Article Text

Abstract
Introduction The SaCoVLM is a new type of video intubating laryngeal mask airway (LMA), and it is the first LMA to realise continuous visual monitoring. There is a lack of studies on intubation using the SaCoVLM. The aim of this study is to compare the success rate of intubation with polyvinyl chloride (PVC) tubes and wire-reinforced (WR) tubes using the SaCoVLM.
Methods and analysis This prospective, single-centre, single-blind, parallel-arm, randomised controlled study will be conducted in a tertiary university hospital in China. We will include 104 patients undergoing elective laparoscopic surgery under general anaesthesia. Patients will be randomly assigned to the PVC tracheal tube group (n=52, PVC group) or the WR tracheal tube group (n=52, WR group). The primary outcome is the total success rate of intubation. The secondary outcomes are the first success rate of intubation, the time of tracheal intubation, the site of the first contact, the adjustment action for tracheal intubation, haemodynamic fluctuation during intubation and extubation, incidence of trauma as evidenced by blood, and the incidence rates of postoperative sore throat, hoarseness, and dysphagia.
Ethics and dissemination This study was approved by the Ethics Committee of the First Affiliated Hospital of Shandong First Medical University (YXLL-KY-2022 (008)). All participants will provide written informed consent. The results will be disseminated through peer-reviewed publications and at conferences or congresses.
Trial registration number NCT05338827.
- adult anaesthesia
- accident & emergency medicine
- adult intensive & critical care
- adult surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study provides a rigorous approach to verify the feasibility of tracheal intubation using the SaCoVLM.
This is an adequately powered study on the SaCoVLM that may provide a new strategy for emergency and difficult airway management.
The study will be conducted at a single centre, which may limit the generalisability of the findings.
Only one type of laryngeal mask will be evaluated, so the results cannot be assumed to apply to other kinds of laryngeal masks.
Introduction
The laryngeal mask airway (LMA) occupies a critical position in airway management.1 In anticipated or unanticipated difficult airways, both the American Society of Anesthesiologists (ASA) and Difficult Airway Society recommend the use of an LMA.1 2 The intubating LMA (ILMA) was introduced into clinical use in 1997. It provides not only oxygenation and ventilation for patients, but also tracheal intubation. The ILMA is effective as both a first-line technique and rescue device in various clinical settings.3–5 The Fastrach (Teleflex Medical, Athlone, Ireland) was the earliest ILMA used in the clinic.6 Baskett et al7 proved that the success rate of the first intubation was 79.8%, and the total success rate of the three attempts was 96.2%. Kanazi et al8 showed that the success rate after the first attempt of blind tracheal intubation via an ILMA was 90% with a silicone wire-reinforced (WR) tube, 54% with a Parker tube and 48% with a polyvinyl chloride (PVC) tube, with total success rates of 90%, 86% and 57%, respectively. The development and application of the CTrach (The Laryngeal Mask Company, Singapore) allowed tracheal intubation through the LMA to enter the visualisation era. It has many advantages compared with the Fastrach.9 10 Its purpose is to reduce or avoid damage caused by blind intubation through the LMA.2 11 Liu et al12 reported that the first success rate of the CTrach for intubation was 98.9%, and the total success rate within three intubation attempts was 100%.
Visual anaesthesia technology has become the mainstream of precise anaesthesia, which significantly improves the safety and effectiveness of anaesthesia.13 LMA visualisation is also a development trend going forward.11 Van Zundert et al14 15 discussed the need for vision-guided insertion of supraglottic airway devices (SADs) and described characteristics of the video LMAs. Gómez-Ríos et al16 discussed the physical differences between video laryngeal masks and second-generation LMAs, and their properties in specific clinical settings. The SaCoVLM (Zhejiang UE Medical Corp, Hangzhou, China) was introduced into clinical practice in 2018. It combines a SAD with a videoscope and has the functions of a double-tube LMA and ILMA. It can visualise laryngeal mask placement and tracheal intubation, and can continuously monitor the position of the LMA during the perioperative period. Preliminary reports have confirmed that in morbidly obese patients with a difficult airway, it is safer to insert a laryngeal mask in an awake state and intubate through the SaCoVLM under the condition of good ventilation.17 PVC and WR tubes are currently the two most widely used tubes for tracheal intubations. The PVC tube used is a stiff tube with an anterior curvature of approximately 130°, which retains the additional curvature imposed by its passage through the ventilation conduit of the ILMA. In contrast to the PVC tube, the WR tube is flexible with a slightly anterior curvature. At present, there are no studies on the application of tracheal intubation using the SaCoVLM. Therefore, in this study, we will compare the success rate of intubation between traditional PVC tubes and WR tubes through the SaCoVLM to explore new airway management methods for clinics. We hypothesise that WR tubes have a high success rate of tracheal intubation and a low incidence of airway complications. The primary objective is to compare the total success rate of tracheal intubation with a PVC tube with a WR tube using the SaCoVLM in patients undergoing elective laparoscopic surgery. The secondary objective is to compare the clinical performance and airway complications of the two tracheal tubes.
Methods and analysis
Study design and setting
This is a prospective, single-centre, single-blind, parallel-arm, randomised controlled study. The study, which was registered with ClinicalTrials.gov (NCT05338827) prior to recruiting patients, will be conducted in a tertiary university hospital in China (the First Affiliated Hospital of Shandong First Medical University). The study will begin on 1 May 2022 and is expected to be completed within a year. This study protocol is reported in accordance with the Standard Protocol Items: Recommendations for Interventional Trials statement,18 and the Consolidated Standards of Reporting Trials statement will be used to guide reporting of the trial results.
Participants and recruitment
From 1 May 2022 to 1 May 2023, patients who will undergo elective laparoscopic surgery will be notified of the trial by the clinical research coordinator the day before surgery. Patients who are interested in participating will be regarded as potential subjects and their basic information will be recorded. Potential subjects will be interviewed by a clinical study coordinator to assess whether they meet the inclusion and exclusion criteria. Eligible patients will voluntarily provide written informed consent before randomisation. After recruitment, the patients will be randomised to either the PVC or WR group in a 1:1 ratio (figure 1).

Study flow chart. PVC, polyvinyl chloride; WR, wire-reinforced.
Eligibility criteria
The inclusion criteria are as follows:
Scheduled to accept elective laparoscopic surgery under general anaesthesia.
Aged 18–70 years.
Body mass index (BMI) 18.5–27.9 kg/m2.
ASA class I–III.
The exclusion criteria are as follows:
Neurological or psychiatric diseases (such as schizophrenia and depression), or unconscious.
Severe cardiopulmonary dysfunction.
Vocal cord injury, pharyngeal disease or history of neck surgery.
Risk of reflux aspiration and indwelling nasogastric tube before and after surgery.
Mouth opening less than 2 cm, limitation of cervical extension, modified Mallampati score IV.
SaCoVLM glottic exposure grade 3 or 4.
Participated in other clinical studies during the last 3 months.
Refused to give informed consent for the clinical study.
Intervention
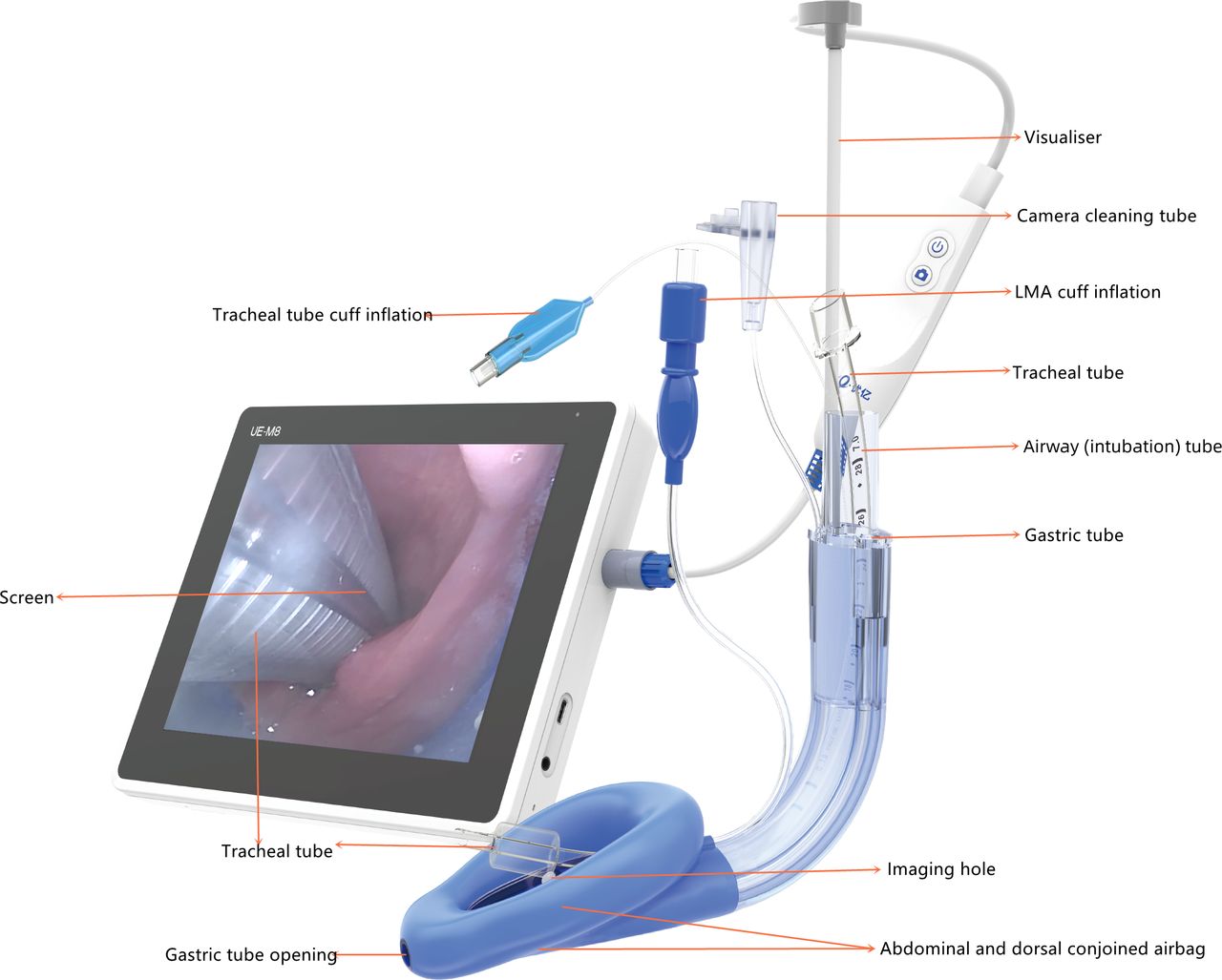
The SaCoVLM is shown in figure 2. The appropriately sized LMA and tracheal tube (PVC tracheal tube, Covidien, Medtronic, Dublin, Ireland; WR tracheal tube, Henan Camel Medical Device Group Co, Zhengzhou, China) will be used based on the weight of the patient and the discretion of the attending anaesthesiologist. A size 3 LMA with 7# tracheal tube will be used for patients weighing 30–50 kg, a size 4 LMA with 7.5# tracheal tube for patients weighing 50–70 kg, and a size 5 LMA with 8# tracheal tube for patients weighing 70–90 kg.
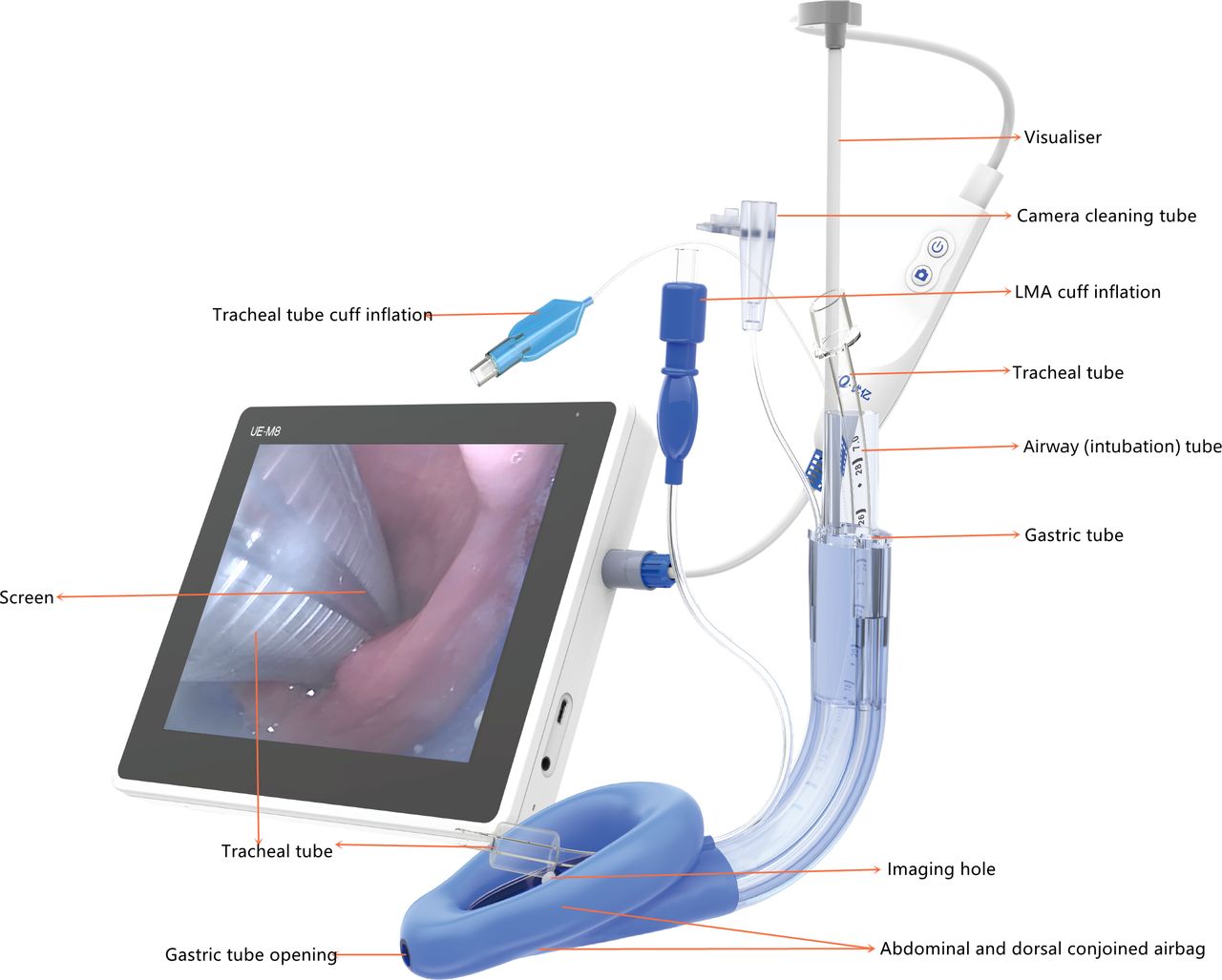
SaCoVLM video intubating laryngeal mask airway (LMA). Photo courtesy of Zhejiang UE Medical Corp (Hangzhou, China).
All patients will be routinely monitored for continuous ECG, heart rate (HR), non-invasive blood pressure, oxygen saturation, bispectral index (BIS) and neuromuscular monitoring using a train of four (TOF). To facilitate the placement of the laryngeal mask and subsequent endotracheal tube, the cuff will be deflated and plastic. The videoscope will be inserted into the visual channel and connected to a screen before use. The posterior side of the laryngeal mask and tracheal tube will be lubricated with water-soluble jelly.
After sufficient preoxygenation, anaesthesia will be induced with intravenous midazolam (0.05 mg/kg), propofol (2.5 mg/kg), rocuronium (0.6 mg/kg) and sufentanil (0.3–0.5 µg/kg). When the TOF count is 0 and the BIS is below 60, the patient will be placed in the supine position without a pillow. An anaesthesiologist, who had performed at least 100 tracheal intubations using the device before this evaluation, will hold the distal end of the laryngeal mask and allow it to slide down along the midline in the mouth, slide the anterior end of the capsule down along the upper palate to the arytenoid cartilage and the posterior commissure, and continue to push the anterior part of the capsule to the back of the arytenoid cartilage until the arytenoid cartilage and the glottic structure behind it can be seen in the visual field. A handheld manometer (Covidien) will be used to inject gas into the cuff to achieve a maximum cuff pressure of 40 cmH2O. The SaCoVLM will be connected to the anaesthetic ventilator and adjusted to manual ventilation mode to squeeze the airbag to observe chest fluctuations. If the display screen shows a clear glottic structure and when squeezing the airbag, the ventilation resistance is small, the thoracic fluctuation is good and regular normal end-expiratory carbon dioxide waveforms appear, indicating that the position of the SaCoVLM is good. If the SaCoVLM is poorly aligned and ventilated, one or more of the up-down manoeuvre, raising the jaw with both hands, the Chandy manoeuvre,5 cervical flexion or extension manipulation will be used to adjust the position of the LMA to obtain the best ventilation. If optimal ventilation is still not achieved after three LMA insertions and after longer than 120 s, tracheal intubation will be performed using video laryngoscopy.
The anaesthesiologist will perform a visual screen for the SaCoVLM glottic exposure grade after the SaCoVLM is successfully inserted. The SaCoVLM glottic exposure grade was referred to the endoscopic view grading system (grade 1: entire glottis aperture, grade 2: partial glottis aperture, grade 3: free edge or lingual face of the epiglottis, and grade 4: no recognisable structure or whiteout screen).19 The SaCoVLM view of the laryngeal structure will be graded according to the criteria listed in figure 3. If the SaCoVLM glottic exposure grade is 3 or 4, and if a slight adjustment of the SaCoVLM position using the techniques described above cannot change the grade to 1 or 2, this case will be excluded. If the SaCoVLM glottic exposure grade is 1 or 2, a lubricated tracheal tube will be inserted in a conventional manner with the curvature of the tracheal tube aligned along the intrinsic curvature of the SaCoVLM. The passage of the tracheal tube into the glottis will be visualised. If there is a discrepancy in the alignment of the tracheal tube exiting from the SaCoVLM and the glottis that will prevent the passage of the tracheal tube into the glottis, the tracheal tube will be withdrawn and manipulations (rotation of the tracheal tube or up/down manoeuvre) will be performed in an attempt to align the glottis and tracheal tube tip to facilitate intubation. Such manoeuvres, if performed, will be recorded. An intubation attempt is defined as the tracheal tube exiting from the cuff of the SaCoVLM and passing into the glottic opening or hitching against any of the laryngeal structures necessitating withdrawal of the tracheal tube through the SaCoVLM and requiring manipulation. After the tracheal tube is successfully inserted, the pressure of the endotracheal tube cuff will be adjusted to 25 cmH2O. If the cumulative number of tracheal intubation attempts is more than 320 and the time is longer than 120 s, the intubation will be considered as failed and tracheal intubation will be guided by a fibreoptic bronchoscope.

{kind=link}
{kind=link}
{kind=link}
SaCoVLM glottic exposure grades. LMA, laryngeal mask airway.
Anaesthesia will be maintained with a target-controlled infusion of propofol (2–4 µg/mL) and remifentanil (3–5 ng/mL), with a BIS target range of 40–60. Sufentanil will be added as needed and rocuronium (0.15 mg/kg) will be added when the TOF count is 1. The endotracheal tube will be removed at the end of the surgery, and the LMA will be removed after recovery of spontaneous breathing and opening of the eyes.
Outcome measurements
The primary outcome is the total success rate of tracheal intubation, defined as the cumulative third-attempt intubation success rate. The secondary outcomes include the following variables:
Successful insertion rate on the first attempt: tracheal intubation is considered successful if the endotracheal tube slides through the LMA without any resistance, and tracheal intubation was confirmed by the laryngeal mask visual screen and detection of end-tidal carbon dioxide (CO2).
Time of tracheal intubation: defined as the time from picking up the tracheal tube to the appearance of three standard end-tidal CO2 waveforms on the monitor.
Site of first contact of tracheal intubation, which will be identified with the SaCoVLM visual screen (four areas are defined based on the glottic opening: the interarytenoid fold, the left and right aryepiglottic, the vestibular and vocal folds, and the tubercle of the epiglottis).8
Adjustment action for tracheal intubation: if tracheal intubation is unsuccessful after the first attempt, the tube will be pulled 2 cm, rotated and then advanced. If this attempt is unsuccessful, the tube will again be pulled 2 cm, adjusted to the SaCoVLM by the up-down manoeuvre, rotated and then advanced. If tracheal intubation is accomplished after either manoeuvre, this is considered a success and the manoeuvre used would be documented.
Haemodynamic fluctuation: the systolic and diastolic blood pressure, mean arterial pressure and HR after induction, immediately, and 3 min after insertion of the laryngeal mask; immediately and 3 min after tracheal intubation; 3 min before extubation; and immediately and 3 min after extubation are recorded.
Incidence of trauma as evidenced by blood on ILMA or endotracheal tube after removal.
Incidence rate of postoperative sore throat, hoarseness and dysphagia at 24 hours after the surgery: the severity of sore throat will be evaluated using a numerical rating scale (0=no sore throat, 10=worst sore throat imaginable).21 22 Hoarseness will be classified as mild, moderate or severe (overall dysphonia grade, roughness, breathiness, asthenia and strain score).23 Dysphagia will be classified as normal, mild, moderate or severe according to the severity.
Data collection
Demographics.
Patient (age, sex, BMI, ASA class).
Airway examination (mouth opening, thyromental distance, neck circumference, modified Mallampati score).
Related records of LMA (SaCoVLM glottic exposure grade, time of laryngeal mask insertion, number of attempts to insert laryngeal mask).
Participant timeline
After recruitment, from the beginning of the induction of general anaesthesia to the end of the surgery, all relevant variables will be recorded by an independent investigator, who will follow up at 24 hours after the surgery to assess the success rate of intubation and the time of tracheal intubation (table 1).
SPIRIT flow diagram: schedule of enrolment, interventions and assessments
Sample size calculation
The sample size was calculated based on the total intubation success rate. According to previous reports, the success rates of the PVC and WR groups were expected to be 57% and 86%, respectively.8 Using PASS software (V.15.0; NCSS, Kaysville, Utah, USA) to compare the sample size of the two groups, the sample size ratio was set at 1:1, and a sample size of 46 in each group was needed to achieve 90% power with an alpha value of 0.025. Anticipating a 10% dropout rate, we plan to enrol 52 patients per group. A minimum of 104 subjects will be included in the study.
Randomisation and blinding
After recruitment, the patients will be randomised to either the PVC or WR group in a 1:1 ratio. Block randomisation with a block size of four will be used for allocation. Randomisation will be conducted using a web-based randomisation system (GraphPad Software, San Diego, California, USA) by an independent investigator with no contact with the participants or researchers. If a participant is found ineligible for the study after randomisation, the original assignment will be reassigned to the next eligible subject. Clinicians and intraoperative data-recording investigators will not be blinded to the randomisation assignment. Participants, postoperative follow-up investigators and data staff responsible for data entry will be blinded to the randomisation assignment.
Data collection and management
The study data will be recorded using a specific case report form (CRF). Before measurement, data from each patient will be collected by the study personnel. All outcome measurements will be recorded during and after CRF evaluation. Each allocated subject will be coded according to a specific number of patients. After the measurements are completed, the study data will be entered into a unique Microsoft Excel file (Microsoft, Redmond, Washington, USA).
Statistical analysis
Intention-to-treat and per-protocol analyses will be performed. After testing the normality assumption using the Kolmogorov-Smirnov test, continuous variables will be expressed as mean and SD or median and IQR. Categorical variables will be expressed as numbers of patients and proportions.
All statistical data analyses will be performed using SPSS software (V.25; IBM). We will conduct χ2 analysis or Fisher’s exact test for the primary outcome. For secondary outcomes, continuous variables will be examined using an independent-samples t-test or the Mann-Whitney U test, and categorical variables will be examined using Pearson’s χ2 test or Fisher’s exact test. All tests are two sided, and statistical significance is set at p<0.05. A statistician who is not involved in data collection will conduct all statistics.
Data monitoring
Prior to patient enrolment, the study physicians and clinical research assistants will be involved in the study protocol and data collection in CRFs. Due to the relatively small number of patients in each group, we will not have a formal data monitoring committee. All data will be kept confidential. Original data will be recorded using CRFs and completed CRFs will be checked by a study coordinator qualified by the principal investigator.
Safety assessments
The study may be temporarily stopped for an individual patient at the discretion of the attending physician in case of major serious adverse events suspected to be associated with the LMA and tracheal tube used. An adverse event or suspected adverse reaction will be considered serious if, in the view of either the investigator or sponsor, it results in any of the following outcomes: death, life-threatening adverse event, inpatient hospitalisation or prolongation of existing hospitalisation, persistent or significant incapacity, or substantial disruption of the ability to conduct normal life functions.
Severe adverse events (SAEs) will be reported by the Ethics Committee. SAEs will include cardiac arrest, acute circulatory failure, death and vocal cord injury when they occur as a result of airway manipulation. No specific procedure for reporting unexpected SAEs has been planned. Appropriate actions, including medical attention, should be taken if and when necessary.
Trial status
At the time of manuscript submission, patient recruitment is underway and is ongoing.
Patient and public involvement
None.
Ethics and dissemination
Research ethics approval
This protocol was approved by the Ethics Committee of the First Affiliated Hospital of Shandong First Medical University (YXLL-KY-2022 (008)).
Consent
Prior to the study, patients must provide written consent after the possible consequences of the clinical study are explained in an understandable way (see online supplemental document). All documents must be written in Chinese and comprehensible. The patient will receive a copy of signed patient information and provide informed consent. Participants may withdraw at any time during the trial at their own request or from their legal representatives.
Supplemental material
Dissemination
The results will be disseminated through peer-reviewed publications and at conferences or congresses.
Discussion
Airway management has always occupied a very important position in anaesthesia, especially difficult airway is often urgent and is accompanied by serious adverse consequences. At present, difficult airway cannot be predicted quickly and effectively.24
When we face the failure of laryngoscope intubation in the clinic, an SAD can be placed to ensure ventilation and oxygenation, followed by endotracheal intubation via the SAD.2 The CTrach is the world’s first video ILMA and was applied in clinical practice in 2004. At present, there have been various studies to verify the success rate of intubation.12 25 The TotalTrack (Medcom Flow, Barcelona, Spain) is another video ILMA. Studies have verified that the success rate of the TotalTrack intubation for the first time was 85%, and the total success rate within three intubation attempts was 94%,26 particularly in super-obese patients, which could better display the larynx and provide effective ventilation and further tracheal intubation.27 The TotalTrack seems to be an effective first-line technology and rescue device in various clinical environments.28–31
The SaCoVLM has shown advantages in clinical applications since its creation in 2018.32 The SaCoVLM is comparable in price with a common LMA and can easily be clinically promoted, allowing visualisation of the conditions around the glottis and thus achieving rapid and accurate insertion. Additionally, the operator can visualise the passage of the tracheal tube through the glottis during intubation. During anaesthesia maintenance, the condition around the glottis can be constantly monitored. However, to our knowledge, there is a lack of studies on tracheal intubation through the SaCoVLM.
This prospective, single-centre, single-blind, parallel-arm, randomised controlled study aims to compare a PVC tube with a WR tube for tracheal intubation using the SaCoVLM. This study is designed to provide a rigorous approach to validate the feasibility of tracheal intubation using the SaCoVLM. Unfortunately, there are several noteworthy limitations of this study. First, it would be difficult to eliminate bias with the current research set-up in the hospital. Selection bias will be present as a consecutive series of patients will not be approached due to insufficient personal resources. Second, the study will be conducted at a single centre, which may limit the generalisability of the findings. Third, only one type of laryngeal mask will be evaluated; therefore, the results cannot be transferred to other kinds of laryngeal masks.
This study aims to explore the best type of tracheal tube by observing the success rate of intubation using the SaCoVLM and the incidence of postoperative adverse reactions. By observing the optimised operation which can improve the success rate of tracheal intubation, this study will provide a reference for the clinical application of the SaCoVLM under general anaesthesia. We believe that tracheal intubation through video laryngeal mask may play an increasingly important role in the future.
Ethics statements
Patient consent for publication
Acknowledgments
The authors wish to thank all anaesthesiologists from the study sites for their great efforts and support for this trial.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it was first published. Author affiliations have been updated.
Contributors YS and YW are the principal investigators of this study and obtained grant funding. ZG, YG and YS designed the study protocol, drafted the protocol and wrote the manuscript. YS and YW refined the study protocol. ZG, XG, WW, MJL, LC, YL and XZ assist with the development and implementation of the study. MZ will supervise the study. All authors have reviewed and approved the final manuscript.
Funding This work was supported by the Academic Promotion Programme of Shandong First Medical University (2019QL015), Natural Science Foundation of Shandong Province (ZR20201MH358), Shandong Provincial Medical Association Analgesia and Anesthesia Optimization Research Project (YXH2021ZX039).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.