Article Text

Abstract
Introduction Patients do not always tell the physician if they have used medicines differently from prescribed. The challenges that patients experience in medication self-management and adherence have been prioritised globally as among the most crucial factors influencing the effectiveness and safety of pharmacotherapies.
Methods and analysis This study protocol presents a new patient-oriented method to investigate reasons for non-adherence using pharmacist-conducted medication reconciliation in a primary care clinic as data collection point. By interviewing, the pharmacist will learn how the patient has been taking the prescribed medicines and whether any non-prescription medicines and food supplements have been used for self-medication. The pharmacist will document the findings of the conversation to the electronic patient record in a structured format. The pharmacist will collect data related to the characteristics of the patients and outpatient clinics, patients’ diseases and medications, and medication discrepancies. These data will be analysed for descriptive statistics to identify (1) the number of discrepancies between the physician’s prescription orders and the patient’s self-reported use of the medicines, (2) what kind of discrepancies there are, (3) which are high-risk medicines in terms of non-adherence and (4) why medicines were taken differently from prescribed; based on the results, (5) a preliminary conceptual model of patient-reported reasons for non-adherence will be constructed.
Trial registration number NCT05167578.
- PRIMARY CARE
- Protocols & guidelines
- Quality in health care
- Risk management
- Adverse events
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The strength of this study protocol is a new patient-oriented method to find the reasons for non-adherence in routine clinical practice in primary care.
Pharmacist-led medication reconciliation will be used as a data collection point.
As this is a preliminary explorative study, we expect to create a better understanding of pharmacist-led medication reconciliation as a possible intervention to improve medication adherence.
The limitation is that it will be conducted in only one city in Finland, and the results cannot necessarily be generalised to other healthcare sites.
Sample size is small, and no sample size calculation was made, which may be a limitation.
Introduction
Challenges related to medication self-management and up-to-date medication lists have been prioritised globally as among the crucial factors influencing rational pharmacotherapy and patient safety.1 2 Establishing and maintaining patients’ reconciled medication lists have proven problematic in healthcare.1 3–5 Medicines may be missing from a list, and there can be old prescriptions or other errors in a list.3 On the other hand, patients’ self-medication may not be included in their medication list, although self-medication may have clinically significant effects or interactions with patients’ other medicines.4 In an emergency department study in Finland, many outpatients who came to the emergency department had errors in their medication list, and 79% had at least one long-term medication missing from the list.5 The most common error was the omission of medications taken as needed.
Polypharmacy can cause risks in medication management, and the risk increases when the number of medicines increases.6–8 Patients’ beliefs and experiences with medicines affect medication taking and treatment outcomes.9 10 Patients do not always tell the physician if they have taken medicines differently from how they were prescribed.10 The more medication-related problems patients experience, the more likely it is that they will start to alter and modify their medication.9 On the other hand, patients may not think that adjusting their medication is non-adherence. They may do it because of practical reasons, misunderstandings or because of experiencing medication-related burden.9 11 Family support and open patient–provider communication have been found to play significant roles when trying to prevent and tackle non-adherence.10 12 13 However, physicians struggle with a high workload and do not always have time to focus enough on each individual patient’s experiences, worries and beliefs about medicines.14 Health professionals may lack understanding of the patient’s journey with a chronic disease and its management.10 15 They may review the positive clinical treatment outcomes as an indicator of adherence to treatment and overestimate medication adherence.15
Medication reconciliation has become an essential part of the safe medication management process in healthcare, and it has increasingly become a pharmacist’s responsibility.16–20 Medication reconciliation is a process in which healthcare professionals compare all the patient’s medication orders to all the medications the patient is currently taking to resolve discrepancies and create an up-to-date list of medicines.21–24 The patient, or someone responsible for his medication, is always one of the sources for finding out and updating the patient’s medication history.25 Therefore, the patient interview needs to be included in every medication reconciliation procedure.1 23 25 However, studies related to medication reconciliation have mainly focused on calculating the number of identified discrepancies in medication data between data sources.26 Identified reasons for discrepancies have not been paid much research attention to, even though medication reconciliation provides an excellent opportunity to get patient-reported reasoning on medicine taking.
This study protocol aims to identify patient-reported reasons for medication non-adherence using pharmacist-led medication reconciliation in primary care as a data collection point. We will examine (1) the number of medication discrepancies between physicians’ prescription orders and patients’ self-reported medication use, (2) what kind of discrepancies there are, (3) which medicines can be classified as high-risk medicines for non-adherence and (4) why medicines are taken differently from prescribed; based on the results, (5) we will form a preliminary conceptual model for patient-reported reasons for non-adherence.
Methods and analysis
Study design and setting
This study is a prospective observational case study that will be carried out in the public primary care clinics in the city of Vantaa, located in the capital region of Finland. The research method will contain the pharmacist-conducted medication reconciliation, including a patient interview in a 30 min appointment. The pharmacist-conducted medication reconciliation practice was implemented in 2019 in Vantaa and is in routine use. The data will be collected through patient interviews during pharmacist-led medication reconciliation. The conclusions will be confirmed by discussion between all authors. The data will be analysed and reported in a peer-reviewed scientific journal.
Patient and public involvement
Patient and public involvement in the study is a new concept in Finland and not very common. Unfortunately, patients from primary care were not involved in the study design. We intend to disseminate the main results of this study to the public via social media.
Study context, population and recruitment procedures
The new electronic client and patient record system Apotti (based on the Epic system) was implemented in the Hospital District of Helsinki and Uusimaa (HUS) starting in November 2018.27 28 The city of Vantaa (approximately 238 000 residents) was among the first municipalities to implement Apotti in May 2019. The changeover from the previous electronic client and patient record system to Apotti was a significant effort for the healthcare staff. It was noticed that the changeover required pharmacists’ involvement in entering the medication lists into the new system in a reconciled format. Since then, pharmacists have been involved in medication reconciliation for outpatients with multimorbidity and multiple medications, usually before their appointments with physicians.
The data will be collected in four public outpatient clinics in Vantaa during medication reconciliation conducted by pharmacists. Physicians, nurses and pharmacists will identify eligible patients for this study (table 1). We will include patients 55 years of age or older, as they most commonly have multiple medications and illnesses. The patient will be receive both oral and written information about the study. If the patient is willing to participate and sign the informed consent, they will be included in the study.
Inclusion and exclusion criteria for the study participants
Sample size
The study will include 250 patients who attend public outpatient clinics in Vantaa, Southern Finland. As our research is a small-scale exploratory study of observational nature and we are not aiming to study the intervention’s effectiveness, we have not performed sample size calculations. We estimate that 250 patients would allow enough observations for preliminary conclusions about the suitability and feasibility of the study design and method to be used in future studies.
Medication reconciliation intervention and data collection
Healthcare professionals (physicians, nurses and pharmacists) present the study to patients (oral and written information) who meet the inclusion criteria and give written informed consent. The patients will have time to consider their participation (figure 1).

The study process starts with identifying eligible patients and ends with analysing of the collected data and reporting the results.
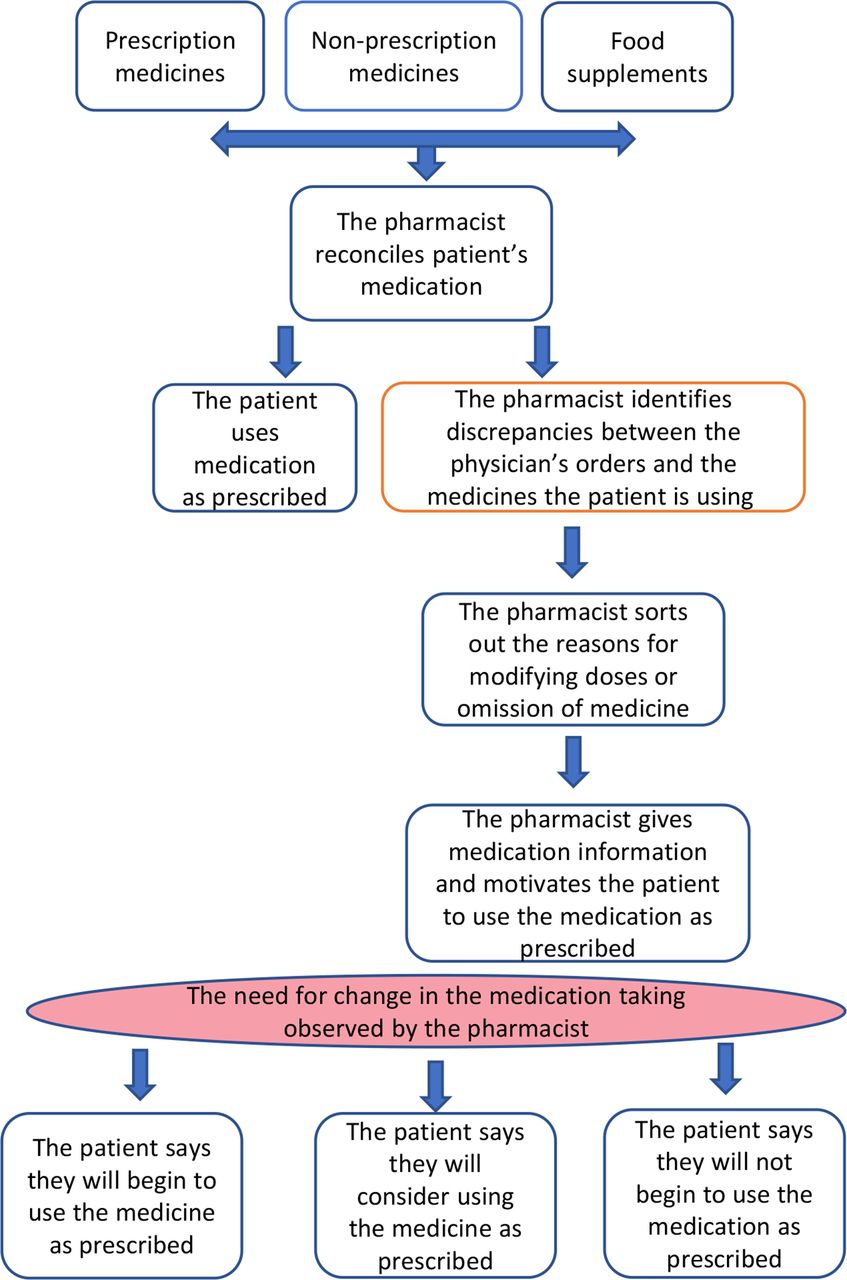
The data will be collected during the pharmacist-led medication reconciliation and entered in the pseudonymised form into the secured Helsinki University Hospital (HUS) electronic case report form, HUSeCRF database (figure 2; HUS electronic case report form presented in table 2). All the pharmacists will use the same interview and documentation technique (figure 2 and table 2). Medication reconciliation will take place on admission to the public outpatient clinic, usually before an appointment with a physician. The pharmacist will go through with the patient all medicines prescribed to them, according to the Apotti database, and will also consider non-prescription medicines and food supplements to assess the actual medicines used by the patient (figure 2). If the pharmacist identifies medication discrepancies between the physician’s prescriptions and the patient’s self-reported use of the medicines, the pharmacist will ask the patient about the reasons for adjusting the medication. Based on this process, the pharmacist will formulate the updated medication list, including also clinically appropriate non-prescription medicines in the patient record system, Apotti, where the physician will verify it.

{kind=link}
{kind=link}
Flowchart of the pharmacist-conducted medication reconciliation process at the public outpatient clinic in the city of Vantaa, which will be used as a data collection point for this study.
Variables that will be documented to the data collection template
If the pharmacist identifies any medicine-taking problems or barriers, the pharmacist will clarify the possible misunderstandings or concerns influencing medication use by discussing and explaining to the patient how to self-manage their medication appropriately and safely. The barrier can be, for example, unintentional non-adherence such as forgetting to take medicine or poor medication administration techniques. The pharmacist will find the best solution from the patient’s perspective together with the patient. The solution may be, for example, to go through with the patient the correct medication-taking technique or find the appropriate memory aid. If a barrier is difficult for the patient to overcome, the pharmacist will report it to the physician. If the pharmacist identifies urgent drug-related problems (DRPs), the pharmacist will inform the clinicians about them immediately. The urgent DRPs can include, for example, inappropriate prescribing, drug interactions or medication that is potentially inappropriate for the patient.
Analysis
The data will be documented in a structured format in the HUSeCRF database (table 2) and analysed by descriptive statistical analysis. The quantitative analysis will focus on the following variables and measures: (1) the number of medication discrepancies between physicians' prescription orders and patients’ self-reported medication use, (2) the type of discrepancies, (3) the list of medicines most commonly reported to been taken differently from prescribed (identification of high-risk medicines for non-adherence) and (4) reasons for taking medicines differently from prescribed; and the qualitative part of the analysis will focus on (5) forming a preliminary conceptual model for patient-reported reasons for non-adherence.
Quantitative analysis
We will calculate the prevalence of discrepancies from the data and how many discrepancies we will find altogether (frequency, %). We will categorise the types of discrepancies, for example, omissions, duplications, contraindications, unclear information and changes (n, %). The occurrence of discrepancies (n, %) according to the therapeutic group and active ingredient will be analysed using Anatomical Therapeutic Chemical (ATC) categorisation.29 The most common (top 10) drug substances and ATC groups of reported discrepancies will be analysed to identify the medicines at high risk of non-adherence. The quantitative data will be analysed using IBM SPSS Statistics V.26 software.
Qualitative analysis and meta-synthesis: constructing the preliminary conceptual model of reasons for non-adherence – the iceberg model
We will analyse the small amount of qualitative data, which the pharmacist has written from uncoded patient reasoning. We will synthesise our qualitative findings with our quantitative findings into the meta-synthesis, where the results of this study and our two previous qualitative studies10 14 are combined to create a hypothesis about the reasons for non-adherence.
In the iceberg model, the medication discrepancies are the tip of the iceberg, a visible part, and the reasons for the discrepancies are hidden below the surface. According to this model, the root reasons for non-adherence can be identified during the medication reconciliation process with the patient, as the reasons for adjusting or stopping taking medicine may not be visible. Understanding the root reasons for non-adherence from the patient’s perspective provides the possibility to support the patient in the most effective way.10
Study schedule and state of the study
The study start was on 15 April 2021, and the study completion is anticipated on 31 December 2023. The recruitment of patients for the study is ongoing, and the pandemic has caused delays in recruitment.
Ethics and dissemination
This study has received ethical approval from the Ethics Committee of Helsinki University Hospital (number HUS/1037/2020). Written informed consent is obtained from all patients involved in the study before any study procedure is performed. The results will be published in a peer-reviewed scientific journal.
Discussion
Health professionals need tools to recognise the patients’ hidden harmful health behaviour in clinical practice. Medication discrepancies can indicate non-adherence, and healthcare professionals can make the most of this information when finding out the reasons behind patients’ behaviour. Our study aims to provide unique information on why patients use medicines contrary to physicians' instructions.
Patients may use the prescribed medicines differently from how the prescriber has planned. There can be intentional or non-intentional non-adherence, and the patient may have a rational reason to modify doses. The pharmacist can be an excellent support to physicians when figuring out patients’ actual use of medicines and reasons for using medications against physicians’ orders at home. However, it is important to determine the prevalence of deviant use of medicines, the typical reasons for variability and what these medicines are in routine clinical practice. Furthermore, understanding the possible correlation between polypharmacy and medication discrepancies is essential according to targeted interventions for patients with chronic diseases.
Identifying patients at risk of using medications against physicians’ orders is essential. When a healthcare professional notices medication discrepancies related to a physician’s orders, it may lead to a more detailed discussion with the patient and interventions to increase medication adherence. Medication reconciliation may be a suitable method to study patients’ reported variant use of medicines and possible non-adherence through discussion between the pharmacist and the patients.
The strength of this study is that it provides a new perspective on finding non-adherence in routine clinical practice. The study shows a new way to find out the reasons for non-adherence and provides possibilities to plan tailored interventions to promote the rational use of medicines. We believe medication discrepancies can indicate non-adherence or problems with the use of medicines. Medication reconciliation is a standardised process, and pharmacists participating in this study are experienced. The study process and questions are standardised and available in writing, and the pharmacists are trained.
One limitation of this study is that it will be conducted at four primary care outpatient clinics in one city in Finland. The results cannot necessarily be generalised to other healthcare sites. Another limitation is the process of patient recruitment as, during COVID-19, outpatient clinics and hospitals have started using digital or remote appointments, in which case the patient consent may be difficult to obtain. As this is a preliminary exploration study of observational nature to test the suitability and feasibility of the study design and method, we did not make a sample size calculation, which may be a limitation. A patient-specific limitation is the possibility that the patients will not tell the pharmacist about the actual use of medicines. However, we believe this study will help those who plan further interventions to find out reasons for non-adherence and develop tailored interventions to support adherence in primary care.
In this study protocol, medication reconciliation will be used to monitor medication adherence and identify the non-rational use of medicines in routine clinical practice. This study is intended to give information about the new method to investigate reasons for medication discrepancies and their connection to polypharmacy. It may also provide a method to identify the high-alert medicines related to medication adherence, which helps healthcare professionals identify patients with a higher risk of non-adherence. We believe our study will help clinicians and researchers to develop more effective and patient-centred interventions to increase medication adherence. More research is needed to understand the patients’ experiences with medicines in different phases of life and to build up more patient-centred interventions to enhance medication adherence.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Acknowledgments
The Kunnallisalan Kehittämisäätiö (the Foundation for Municipal Sector Development) is thanked for a research grant for PhD thesis of KK. The city of Vantaa is gratefully thanked for providing resources for conducting the study: physicians', nurses' and pharmacists' time for recruiting the patients, and the pharmacist's time for collecting the data.
References
Footnotes
Twitter @KirsiKvarnstrom
Contributors Conceptualisation, methodology, formal analysis, investigation and writing (review and editing),: KK, AW, HL and MSAA; writing (original draft preparation), visualisation and project administration: KK; supervision: HL and MSAA; read of and agreement to the published version of the manuscript: all authors.
Funding This research was funded by the Kunnallisalan kehittämissäätiö (the Foundation for Municipal Sector Development, personal grant for PhD thesis for Kirsi Kvarnström). Open access was funded by the Helsinki University Library. The funding entity had no role in the design or conduct of the study; collection, management, analysis or interpretation of data; preparation, review or approval of the manuscript; or the decision to submit the manuscript for publication. This study has not received funding/assistance from any commercial organisation.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.