Article Text

Abstract
Introduction Ankyloglossia is a situation where the tongue tip cannot go beyond the mandibular incisor because the frenulum linguae is short. It could affect children’s health by interfering with their ability to talk, breast feeding and dental development. The most effective measure to control ankyloglossia is the surgical method. However, which surgical procedure is the best one is still controversial. Thus, this protocol aims to assess the effectiveness of different surgical interventions in children with ankyloglossia.
Methods and analysis PubMed, EMBASE, Cochrane Library, Web of Science and OVID will be searched for relevant information from inception to 31 May 2022. Observational studies in English that investigate the association between surgical methods and ankyloglossia will be included in this protocol. This protocol follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols. The Critical Appraisal Checklist for Analytical Cross-Sectional Studies and the Newcastle–Ottawa Quality Assessment Scale for longitudinal studies will be used to assess the included studies. The improvement of breast feeding and nipple pain will be the primary outcome. STATA V.15.1 will do the statistical analysis in the meta-analysis. Subgroup and meta-regression will be carried out based on the characteristics of included studies.
Ethics and dissemination This systematic review and meta-analysis will summarise relevant information on the effects of different surgical treatments on patients with ankyloglossia. The results will be disseminated through peer-reviewed publications. The data included in this study will be extracted from the published original studies. Thus, ethical approval and informed consent will not be required.
PROSPERO registration number CRD42022323350.
- ORAL MEDICINE
- ORAL & MAXILLOFACIAL SURGERY
- Paediatric oral & maxillofacial surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This protocol provides a systematic review and meta-analysis only based on studies in English.
This study could be limited by insufficient studies regarding the different surgical methods in ankyloglossia treatment.
This study will provide a comprehensive assessment concerning the effect of different surgical treatments on children with ankyloglossia.
Introduction
In the 1960s, ‘ankyloglossia’ was first used in the medical field by Wallace,1 who regarded tongue-tie as a situation where the tongue tip cannot go beyond the mandibular incisor because the frenulum linguae is short. Ankyloglossia is traditionally described as a frenulum near the tongue tip. In recent years, attention has transferred from definitions based on anatomy frenulum attachment alone to a more comprehensive and functional focus on symptoms led by the frenulum.2 It has long been concern by clinical practitioners that ankyloglossia may harm children’s health by interfering with their ability to speak, oral hygiene, dental development, breast feeding or ability to perform social skills.3 4 There are lots of surgical treatments used to inhibit the severe symptom.
The conventional frenulum, a simple procedure that releases the lingual frenulum with scissors,5 seemed to be the first surgical procedure that helps to relieve severe symptoms. Some published studies found that the conventional frenulum contributes to improving breast feeding.6 7 With the rapid development of the laser, different kinds of laser with various lengths became available in ankyloglossia.8 9 Laser-assisted surgeries in tongue-tie were proven to be safe, simple and comfortable.10 In addition, various surgical procedures tend to be effective, such as straight cut of the frenulum, complete removal of the frenulum, Z-plasty and so on.11 However, it is evident that choosing which method is suitable primarily depends on the severity of ankyloglossia. Then controversies occur, whether laser should used, which type of laser to be used, which surgical procedure should be used and other questions are considered.
Thus, this protocol aims to offer a transparent methodology to synthesise the results of different surgical treatments for ankyloglossia in the paediatric population.
Objective
This systematic review and meta-analysis will provide the latest comprehensiveness of the effects of different surgical treatments on children with ankyloglossia.
Methods and analysis
This review has been registered in PROSPERO. In addition, this systematic review and meta-analysis will follow the PRISMA-P (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols) statement12 and the Cochrane Collaboration Handbook.13
Patient and public involvement
No patients or members of the public will be included in this study. However, if our research is accepted as a scientific report, it will be spread through social networks. In this way, our conclusions will affect the surgical treatment of ankyloglossia in the paediatric population.
Inclusion/exclusion criteria
For this protocol, studies regarding the links between different surgical treatments and ankyloglossia in kids, which accord with all inclusion criteria, will be included in this review.
Inclusion criteria: (1) children aged 0–18 years old; (2) participants diagnosed with ankyloglossia; (3) exposure: different surgical treatments or methods; (4) outcomes: various subjective and objective assessments of function and morphology (articulation test, tongue protrusion, breast feeding) and adverse effects (bleeding, pain, infection); (5) randomised controlled trials or non-randomised experimental studies; (6) studies written in English and published before April 2022.
Exclusion criteria: (1) including only participants aged older than 18 years old; (2) including only the surgical treatment group but no control group; (3) including only speech training without surgical procedure.
Search strategy
The electronic search will be limited to keywords, abstracts and titles. Literature searches will be conducted through the EMBASE, Cochrane Library, PubMed, Web of Science and OVID from inception to 31 May 2022. In addition, experienced researchers will also search references from relevant trials and reviews.
The following search terms will be combined: ‘Ankyloglossia’, ‘Tongue Tie’, ‘Tongue Ties’, ‘Partial Ankyloglossia’, ‘Ankyloglossia, Partial’, ‘Ankyloglossias, Partial’. The precise search strategy can be seen in the online supplemental material 1. Previous similar studies will be screened to identify additional sources. The search strategy will follow free-text accessible Medical Subject Heading terms in the case of PubMed.
Supplemental material
Selection of studies and data extraction
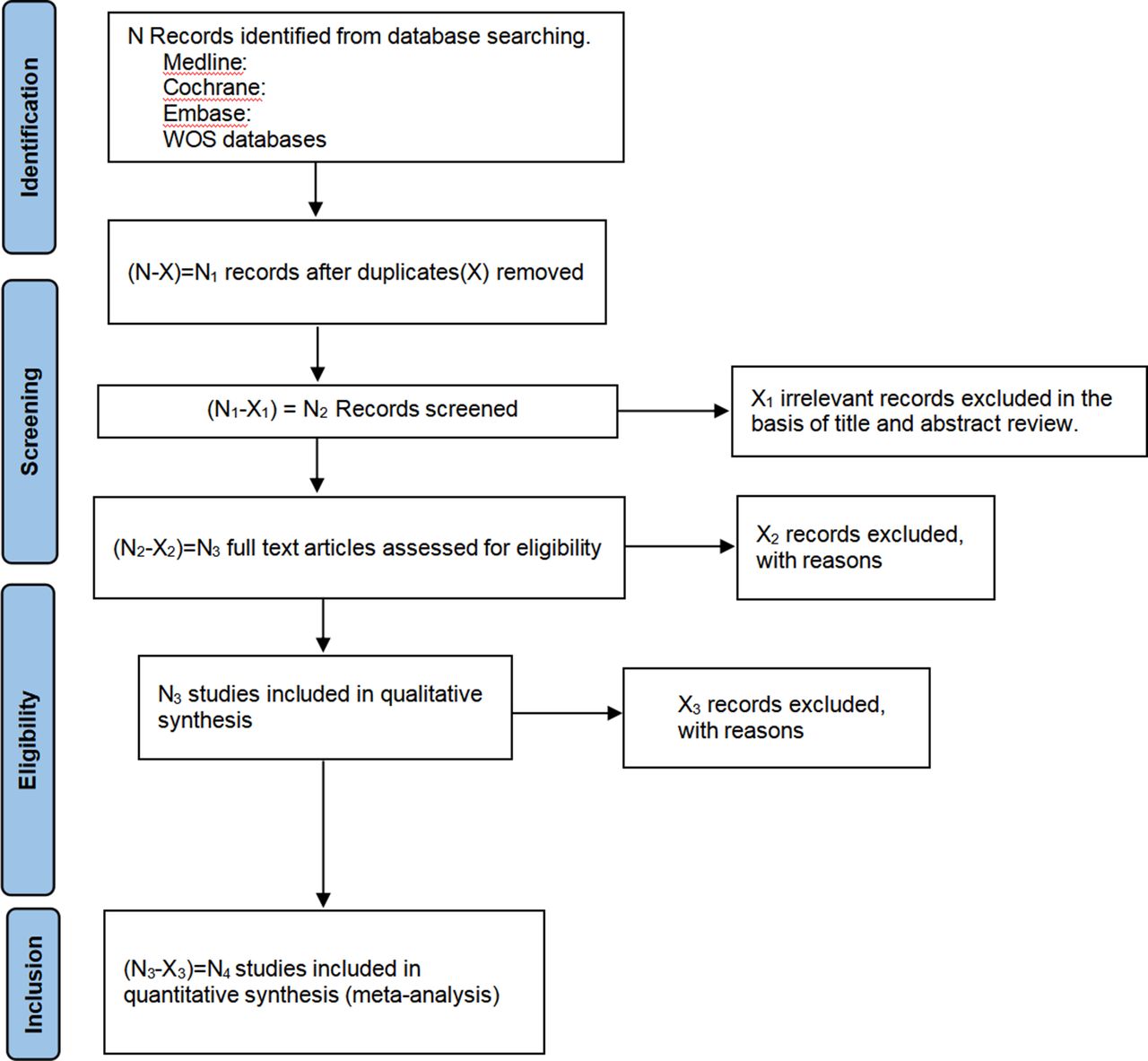
Relevant titles and abstracts of the included publications will be screened independently by two reviewers to identify qualified studies for this systematic review. Any disagreements between them will be settled with the aid of the third reviewer. According to the inclusion and exclusion criteria, the article that does not meet the eligibility criteria will be excluded. The progress of identification, screening and including/excluding articles will be shown using the PRISMA flow chart (figure 1).

{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of identification, screening, eligibility and inclusion of studies.
Finally, full texts of the included studies will be extracted, with the following data: (1) author’s name, (2) publication year, (3) country, (4) study design, (5) number of participants in each study, (6) surgical procedure, (7) outcome assessment (table 1).
Characteristics of studies included in the systematic review and/or meta-analysis
Assessment of risk of bias
Two researchers will be blinded to the authors, titles and years of publication of the included studies; after that, they will evaluate the quality of the included studies. Then, the Critical Appraisal Checklist for Analytical Cross-Sectional Studies from the Joanna Briggs Institute will be used to assess the quality of cross-sectional studies.14 It consists of eight items that could be scored as ‘yes’, ‘no’, ‘unclear’ or ‘not applicable’.
The Newcastle–Ottawa Quality Assessment Scale15 will be used to assess the quality of longitudinal studies, which involve case–control and cohort studies. This tool includes eight items, which could be grouped into three categories: (1) selection, (2) comparability, (3) exposure 75% or outcome (for case–control and cohort studies, respectively). Each study can obtain one star for one item within the selection and exposure categories and a maximum of two stars in the comparability category.
Any disagreements during the assessment of quality will be resolved by a consensus. A third viewer will be required if an agreement is not reached.
Statistical analysis
Reviewers will summarise the main characteristics via table 1; correlational research’s features and population description will be involved. After data extraction, it will be determined whether a meta-analysis is possible. If possible, STATA V.15.1 software will be used to compute the pooled mean differences with 95% CIs. A fixed-effects model will be used if there is no evidence of heterogeneity. Otherwise, a random-effects model will be used.
The heterogeneity of results will be evaluated by calculating the I2 statistic. The values of I2 will be considered as: not significant (0%–40%), moderate (30%–60%), substantial (50%–90%) and considerable (75%–100%); the corresponding p values will also be in consideration. In addition, publication bias will be evaluated using a funnel plot based on the method proposed by Egger et al.16 Finally, if a meta-analysis is not feasible, a narrative synthesis will be conducted.
Subgroup analyses and meta-regression
Subgroup analyses and meta-regression will be put into practice, considering the factors that cause heterogeneity, such as age (children aged 0–18 years), country of study participants, different surgical treatments (laser, frenotomy), type of intervention (only surgical treatment or combined with speech training) and kind of pain scoring after surgical procedure (Visual Analogue Scale, Numerical Rating Scale). In addition, the methodological quality will be evaluated for extra subgroup analyses.
Sensitivity analyses
Sensitivity analyses will be conducted by removing the included studies to assess the robustness of summary estimates.
Discussion
The objective of this study was to present a different technology to implement a systematic review and meta-analysis exploring the effects of different surgical treatments on ankyloglossia in the paediatric population.
Many studies have investigated different surgical methods in reducing severe symptoms of ankyloglossia.11 17–20 Obviously, conventional frenotomy could contribute to reducing symptoms of ankyloglossia when compared with no surgical frenotomy.21–24 A study reported that Z-plasty with genioglossus myotomy could improve tongue mobility and articulation. Still, no control group is mentioned.11 So there is a lack of adequate evidence to conclude that Z-plasty with genioglossus is one particular method that is much better than the others. One study mentioned frenectomy with rhomboid plasty,25 but this study is indeed just a protocol. Thus, more convincing research should be conducted to assess the effectiveness of this method. Heller et al found that in patients with ankyloglossia who underwent surgical correction via four-flap Z-frenuloplasty, it was found that it was superior to the more traditional horizontal-to-vertical frenuloplasty.19 But when taking the sample size into account, different groups do not own the similar sample size, with 11 patients in the four-flap Z-frenuloplasty group and five patients in the traditional group. As a result, original articles with a similar and more significant sample size are needed to compare these two methods. Besides, several studies believed that laser could improve severe symptoms of ankyloglossia,10 26 27 but the application of laser that could be used to assist surgical procedures still needs more clinical trials.
Thus, a suitable systematic review and meta-analysis will help us obtain an overview of current literature regarding the study subject. In the meantime, this systematic review and meta-analysis could contribute to the development of discussions regarding the benefits of surgical interventions on ankyloglossia.
To achieve this goal, this protocol provides a clear and easy structure for the extraction and synthesis of relevant data. This could offer evidence regarding surgical interventions that are most beneficial for reducing severe symptoms from ankyloglossia in the paediatric population.
Another issue that should be emphasised when conducting this systematic review and meta-analysis is the potential limitation of this study. It includes publication bias, information bias, the inclusion of articles in English only, poor statistical analysis and inadequate reporting of methods. To conquer these limitations, this systematic review will be accomplished by two independent reviewers. If disagreement appears in data collection, the third reviewer will be consulted.
Furthermore, when studies regarded articulation tests as an outcome after surgical intervention in children with ankyloglossia, whether linguistic training is used should be considered because it may lead to different results.28 This systematic review only aimed to find out the effects of different surgical procedures on ankyloglossia in the paediatric population, so other variates should be controlled.
In summary, a clinical guideline should be developed for practitioners when confronted with children or infants with ankyloglossia; at the same time, the quality and quantity of existing studies are not sufficient to create a clinical practice guideline.3 So, it is logical and significant to conduct a systematic review and meta-analysis.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CY and ZZ designed the study, CY was the primary investigator. Q-QL, S-LC and R-ZZ were the main coordinators of this study. F-FX and S-LC gave the statistical support for this study. CY wrote the article with the support of Q-QL and ZZ. All authors reviewed and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.