The CA recognises that people have different abilities to convert goods and resources into valuable functionings, and this is influenced by an individual’s personal, social and structural environmental factors.26
The CA contends that social and public policies should aim to expand people’s capabilities, and a policy would be considered successful if it leads to an expansion of a persons’ capability set.25 To aid the development of social and public policies there have been attempts to identify and categorise which capabilities these should target. Martha Nussbaum was the first to develop a list of universal capabilities based on the understanding of minimal capabilities required to live a dignified life.27 This was influenced by her understanding and consideration of different philosophical perspectives, which led to a central list of ten human capabilities, namely Life; Bodily Health; Bodily Integrity; Senses, Imagination and Thought; Emotion; Practical Reason; Affiliation; Other Species; Play; and, Control Over One’s Environment.24 This list raised questions over its prescriptiveness,28 concerns with it not being sufficiently attuned to quantitative empirical applications and measurement,29 and controversy with regards to Sen’s central idea of pluralism.30 Sen explicitly refrained from endorsing a universal list of capabilities, stating that different capabilities are relevant in different contexts and can be influenced by personal, social and environmental factors.31 Instead of using a predetermined list, Sen highlights there is a need to work closely and collaboratively with communities to identify what different people value and prioritise in different contexts.32 This provides important insights into which capabilities are worth promoting in any given context, and why.
The context-sensitive nature of the CA aligns with the UN Declaration on the Rights of Indigenous Peoples, which states that Indigenous People need to be agents of their own development. Consequently, the CA is an attractive approach to understanding the health and well-being of Indigenous Peoples as it places the person(s) at the centre of human development, enriching understanding of the pathways towards human development and a person’s agency to realise the capabilities that they themselves have reason to value.23 33 While enhancing the capabilities of the individual is important, it is also one of the most persistent criticisms the CA receives. Specifically, multiple researchers have argued that the CA is excessively focused on the individual and fails to facilitate sufficient insights into the relational determinants of human well-being and freedom.34 35 As an alternative, these researchers propose the need for the concept of ‘collective capabilities’, which considers the importance of collective action in expanding human freedom.36–38 In other words, collective capabilities are those freedoms whose nature ‘requires that it be sought in common’ (Taylor, p5939). Two main criteria exist that can help distinguish between individual and collective capabilities.36 First, collective capabilities are dependent on collective action; and second, the wider community can benefit from the newly generated capabilities. As such, these capabilities constitute choices/freedoms the individual would not have had nor would have been able to achieve had it not been for the collective group (ie, recognition of Indigenous rights). This is particularly relevant to indigenous settings, as research suggests that Indigenous Peoples strive for their well-being through the individual and collective capabilities for self-determination. As noted by Gordon and Datta40; ‘efforts to achieve Indigenous well-being through the individual and collective capabilities for self-determination should be led by Indigenous people within their communities in order to take into account indigenous knowledge systems, ways of governing, treaty negotiations and indigenous worldviews’ (Gordon and Datta, p20).
Recently, Yap and Yu41 also reported that framing the CA using indigenous worldviews is not only key to understanding their human development, it is also a helpful way of informing capability-based tools. Such tools would facilitate the monitoring and evaluation of health, well-being and human development more broadly in Indigenous communities as per their self-defined understanding of what a ‘good life’ means to them. While research with Indigenous Peoples using the CA is growing37 42, the literature remains scarce and largely unpublished.
Methods and design
This protocol describes the methodology for a mixed method scoping review. Scoping reviews aim to systematically map the available literature on a topic, to clarify key concepts in the literature, examine how research is conducted on a certain topic, identify key characteristics of the topic, be a precursor to a potential systematic review, and identify and analyse knowledge gaps.43–45
Given the breadth of the research questions driving this study, a scoping review methodology was chosen to help identify areas for future research and knowledge gaps. The current protocol was designed in accordance with the ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews’ reporting guidelines (online supplemental file 146). This study has been registered with the Open Science Framework.
Supplemental material
Review question
The aim of this scoping review is to synthesise existing qualitative and quantitative evidence that has applied the CA to the field of Indigenous People’s health and/or well-being, addressing the following research questions:
In which geographical locations has the CA been integrated with indigenous conceptualisations of health and/or well-being?
What CA dimensions (eg, capabilities, conversion factors, functionings) have been identified as being important for the health and/or well-being of Indigenous People?
What are the similarities and differences in CA dimensions relating to health and/or well-being across different Indigenous settings?
What, if any, capability-based assessment tools/approaches have been used with Indigenous peoples?
The components of population, exposure, comparator and outcome (PECO) for this review are:
Population: Indigenous peoples.
Exposure: Indigeneity.
Comparator: None.
Outcome: The conceptualisation and application of the CA to understand and/or measure dimensions of the health and/or well-being of indigenous peoples.
Study designs eligible
Studies will be selected according to the criteria outlined in table 1.
Inclusion and exclusion criteria
Supplemental material
Historically, there has been relatively little research relating to the CA and Indigenous Peoples published in peer-reviewed journals.23 As such, a pragmatic search strategy will be adopted including both the identification of peer-reviewed articles and grey literature including book chapters, theses and policy papers. The following peer-reviewed databases will be searched: Web of Science, PsycINFO, EMBASE, OVID MEDLINE, ECONlit, LILACS (Literatura Latino Americana em Ciências da Saúde), Aboriginal and Torres Strait Islander health bibliography, SCIELO, ADOLEC, Biblioteca Virtual en Salud Medicinas Tradicionales Complementarias e Integrativas (BVS MTCI) and IBECS (Índice Bibliográfico Español en Ciencias de la Salud). Additionally, the PubMed database will be searched using the Lowitja Institute search tool for access to Aboriginal and Torres Strait islander health literature (https://www.lowitja.org.au/page/research/lit-search), and the Journal of Human Development and Capabilities will be searched through the Indigenous Peoples’ thematic group’s publication list. To identify relevant grey literature, filter terms will be used relating to the CA and Indigenous Peoples (ie, World Bank: (‘Capabilit* Approach’ AND ‘Indigenous People*’)). The following grey literature sources will be searched; Department of Economic and Social Affairs Indigenous Peoples United Nations resources (https://www.un.org/development/desa/indigenouspeoples/publications/desktop-publications.html), World Bank e-Library, Pan American Health Organisation e-library, Opengrey and Social Care Online. Citation searching in retrieved papers that are included in the review will also be done, and experts that are part of the Human Development and Capabilities Association’s ‘Indigenous Peoples’ thematic group will be consulted to identify additional sources.
Search methods for the identification of studies
For academic bibliographic databases, a combination of free text searches using keywords, Medical Subject Heading or filter terms will be used to search the title and abstracts of sources. Due to the limited functionalities of grey literature resource libraries, searches will involve the use of keywords which will be combined where possible (ie, using simple Boolean operators), or by hand searching relevant sub-sections of sites, for example, collections of Indigenous literature. The search strategy comprises two main components: Indigenous Peoples and CA terms.
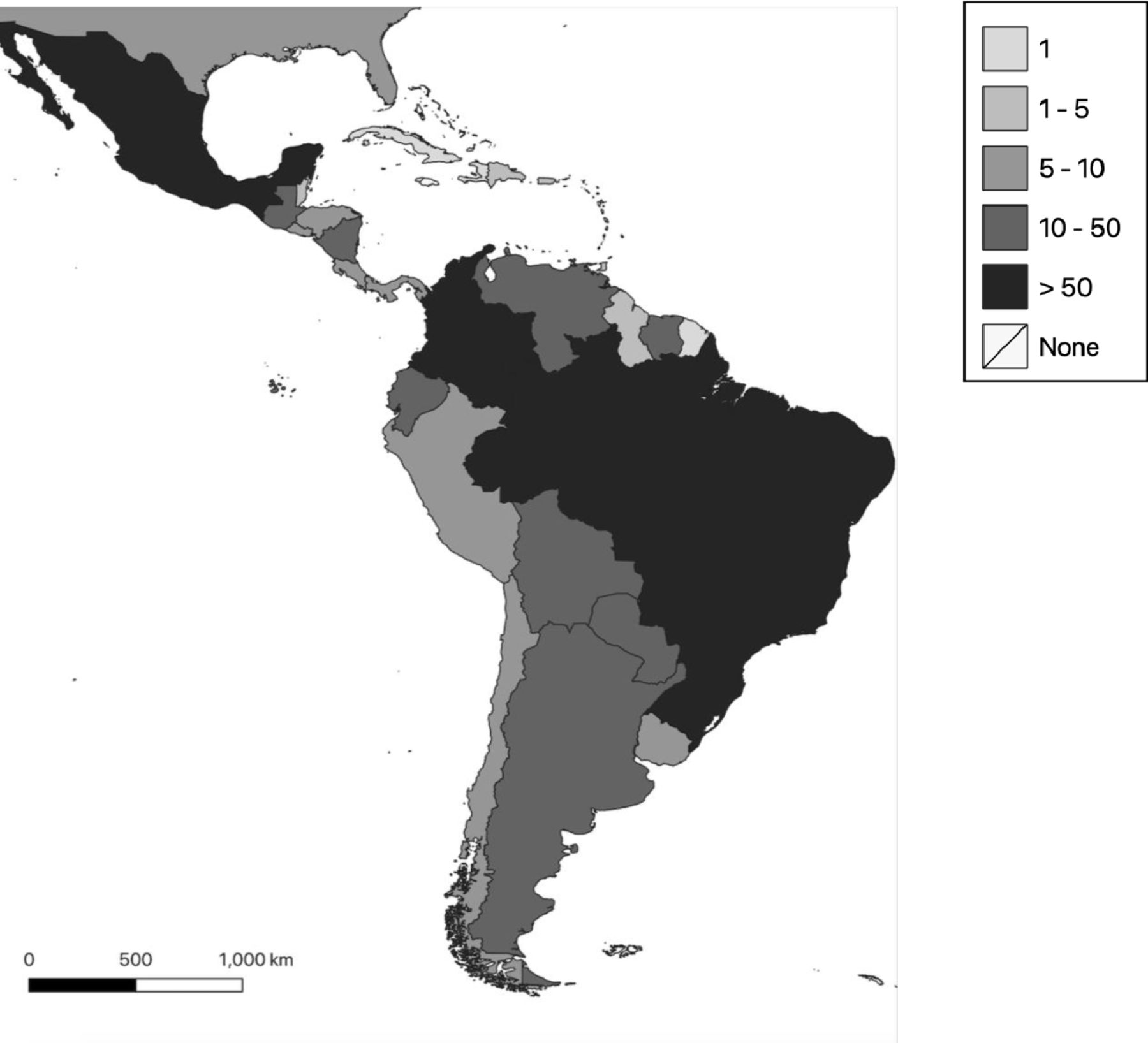
A list of Indigenous community names compiled by Bishop-Williams et al.47 from two major international sources was used as the baseline for the populations to include in the search strategy. Building on Harding et al’s48 recently expressed concerns about how transparent and complete this list is, we have supplemented the list for the purpose of this review. Given that our review is part of a larger project investigating the mental health and well-being of Indigenous Peoples in Colombia, the authors (CvdB and CIM-B) further investigated available, comprehensive, lists of Indigenous Peoples specific to South America. An individual list was drawn for each of the South American country (see https://et-ivc.shinyapps.io/cvdb/), and these were used to complement the baseline strategy created by Bishop-Williams et al.47 As a result, the search strategy created for the current review sought to ensure completeness for the South American region, while recognising that to be fully comprehensive a similar exercise would need to be completed for other continents. The differences between the two search strategies are visually represented in figures 1 and 2. To see an interactive representation visit: https://et-ivc.shinyapps.io/cvdb/. The full search strategy can be found in online supplemental appendix A.
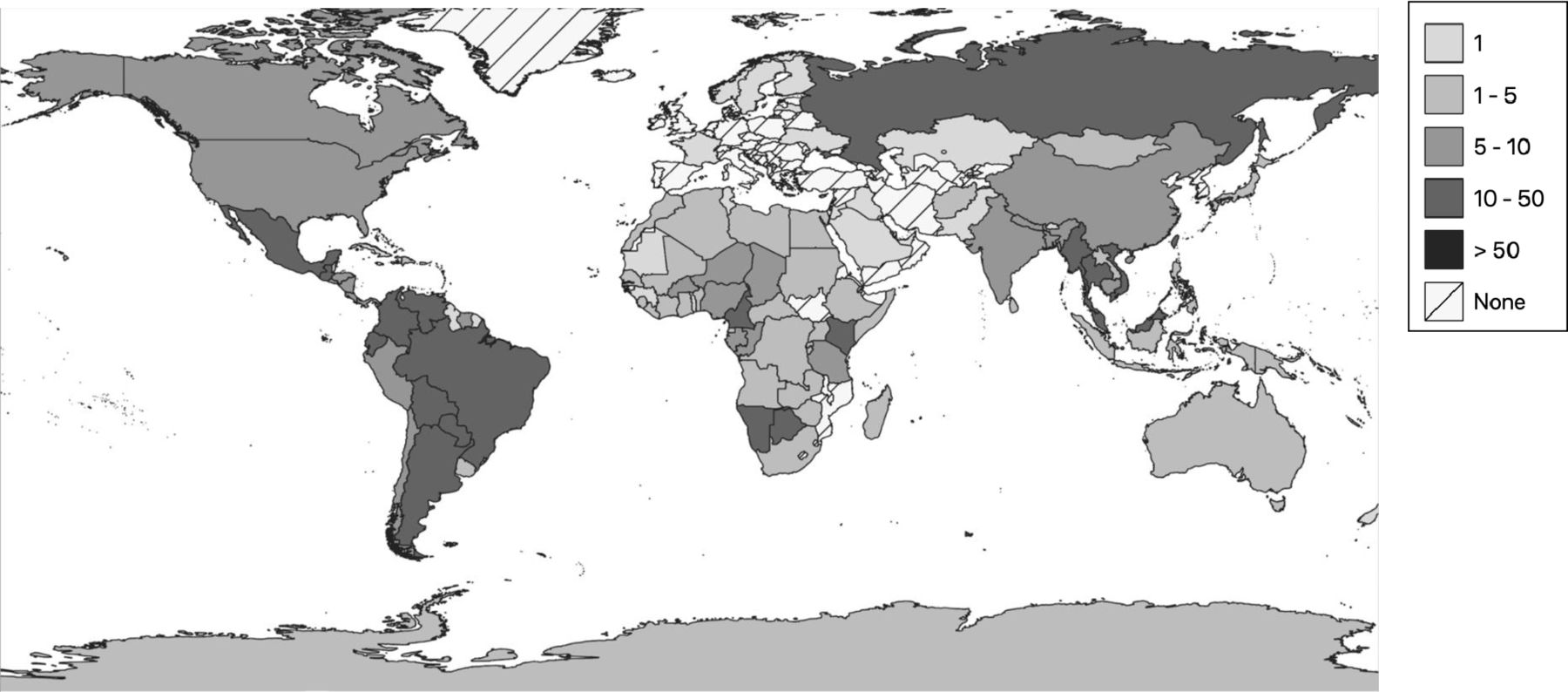
A visual representation of the indigenous peoples covered globally by the search string created by Bishop-Williams et al.47

{kind=link}
{kind=link}
A visual representation of the additional indigenous peoples from the South America region included in the search string for the current review.
Selection of eligible studies
All sources collected from academic databases will be uploaded to Endnote bibliographic software and duplicates removed automatically. Then, sources will be uploaded to Rayyan (https://www.rayyan.ai) which facilitates the screening and management of references across reviewers. Non-academic sources will be manually imported into Excel to be shared across reviewers for two-stage screening and then full text review, as recommended by Levac et al.44
CvdB will independently screen all English titles, abstracts and subject description of each source against the inclusion/exclusion criteria to identify potentially relevant sources. A similar exercise will be done by CIM-B for the Spanish, Portuguese and French sources. For each language, 20% of the titles will be double screened by a second reviewer. Of these 20%, articles rated as candidates for inclusion by either the first or second reviewer will be added to a preliminary list for each language. This list will be compared across the two reviewers of each language, and any discrepancies will be resolved through discussion, where required further review of the title/abstract by a third person and consensus agreement among the research team.
Once screening is complete, two reviewers will then review the full texts and apply the inclusion and exclusion criteria to each source to identify those that should be further included or excluded. Where necessary and possible, additional information from authors will be requested. Any reviewer discrepancies will be discussed with a third reviewer to reach a consensus. A record will be kept with reasons for exclusions.
Data collection from eligible studies
As this is a mixed-method review, both qualitative and quantitative data will be extracted. See table 2 for a template of the data extraction form. CvdB will extract the data of all the English included sources and CIM-B will do the same for the Spanish, French and Portuguese sources. In all cases, 20% of the data will be extracted in duplicate by a second member of the review team. To promote consistency, a calibration exercise will be conducted before starting the review. Any disagreements will be resolved through discussion, and if a consensus cannot be met then a third rater will be asked to adjudicate. A standardised data extraction form will be used for the included sources (see table 2). The questions highlighted in table 2 will be considered for each source independently, and where not applicable due to the source type, this will be explicitly marked. Where the question is relevant to the source type, but the data are missing, this will also be explicitly stated in the table.
Template of the data extraction form
Supplemental material
If there is unclear, missing or unusable data, the authors of the source will be contacted via email for clarification (where available). Authors will be given 3 weeks from the initial email to respond, if they do not respond within this time frame then the data will be reported as missing. In line with the scoping review methodology,43 44 no quality appraisal of the included sources will be conducted.
Strategy for data synthesis
The qualitative findings will be pooled using a thematic synthesis and following the guidelines developed by Thomas and Harden,49 and quantitative data will be presented in a summary table. To synthesise the qualitative research, the three stages proposed by Thomas and Harden49 will be followed, namely: (1) coding of text ‘line-by-line’; (2) development of ‘descriptive themes’ and (3) generation of analytical themes. Within this methodology, the development of descriptive themes stay close to the primary study, whereas the analytical themes represent an interpretative stage whereby new interpretive constructs, explanations or hypotheses are created. NVivo V.12 software will be used to manage qualitative data and facilitate thematic synthesis. These stages will be carried out independently by CvdB and CIM-B to ensure all languages are covered. The development of themes and concepts and the translation and synthesis of data across multiple sources will be discussed and reviewed by all co-authors at regular team meetings to support the development of robust interpretation and analysis of included sources. The quantitative findings will be descriptively summarised. A meta-analysis will not be conducted given that we expect high levels of variation in the data with regards to population, measures and outcomes. Efforts will be made to bring together the qualitative and quantitative findings in an overarching discussion to identify gaps in the literature and make recommendations for sustained research to build an evidence base that could potentially be subject to a systematic review.
Patient and public involvement
This review constitutes the first phase of a wider participatory action research project that aims to apply the CA to develop locally relevant tools/approaches of mental health and well-being for the Kankuamo Indigenous Peoples of Colombia. The aim of the research project is to support the Kankuamo people in the recovery and strengthening of their community knowledge. In addition, the project aims to inform the construction of an indigenous intercultural health system in partnership with Instituto Prestador de Salud, which is embedded within Colombian health systems. The Kankuamo authorities and health leaders have been involved from the conception to the design and implementation of this wider project. The findings of this review will be shared with the Kankuamo authorities through a brief summary report in Spanish.
Discussion
There has been a growing interest in understanding the health and well-being needs and priorities for Indigenous Peoples across the globe. This has brought challenges of potential appropriation and the imposition of Western understandings of health and well-being on Indigenous communities, highlighting instead the need to understand Indigenous health and well-being in the context of their own worldviews. To ensure adequate decision-making when it comes to Indigenous well-being, there is a strong need for intercultural dialogue, reciprocal and equitable processes of participation and prioritisation of actions based on consensus understandings of what it means to be healthy and to achieve well-being to Indigenous Peoples. Theoretical frameworks in this field need to be applicable, adaptable and useful in different contexts, not solely for the recognition of health and well-being problems, but also to inform resources that are available to different Indigenous groups, and the agents that play a key role promoting and maintaining Indigenous health and well-being.
This protocol presents the methods for conducting a review to identify available academic and grey literature relating to conceptual and empirical application of the CA in the field of Indigenous people’s health and well-being. The CA can be a valuable framework as it stresses the multidimensional nature of well-being and places the individual, and their agency to realise the capabilities that they have reason to value, at the centre of human development. Furthermore, it allows for a collective understanding of well-being as it recognises that some freedoms are only available to, and exercisable by, individuals working together as part of a group.50 51 Through an overview and comparison of peer-review and grey literature across different fields, sectors and methodologies, this scoping review will allow us to summarise how capabilities have been applied and measured in Indigenous settings, and whether there are clear CA dimensions which are important to consider. Specifically, we hope that this review will provide valuable information on how different sectors are drawing from the CA to address similar problems in different ways. Ultimately, this can help identify knowledge gaps, inform best practice for intercultural dialogues that adopt the CA framework; research and policy development; resource allocation and contribute to reducing the exclusion and discrimination of Indigenous People.
When developing this protocol, creating a comprehensive list of Indigenous search terms proved challenging as existing lists were incomplete. To address this, it was deemed necessary to carry out an additional focused scoping review to develop a comprehensive list for the South American region. We hope that the steps carried out to do this can be beneficial and informative to those creating similar lists for reviews looking at Indigenous Peoples in other global regions. Our reflections on the approach we have taken will be further reported and discussed in the publication of the findings. Furthermore, some potentially relevant databases have not been included. These decision were made based on resource constraints, and we recognise this as a limitation of the current review.
The findings of this review will be reported to local project partners, published in a peer-reviewed journal and an executive summary will be shared with the Indigenous Peoples HDCA group. Within the wider project in which this review is embedded, the review will be considered alongside primary data to inform the development of tools/approaches of mental health and well-being for the Kankuamo people.
Ethical consideration
This protocol and proposed scoping review do not involve collecting primary data but will be based on previous research conducted within indigenous settings. The protocol has been co-developed with team members from the Universidad Externado de Colombia. The team that will carry out the review includes researchers at the Universidad Externado de Colombia. Due to the nature of the predominately English language journal articles, it has not been possible to directly integrate members of the Kankuamo community into the review team. However, within the wider project in which this review is embedded, findings from this review will be shared for discussion with the Kankuamo Peoples across different points of the scoping review. The results will be used to guide discussion on their relevance and applicability to advancing an intercultural perspective on mental health and well-being in the Kankuamo communities. As such, the current protocol and the proposed scoping review incorporate aspects of community involvement to guide the research process, and we remain attentive to ethical dimensions of equitable coconstruction in the development, conduct and reporting of this review.52
Ethics statements
Patient consent for publication
Acknowledgments
The authors wish to thank Dr. Ruaraidh Hill and Dr. Yenal Dundar, for their time and expertise contributed to the development of the search strategy for this protocol. We would also like to thank Dr. Tiago Canelas for contributing his time to the development of the maps which were included in this protocol.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ivanmol70, @achiumento
Contributors CvdB is first author of the protocol, leading all the stages of the protocol development. Authors CIM-B, AC and RGW supervised the conception and design of the research, the development of the search strategy, selection criteria, the data extraction criteria and the writing of this manuscript. All authors read, edited/commented on and approved the final manuscript.
Funding This research is part of the bilateral UKRI and Newton-Caldas/Minciencias funded project Participatory research to support the development of culturally sensitive mental health and wellbeing services for the Kankuamo people of Colombia (UK identifier: ES/V013416/1).
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.