Article Text

Abstract
Introduction The COVID-19 pandemic has caused disruptions in access to routine healthcare services worldwide, with a particularly high impact on chronic care patients and low and middle-income countries. In this study, we used routinely collected electronic medical records data to assess the impact of the COVID-19 pandemic on access to cancer care at the Butaro Cancer Center of Excellence (BCCOE) in rural Rwanda.
Methods We conducted a retrospective time-series study among all Rwandan patients who received cancer care at the BCCOE between 1 January 2016 and 31 July 2021. The primary outcomes of interest included a comparison of the number of patients who were predicted based on time-series models of pre-COVID-19 trends versus the actual number of patients who presented during the COVID-19 period (between March 2020 and July 2021) across four key indicators: the number of new patients, number of scheduled appointments, number of clinical visits attended and the proportion of scheduled appointments completed on time.
Results In total, 8970 patients (7140 patients enrolled before COVID-19 and 1830 patients enrolled during COVID-19) were included in this study. During the COVID-19 period, enrolment of new patients dropped by 21.7% (95% prediction interval (PI): −31.3%, −11.7%) compared with the pre-COVID-19 period. Similarly, the number of clinical visits was 25.0% (95% PI: −31.1%, −19.1%) lower than expected and the proportion of scheduled visits completed on time was 27.9% (95% PI: −39.8%, −14.1%) lower than expected. However, the number of scheduled visits did not deviate significantly from expected.
Conclusion Although scheduling procedures for visits continued as expected, our findings reveal that the COVID-19 pandemic interrupted patients’ ability to access cancer care and attend scheduled appointments at the BCCOE. This interruption in care suggests delayed diagnosis and loss to follow-up, potentially resulting in a higher rate of negative health outcomes among cancer patients in Rwanda.
- COVID-19
- epidemiology
- international health services
Data availability statement
Data are available upon reasonable request. Data may be made available to reasonable requests sent to the authorship team, as any data sharing must follow existing health data sharing guidelines by Partners In Health/Inshuti Mu Buzima and Rwanda Ministry of Health.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
We used time-series modelling to assess the impact of COVID-19 on cancer care, which has not yet been studied in Rwanda, at the main cancer treatment centre in the nation.
We used over 4 years of baseline data to generate time-series models that provide quantitative estimates of both monthly and cumulative drops in cancer services throughout the pandemic.
We compared the results between indicators at multiple steps of patient flow through cancer care during the pandemic.
We were limited by the use of electronic medical records data, which suffer from some incompleteness for certain indicators, reducing our ability to analyse factors such as cancer type.
Our analysis did not incorporate data on social policies, such as COVID-19-related campaigns, to change cancer care or patient behaviour.
Introduction
In 2020, an estimated 19.3 million people in the world were newly diagnosed with cancer and nearly 10 million cancer deaths occurred.1 Although cancer is a global public health concern, cancer incidence and mortality rates are increasing in low and middle-income countries (LMICs), while rates in high-income countries are plateauing or decreasing due to enhanced screening, early detection and improved treatments.2 3 Screening and early detection of cancer as well as early treatment can increase chances of survival and less morbidity. However, the capacity to diagnose cancer is scarce in LMICs given that many hospitals and health clinics are not equipped with the adequate medical equipment or laboratories to diagnose cancer.3 4 Consequently, most people living in LMICs are not diagnosed until their cancer is on advanced stage.5 Individuals with treatable cancer must receive treatment at dedicated comprehensive cancer centres, which are scarce and may be costly and far from their home.6 Further, cancer management requires long-term treatment and adherence to follow-up care visits, but loss to follow-up remains a major issue in LMICs.7
In addition, the COVID-19 pandemic, which emerged in early 2020, caused major disruptions in access to routine healthcare services worldwide.8 9 As many countries responded to the spread of the disease, the delivery of non-COVID-19-related health services was adversely impacted due to resource constraints and lockdown measures.10 Disruption of cancer services during the COVID-19 pandemic has also been documented, consisting of a reduction in patient visits for different cancer clinical procedures—most notably diagnosis and staging procedures such as biopsy, imaging and CT scanning, and treatment procedures such as chemotherapy and surgery.11–14 Most of these studies have been in high-income countries. However, one survey among cancer providers in Africa found staff shortages, treatment delays and reduced patient volume during the first months of the pandemic in 2020.10 These COVID-19-related disruptions in care for diseases that require timely diagnosis, treatment and monitoring, such as cancer, may result in excess mortality and morbidity.15
The first cancer centre in Rwanda—the Butaro Cancer Center of Excellence (BCCOE)—was established in 2012 in a partnership between the non-governmental international organisation Partners In Health/Inshuti Mu Buzima (PIH/IMB) and the Rwanda Ministry of Health. The BCCOE is located in Burera, a rural district in northern Rwanda, and provides cancer care services, including pathology-based diagnosis, basic imaging, chemotherapy and surgery, to patients with cancer from across Rwanda and a small proportion of patients from neighbouring countries, such as the Democratic Republic of Congo and Burundi.16 During the COVID-19 pandemic, the BCCOE has implemented ad hoc strategies to ensure the continuity of cancer service delivery to the patients amid COVID-19 lockdowns. These strategies have included some patients being transferred to a satellite infusion centre unit at the Rwanda Cancer Center (RCC) in Kigali City for intravenous, oral therapy and follow-up care, delivery of oral chemotherapy drugs to patients in their near geographical proximity using drones10 and provision of social and food support to vulnerable patients with cancer.17 However, these strategies only supported patients in need of chemotherapy and radiotherapy, and did not address gaps in screening, new diagnoses or other ongoing treatments for patients with cancer. Among the existing studies on the impact of COVID-19 on health services in Rwanda,18–20 no studies have shown the impact of COVID-19 on cancer care patients. In this study, we use time-series modelling to assess the impact of the COVID-19 pandemic on cancer care services among patients seeking cancer care in Rwanda.
Methods
Study setting
The BCCOE is located in the Northern Province of Rwanda in the rural Burera district and was the first cancer referral centre in the area. In its early years, BCCOE provided clinical diagnosis with the support of the Brigham and Women’s Hospital (USA) for cancer confirmation. The capacity for cancer diagnosis and treatment has grown such that BCCOE now provides the majority of the cancer care in Rwanda, with the exception of radiotherapy, which is provided at the RCC. The RCC opened in February 2020 at the Rwanda Military Hospital in the capital city of Kigali. New patients at the BCCOE are usually referred from district and referral hospitals, private clinics across Rwanda or transferred from outside Rwanda (figure 1). The most common cancers diagnosed at BCCOE are breast and cervical cancers among adults and Wilms tumour and leukaemia among paediatrics.17 21 In addition, the BCCOE provides socioeconomic support to patients in need, including meals, transport and accommodation. Enrolment in the cancer care programme occurs at the first in-person presentation to the BCCOE from the referral health facility, and then clinical consultation is conducted for cancer diagnosis. When the clinical consultation outcome indicates that the patient does not have cancer, she is discharged from the programme. Patients with cancer may end up being hospitalised or treated in the outpatient mode based on the stage of their disease and type of treatment needed. For follow-up care visits in the outpatient clinic, clinical visits are prescheduled with the frequency of visit varying from patient to patient depending on the treatment plan; however, unscheduled visits for existing patients do also happen for emergency care.

Flow chart of new patients at the Butaro Cancer Center of Excellence during the COVID-19 pandemic. F/U, follow-up; IV, intravenous; PO, peroral.
Study design and population
We conducted a time-series study using retrospective data from the electronic medical records (EMR) system at the BCCOE. We only included patients who received cancer care at the BCCOE from 1 January 2016 to 31 July 2021. We defined the baseline (ie, period before the COVID-19 pandemic in Rwanda) period starting from 1 January 2016, as we anticipated a low quality of EMR data collected before 2016. In the early years of the implementation of EMR for routinely collecting data on cancer care at the BCCOE, data were more vulnerable to incompleteness due to the delays and errors in the process of transcribing data from paper into EMR by data officers. During the chosen study period, most of the data on cancer care at the BCCOE were directly entered into EMR by clinicians at the point of care. We also excluded international (non-Rwandan) patients from our analysis as we expected a differential effect of the COVID-19 pandemic on them compared with patients from within Rwanda. According to national policy, access to care for domestic health emergencies, including cancer treatment, should have been able to be accommodated even during strict lockdowns, but international travel bans were much more absolute and continued for an extended period of time throughout the pandemic.22
Data source and definition of outcome variables
BCCOE uses OpenMRS, a web-based EMR to enter patient data. Patient information is directly recorded into EMR by healthcare providers at the point of care and EMR data officers conduct regular data quality checks by comparing different sources of data and correcting errors where necessary. When a patient attends a clinical visit at BCCOE, a dedicated EMR form is used to record each clinical encounter and procedures performed for that patient. Data for patients who received care from the RCC as a coping strategy to ensure access to cancer care during the COVID-19 pandemic were also recorded using OpenMRS EMR system and later synced to the BCCOE EMR server. We requested and received patient-level data from the oncology programme EMR system. We later aggregated and prepared these data for use in time-series analysis using Stata V.15 (Stata, College Station, Texas). The EMR data were extracted in multiple tables, including a patient roster, scheduled appointments and clinical visits attended. We merged these tables together to compute four different indicators aggregated at the monthly level (figure 1).
The ‘number of new patients’ outcome was defined based on the enrolment dates in the oncology programme. Only patients enrolled between 1 January 2016 and 31 July 2021 were included in the calculation of this variable. The ‘number of scheduled appointments’ outcome was created based on the monthly sum of patients’ unique scheduled appointment dates. Clinical care follow-up visits are only scheduled for existing patients and the types of scheduled appointments were as follows: chemotherapy infusion centre visit, chemotherapy inpatient ward visit, oncology pathology result visit, oncology special consultation visit, oncology biopsy visit and oncology outpatient clinic visit. The ‘number of clinical visits attended’ outcome was defined as the monthly sum of all patients’ unique encounter dates taken from EMR forms that are filled out when a patient is physically present for cancer care (eg, oncology clinical intake, cancer diagnosis, staging and treatment plan, etc)—this indicator included new patient intake visits and both scheduled and unscheduled clinical follow-up care visits for existing patients. Some forms which were not specific to cancer care (eg, mental health routine encounter, comorbidity of diabetes, hypertension, HIV/AIDS and heart failure diagnosis and treatment, etc) or could be filled out during remote patient follow-up (eg, rescheduled appointment) were excluded from the calculation of clinical visits attended. A patient was considered to have a ‘timely visit’ if the scheduled appointment date matched the date of the attended clinical visit; the ‘proportion of timely visits’ outcome was calculated by taking the number of timely visits divided by the number of scheduled visits for a given month. This indicator only included clinical follow-up care visits which are supposed to be prescheduled.
Data analysis
We described patients’ characteristics at enrolment using frequencies and percentages for categorical data and median and IQRs for numerical data. We tested associations between patient characteristics and the study period (before vs during COVID-19) using χ2 and Wilcoxon rank-sum tests as appropriate. We fit time-series models for the monthly number of new patients, scheduled clinical visits, attended clinical visits and timely clinical visits attended as a percentage of scheduled visits at the BCCOE during the baseline period (January 2016 to February 2020). We fit a generalised linear model with negative binomial distribution to estimate the monthly counts, and included terms for a yearly trend and seasonality:
 (1)
(1)
where  indicates monthly indicator count, t indicates the cumulative month number, K indicates the number of harmonic functions to include (we take
indicates monthly indicator count, t indicates the cumulative month number, K indicates the number of harmonic functions to include (we take  ) and
) and  is the denominator. The year term captures long-term annual trend while the harmonic terms capture seasonality. The offset (denominator) term takes value 1 for count indicators and is the monthly number of scheduled visits for the proportion of timely visits indicator. This mean model was chosen to allow smoothing without imposing strong assumptions on the seasonal behaviour. We used a negative binomial distribution to account for overdispersion.
is the denominator. The year term captures long-term annual trend while the harmonic terms capture seasonality. The offset (denominator) term takes value 1 for count indicators and is the monthly number of scheduled visits for the proportion of timely visits indicator. This mean model was chosen to allow smoothing without imposing strong assumptions on the seasonal behaviour. We used a negative binomial distribution to account for overdispersion.
The model in equation 1 was fit using prepandemic data and then used to predict outcomes for the COVID-19 period. These predicted outcomes reflect what we would have expected to observe if the COVID-19 pandemic had not occurred and can be used to assess disruptions attributable to the COVID-19 pandemic. Predicted counts were computed along with 95% prediction intervals (PI) and were used to compare observed counts to predicted counts during the COVID-19 period (March 2020 to July 2021). In this procedure, we also computed monthly deviations (predicted−observed count), cumulative deviations and per cent deviations over the entire period with 95% PIs. The bootstrap procedure has been described in further detail in a study conducted to investigate health facility catchment areas experiencing higher than expected rates of acute respiratory infections during the COVID-19 pandemic in seven LMICs,23 and has also been used to forecast annual incidence of dengue haemorrhagic fever in Thailand24 and to estimate the number of COVID-19-related deaths in the USA.25 We produced time-series plots showing observed and predicted counts (with 95% PI) during the baseline period and COVID-19 period. We also reported cumulative counts (observed and predicted), deviations and per cent deviations (with 95% PIs). All analyses were performed in R V.4.0.4.
Patient and public involvement
None.
Results
In this study, we analysed data on new enrolments, scheduled appointments and clinical visits attended for 8970 patients with cancer (figure 2). In total, 44 705 appointments were scheduled for these patients, while patients received cancer care at 51 370 different encounters during the study period.

Study participants and data cleaning flow chart. The total number of scheduled visits was smaller than the total number of attended clinical visits, as there was a portion of visits (eg, inpatient admission) that were not scheduled in advance. It was also true that not all scheduled visits were attended.
Table 1 shows the breakdown of patient characteristics at enrolment. Of the 8970 patients, 7140 (79.6%) were enrolled in the 50-month period before COVID-19, while 1830 (20.4%) were enrolled during the 17-month COVID-19 period. Based on the physical address of patients recorded in EMR, 3174 (35.4%) patients were from the Northern Province, 2110 (23.5%) from the Western Province and 920 (10.3%) from Kigali City. Seventy-five per cent (n=6753) of the patients were female. The median age at enrolment was 44.7 years (IQR: 30.7–58.1).
Characteristics of patients
Home province (p<0.001), gender (p<0.001) and diagnosis (p<0.001) at enrolment were significantly different between patients enrolled before and during the COVID-19 pandemic. There was no significant difference between the ages of patients at enrolment before and during COVID-19 (p=0.850).
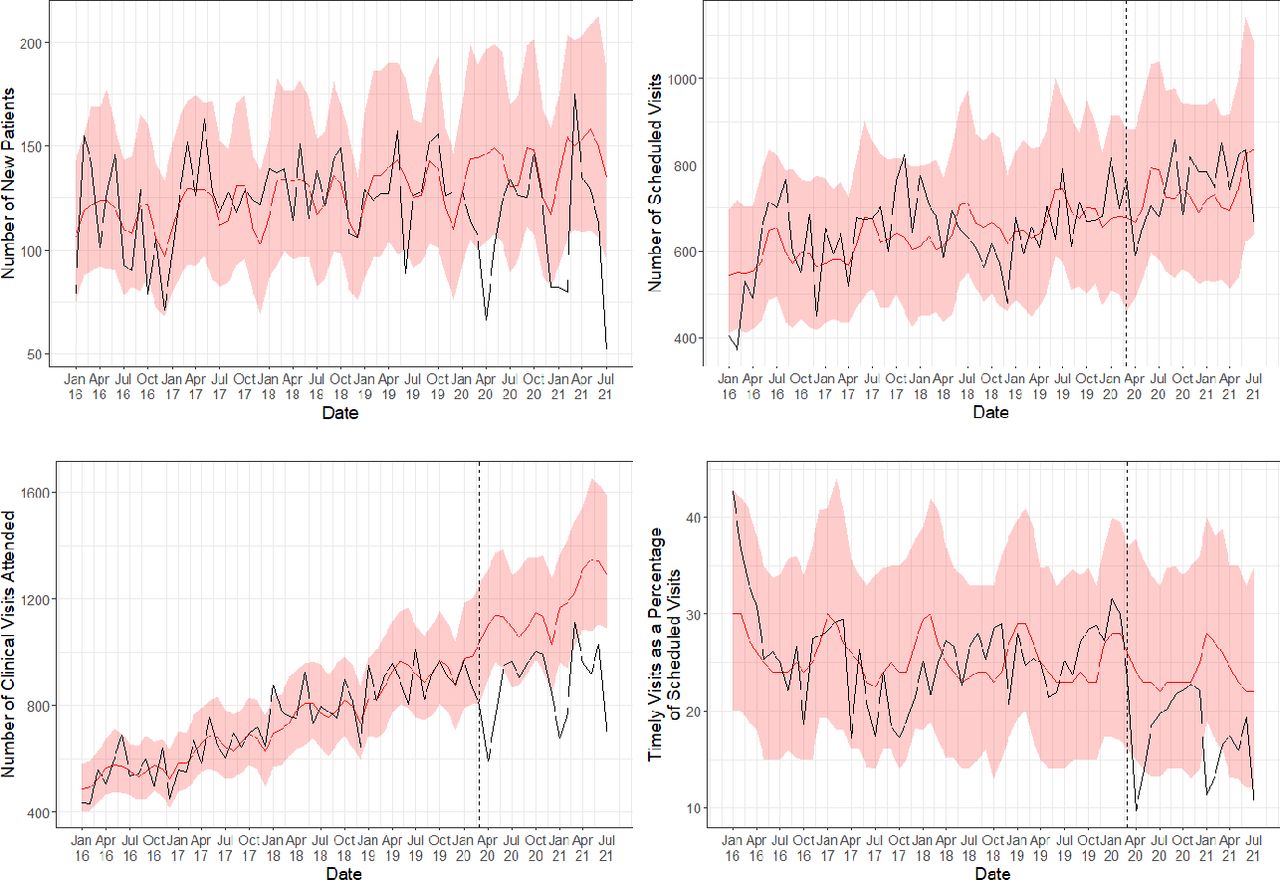
Our time-series analysis found significant deviations from the expected counts of new patients reported in April 2020, December 2020 to February 2021, and July 2021 (figure 3). There were also significant drops in the number of clinical visits reported in the months of April 2020, January to February 2021, and March to July 2021. Similarly, there were significant drops in the observed proportion of scheduled visits completed on time from expected in April 2020, January to February 2021, and July 2021. For the number of visits scheduled, no months show significant deviations from expected.
{kind=link}
{kind=link}
{kind=link}
Time-series models of new patients, scheduled clinical appointments, clinical appointments attended and timely visits as a percentage of scheduled appointments during the baseline period (January 2016 to February 2020) and COVID-19 period (March 2020 to July 2021).
Cumulatively, over the 17-month COVID-19 period, the observed counts of new patients, clinical visits and timely visits were significantly lower than expected (table 2). The estimated percentage deviation in the number of new patients reported was 21.7% (95% PI: −31.3%, −11.7%) less than expected. The estimated cumulative percentage deviation in the number of clinical visits reported was also 25.0% (95% PI: −31.1%, −19.1%) less than expected. In addition, the estimated percentage deviation in timely visits as a percentage of scheduled visits was 27.9% (95% PI: −39.8%, −14.1%) less than expected. There was no change in the number of visits scheduled (1.0%, 95% PI: −10.1%, 13.1%).
Cumulative counts and estimated deviations of indicators during the COVID-19 period (March 2020 to July 2021)
Discussion
In this study, we used routinely collected EMR data to assess the impact of the COVID-19 pandemic on access to cancer care at the BCCOE in rural Rwanda by comparing observed data during the COVID-19 period to the expected data, which was estimated based on 4 years of pre-COVID-19 pandemic data. Our findings indicate significant reductions in the enrolment of new patients, the number of clinical visits and the proportion of scheduled visits completed on time during COVID-19. However, the number of scheduled visits was not affected by the COVID-19 pandemic.
A significant drop in access to cancer care at the BCCOE during the COVID-19 could be attributed to the imposed measures to halt the spread of COVID-19 in Rwanda, including lockdowns, restrictions on movements of people between places and suspension of public transport which negatively affected the patient’s ability to reach the cancer centre.26 Specifically, we reported the largest declines in new patient and clinical visits in April 2020, January to February 2021, and July 2021 during which nationwide or regional lockdowns and restrictions on movement between districts were imposed in Rwanda.26 27 A previous survey conducted among chronic care patients in Rwanda during the initial COVID-19 lockdown (March to April 2020) found that patients with cancer were more likely to report at least one barrier to accessing care than any other group of chronic care patients (64.5% vs 43.6%).9 Cancer care in Rwanda is highly centralised and most care is provided in one of two health facilities. The BCCOE is in a rural location and is a 3-hour drive from the capital city of Kigali, making it challenging to access, particularly in a context of lockdowns and movement restrictions. In the early months (between 30 March and June 2020) of the COVID-19 pandemic in Rwanda, coping interventions were implemented through partnerships of PIH/IMB, governmental and private institutions to ensure continued access to cancer care for patients who were receiving care from the BCCOE.17 These coping interventions included transferring patients who need chemotherapy or radiotherapy and lived in Kigali City, southern or eastern provinces to RCC and availing PIH/IMB cars to transport patients between their homes to the BCCOE or RCC. However, the beneficiaries of these interventions were selected based on a number of criteria, including the type of treatment, the severity of the disease and the availability of infrastructure and space at RCC, and not all patients would have been eligible for this assistance. Furthermore, these interventions were designed for patients who had already enrolled at BCCOE before COVID-19—meaning that they would not have helped new patients access care during the pandemic.
A similarly significant drop in the number of new cancer cases detected during COVID-19 has been reported in other low-income10 28 and high-income countries.12 Elsewhere, reported reasons for the drop in the routine healthcare visits, including the number of visits for breast and cervical cancers, included health facilities’ prioritisation of emergency cases with COVID-19 like symptoms during the onset of COVID-19.28 In addition, a study conducted in Kenya revealed that the number of women screened for breast and cervical cancers through organised mass screenings declined by 89% between 2019 and 2020 due to the COVID-19 pandemic.29 In Rwanda, COVID-19 cases were referred to specialised treatment centres, such that health facilities did not experience similar resource shortages, even during COVID-19 surges.17 Our analysis corroborates this as BCCOE clinicians continued to schedule patients for visits at a similar rate to the prepandemic period, indicating minimal internal interruptions from the perspective of the healthcare providers. However, the stable levels of scheduled visits combined with the observed reduction in attended visits suggest that reduced utilisation of cancer services cannot be explained by clinicians adapting patients’ treatment plans to minimise in-facility visits by, for example, issuing multimonth prescriptions or delivering services at a more local health facility. Instead, patients appear to have been missing essential clinical appointments, and therefore increasing their risk of poor cancer-related outcomes.
Limitations
First, we used routine healthcare data from the EMR, which suffer from incompleteness, especially related to cancer diagnosis at enrolment, precluding our ability to look at these results by type of cancer. However, data on dates of enrolment, scheduled appointments and clinical encounters—variables that were used in the making of the outcome variables for this study—were all complete. Second, we used time-series models that controlled for pre-COVID-19 trends but did not account for other factors like cancer screening campaigns or changes in the socioeconomic and clinical characteristics of patients over time, which might have affected these trends before and during the COVID-19 pandemic period. Our clinical visits model captured the linear growth in the number of clinical visits over time; it is possible that the level of growth would have levelled out during 2020/2021 in the absence of COVID-19, potentially resulting in a false drop during the COVID-19 pandemic. However, we believe this is unlikely as the number of scheduled visits continued to grow linearly during this period, and there is still an unmet need for cancer care in Rwanda with only two cancer centres currently available to patients.
Conclusions
Compared with the pre-COVID-19 period, we observed a significant drop in the number of new patients, the number of clinical visits and the proportion of timely visits conducted by patients with cancer at BCCOE. This suggests delayed cancer diagnoses and treatment, which both may lead to negative health outcomes among our patient population in the coming months and years. Future studies should investigate the impact of these care interruptions on morbidity and mortality. It would also be very informative to specifically evaluate how the COVID-19 pandemic affected access to cancer care for the subset of international patients. Because BCCOE is one of the country’s main cancer referral centres and provides cancer care to most patients across Rwanda,21 these findings are of national importance. Increased investment in the decentralisation of cancer care services and the systematic adoption of telemedicine in the provision of cancer care could help reduce the effects of COVID-19 and future interruptions on access to care for patients with cancer in Rwanda and other similar settings.
Data availability statement
Data are available upon reasonable request. Data may be made available to reasonable requests sent to the authorship team, as any data sharing must follow existing health data sharing guidelines by Partners In Health/Inshuti Mu Buzima and Rwanda Ministry of Health.
Ethics statements
Patient consent for publication
Acknowledgments
We acknowledge the support of Todd Anderson in data extraction.
References
Footnotes
Twitter @DonaldFejfar, @DA_Barnhart
Collaborators The Cross-Site COVID-19 Cohort Technical Working Group is composed of the following members: Partners In Health/Boston: Jean Claude Mugunga, Stefanie Joseph; Partners In Health/Haiti: Wesler Lambert, Mary Clisbee, Fernet Leandre; Partners In Health/Liberia: Prince F Varney; Partners In Health/Lesotho: Melino Ndayizigiye, Patrick Nkundanyirazo, Afom Andom; Partners In Health/Malawi: Emilia Connolly, Chiyembekezo Kachimanga, Fabien Munyaneza; Partners In Health/Mexico: Zeus Aranda Remon; Partners In Health/Peru: Jesus Peinado, Marco Tovar; Partners In Health/Sierra Leone: Foday Boima, Gregory Jerome; Harvard Medical School: Bethany Hedt-Gauthier, Megan Murray.
Contributors PH and ANs were responsible for the design of the research, data cleaning, data analysis and writing of the manuscript. PH, ANs, DLF and IF were responsible for the ideation and development of this study. DLF was responsible for the data cleaning, analysis, code creation and figure creation. IF was responsible for the statistical methods development. All authors, including ANi, VKC, NK, JBB, CS, DAB, FK and the Cross-Site COVID-19 Cohort Technical Working Group, contributed to the design of the research and interpretation of results, and provided comments and review of the manuscript. AN, DLF and IF are the guarantors for the data used for this analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.