Article Text

Abstract
Objectives To describe clinical characteristics and prognosis related to heart failure (HF) phenotypes in a community-based population by applying a novel algorithm to obtain ejection fractions (EF) from electronic medical records.
Design Retrospective population-based cohort study.
Setting Data were collected for all patients with HF in Southwest Sweden. The region consists of three acute care hospitals, 40 inpatient wards, 2 emergency departments, 30 outpatient specialty clinics and 48 primary healthcare.
Participants 8902 patients had an HF diagnosis based on the International Classification of Diseases, Tenth Revision during the study period. Patients <18 years as well as patients declining to participate were excluded resulting in a study population of 8775 patients.
Primary and secondary outcome measures The primary outcome measure was distribution of HF phenotypes by echocardiography. The secondary outcome measures were 1 year all-cause mortality and HR for all-cause mortality using Cox regression models.
Results Out of 8775 patients with HF, 5023 (57%) had a conclusive echocardiography distributed into HF with reduced EF (35%), HF with mildly reduced EF (27%) and HF with preserved EF (38%). A total of 43% of the cohort did not have a conclusive echocardiography, and therefore no defined phenotype (HF-NDP). One-year all-cause mortality was 42% within the HF-NDP group and 30% among those with a conclusive EF. The HR of all-cause mortality in the HF-NDP group was 1.27 (95% CI 1.17 to 1.37) when compared with the confirmed EF group. There was no significant difference in survival within the HF phenotypes.
Conclusions This population-based study showed a distribution of HF phenotypes that varies from those in selected HF registries, with fewer patients with HF with reduced EF and more patients with HF with preserved EF. Furthermore, 1-year all-cause mortality was significantly higher among patients with HF who had not undergone a conclusive echocardiography at diagnosis, highlighting the importance of correct diagnostic procedure to improve treatment strategies and outcomes.
- heart failure
- epidemiology
- echocardiography
Data availability statement
No data are available. The data underlying this article cannot be shared publicly as the data are retrieved from patient medical records which are protected under the Swedish Health and Medical Services Act and the Secrecy Act in accordance with Swedish legislation. The data may be shared on reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Ejection fraction (EF) was determined in an unselected, community-based heart failure (HF) population.
Data were available for virtually all patients through the Regional Healthcare Information Platform including medications and clinical investigation results.
The EF algorithm had an extraction rate of 97% with 99% accuracy on validation.
A conclusive echocardiography was determined in 57% of cases and HF phenotyping was possible for a large number of patients.
Despite the comprehensiveness of this dataset, residual unmeasured confounding cannot be ruled out and causal inference is not established.
Introduction
The estimated prevalence of heart failure (HF) in the Scandinavian countries is approximately 2% and increases with age.1–4 HF may lead to decreased quality of life, frequent hospitalisations and an increased risk of premature death.3–10 Classification of HF is based principally on ejection fraction (EF) as determined by echocardiography.6 11 12 Patients diagnosed with HF with an EF <40% are considered HF with reduced EF (HFrEF) and those with an EF 40%–49% are considered HF with mildly reduced EF (HFmrEF), in accordance with guidelines from 2016.6 Individuals that present clinically as patients with HF but have an EF >50% are classified as HF with preserved EF (HFpEF). Optimally treated HF is evidently associated with improved quality of life, decreased morbidity and all-cause mortality.3–7 10 12 13 However, there are distinctions in the management of patients with HF based on the HF phenotype.6 10 12 14 15 Previous studies provide evidence of decreased mortality among patients with HFrEF when treated with beta-blockers (BB), renin-angiotensin-aldosterone system inhibitors (RAASi), mineralocorticoid receptor antagonists (MRA) and angiotensin receptor neprilysin inhibitors (ARNI).6 However, the recommended therapies have not shown the same effect among the other HF phenotypes.
A review of the European HF registry showed that 53% of all reported HF cases were classified as HFrEF.15 The vast majority of patients in this, and other registries, are diagnosed at the secondary care level where HF is often diagnosed secondary to underlying ischaemic heart disease (IHD) and the patients are often younger in age.13 14 16–18
Most population-based studies on patients with HF are based on surrogate variables for HF such as International Classification of Diseases, Tenth Revision (ICD-10) codes. These diagnostic codes are registered on completion of patient assessment including findings from physical examination and evaluation of laboratory findings. While validation studies of ICD-10 codes are common in Scandinavian countries, they may not be as common worldwide, thus, possibly compromising the internal validity of HF diagnosis.19–21 In addition, the majority of HF registries are, to date, not coded with regard to phenotypes. Studies from electronic medical records usually require manual data collection as phenotypes are rarely structured data, which is both time consuming and resource consuming.
The purpose of this study was to determine the proportion of patients who had undergone echocardiography at the time of diagnosis, and to better understand the clinical characteristics and distribution of HF phenotypes in a community-based population. Second, we aimed to estimate 1-year all-cause mortality and examine whether the application of echocardiography as part of the diagnostic workup was associated with mortality.
Methods
Data sources
Region Halland (RH) in Sweden provides a unique data ecosystem using the Regional Healthcare Information Platform (RHIP), which includes information from both the primary and secondary care levels, including all prescribed medications, clinical investigation results (ie, laboratory assessments, radiological examinations) and care delivery resources.22 RH is a county located in Southwest Sweden with a population of approximately 320 000. The infrastructure in the region consists of 3 acute care hospitals, 40 inpatient wards, 2 emergency departments, 30 outpatient specialty clinics, 48 primary healthcare (PHC) clinics of which approximately half are private care provider. The data were retrieved from RHIP.20 Medication’s data came from two sources into RHIP: (i) Swedish Prescribed Drugs Register and (ii) Apotekets Dosdispensering (Apodos).
Study population
All individuals ≥18 years of age with an ICD-10 diagnosis of HF (I110, I420, I423, I424, I425, I426, I427, I428, I429, I430, I431, I432, I438, I500, I501 and I509) during 2013 until 2019 were included in the study. The HF diagnoses were based on a clinician’s assessment. All patients included resided in RH at the time of diagnosis according to the Swedish National Population Registry. A lookback period from 2008 to 2012 was applied to ensure a naïve incidental HF patient cohort. Individual follow-up was completed at the end of the study period or at time of death, whichever came first.
Study procedure
Age and gender were registered at the time of initial HF diagnosis, henceforth referred to as index. Concomitant diseases were retrieved from the lookback period of the study period until index. The diagnoses are described in online supplemental appendix table 1, Charlson Comorbidity Index (CCI) was retrieved.23 24 All-cause mortality was defined as death from any cause during the period from diagnosis until 1 year postindex and the number of days after index was recorded.
Supplemental material
The distribution of genders, age, comorbidities and treatment at baseline in total and between different types of impaired cardiac function and HF-NDP
The NT-proBNP values registered were those closest to the time of the first HF diagnosis, here known as index. The NT-proBNP values were defined as either normal or elevated. A NT-proBNP was considered normal when NT-proBNP was <125 ng/L.25 Kidney function was established with the available estimated glomerular filtration rate (eGFR) (mL/min/1.73 m2) and P-creatinine closest to index.26 The eGFR were distributed into normal renal function with eGFR >60 mL/min/1.73 m2, lowered renal function with eGFR 30–59 mL/min/1.73 m2 and impaired renal function with eGFR <30 mL/min/1.73 m2. Heart rate, systolic blood pressure and diastolic blood pressure were collected when HF was first diagnosed.
The medications registered were BB (C07), RAASi (C09), MRA (C03DA) and loop diuretics (C03C). All registered BB, RAASi, ARNI and MRAs have an HF treatment indication (listed in the online supplemental appendix table 2).6 For the purpose of the analyses, treatment with ARNI was incorporated in the RAASi treatment group. Data regarding HF medications dispensed at the pharmacy were extracted pre-index and post-index. Dosage or the amount of drug were not considered. Four treatment groups were created based on post-index therapeutic strategies. Treatment with either BB or RAASi was defined as single HF therapy. Those with BB and RAASi were considered as having a double HF therapy and those with BB, RAASi and MRA were considered as having a triple HF therapy. Patients who were not prescribed BB or RAASi, or were only prescribed loop diuretics or MRA, were defined as having no HF therapy.
The distribution of HF treatment at baseline before first diagnosed with HF and treatment during the first year after diagnosed with HF
Extraction of ejection fraction values using algorithms and validation of methodology
The EF values were not part of the structured EHR data but were found in the free-text notes for a given echocardiography investigation. We developed an algorithm based on regular expression (RE) and keyword search to extract the EF values from the echocardiography notes (online supplemental appendix—algorithm 1). This approach was based on the observation that most EF values are expressed using a simple grammatical structure that could be analysed by a limited set of rules. In addition, a machine learning approach would require many examples of already labelled echocardiography notes for the training process. The necessary manual labelling process to create such training data was not possible in this study.
The most common way to express the EF values in the free-text notes was:
<keyword> <a variable amount of characters or word> <numbers or limited set of statements>
Examples of keywords are ‘EF’ or ‘Ejection fraction’, but they can also consist of multiple words such as ‘Systolic left ventricular function’. The EF statements are typically a number followed by a per cent sign (eg, 50%, but many variations are possible, such as 45%–50% and >55%). The statements can also be expressed using words, including ‘normal’, ‘moderate’ or ‘severe’. The above construction is ideal for an RE approach. Search patterns were created to find combinations of words that fit the above structure and identified the intended statements. From the found statements, including both values and words, the EF was categorised into HFrEF (EF <40%), HFmrEF (EF 40%–49%), HFpEF (EF >50%) and those with HF but no performed diagnostic echocardiography, which was classified as HF with no defined phenotype (HF-NDP) in this study.
The RE-based method to extract EF was validated in two independent steps. After an initial development of the method, using a limited set of echocardiography notes, a random selection of 100 notes were selected for the first validation step. This set was manually processed to extract EF categories and compared with the result of the automatic RE method. The mistakes made by the RE method was used to identify new rules and new keywords to handle the mistakes. The second validation step used a new set of 100 random notes and was used to assess the performance of the RE method. Since the phenotype was determined either by extracting a numeric EF value (if available) or phenotype-specific keywords, the sampling method was stratified to collect a similar proportion of notes for the different phenotype subgroups. The stratified random sampling was applied to evaluate both ways in which the EF algorithm classified the echocardiography notes in equally distributed subgroups. The RE method was developed using the Python programming language (V.3.8). A more detailed description of the EF extraction algorithm can be found in online supplemental file 1, algorithm 1.
If several EF measurements were available, the lowest EF was applied in the study as it was considered to best represent the patient’s heart function and used to classify the HF phenotypes. Patients diagnosed with HF not having an echocardiography at index were categorised as HF-NDP. Patients with an HF diagnosis and an EF <40% was categorised as ‘HFrEF’ and an EF ranging from 40% to 49% were categorised as ‘HFmrEF’. Patients with EF >50% were categorised as ‘HFpEF’ if given an HF diagnosis within 1 year after the echocardiography was performed. Those with EF >50% without a clinical HF diagnosis within 1 year after echocardiography were considered as not conclusive in order to emanate an HF diagnosis at the time of examination and categorised as HF-NDP.
Statistical analyses
Age, gender, concomitant diseases, laboratory tests and HF treatment were summarised using descriptive statistics. Continuous variables were described as means±SD or, when applicable, median and IQR. Kruskal-Wallis tests were used for comparison of groups. Categorical variables were analysed using χ2 tests and summarised using frequency and percentages. The number of missing values were described for both continuous and categorical variables. Missing baseline or follow-up covariate data were considered as randomly missing values in both groups. Missing values were noted for eGFR to a nominal degree, as well as NT-proBNP. As the latter was not used in comparing HF phenotypes, it was determined that imputation was not necessary. All-cause mortality ratio was analysed using Cox regression to first compare those with echocardiography and those with no defined phenotype (HF-NDP), and second to compare the different HF phenotypes. These Cox regressions were adjusted for age, gender, renal function, NT-proBNP, comorbidities and treatment strategies. The covariates included were chosen based on statistical significance in univariable analyses with a p value of <0.10 and with at least 80% of data available. The data were analysed using Cox regression for survival analysis. A two-sided p value <0.05 was considered as statistically significant. All analyses were performed with IBM SPSS Statistics V.27.0.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
Extraction of ejection fraction values for detecting HF phenotype
Of the 8775 individuals included in this study with an HF diagnosis, 6665 (75%) had undergone an echocardiogram at some point. The algorithm was able to extract EF data from 97% of these, and 57% were considered conclusive in relation to the date of diagnosis. Those with a non-detected EF were distributed to the HF-NDP-group. At the time of HF diagnosis, 5023 patients (57%) had undergone a conclusive echocardiographic examination. Of these, 35% were HFrEF, 27% were HFmrEF and 38% were HFpEF (online supplemental appendix figure 1). There were 19% of patients that had an echocardiogram performed beyond 1 year from index. Of these, 1642 had an EF >50% and 53 patients had an EF <50%.
Patient characteristics
Distribution of the HF phenotypes, gender, age, comorbidities, CCI and treatment at baseline are illustrated in table 1.
Renal function, NT-proBNP, heart rate and blood pressure are presented in table 2. The mean eGFR was 53.8 mL/min/1.73 m2 and there were 904 (10%) patients with impaired renal function <30 mL/min/1.73 m2. The number of patients having normal eGFR >60 mL/min/1.73 m2 were 5024 (57%) and 3751 (43%) had lowered renal function (<30–60 mL/min/1.73 m2).
The distribution of HF drug treatment at baseline is illustrated in table 1. Combination therapy with BB and RAASi appeared before index in 27% of the total patient population.
Baseline characteristics and associations with HF phenotypes
Female gender, higher age and hypertension were more common in the HFpEF group as well as in the HF-NDP group. Among patients with HFrEF, lower age, male gender and the occurrence of IHD were more common. The CCI was significantly higher in the HFrEF group (3,5 in average) compared with CCI for the HF-NDP group (3.2 in average) (p<0.001).
Treatment with the combination of RAASi and BB was more common in the HFpEF, HFmrEF and HF-NDP groups at baseline. The use of loop-diuretics was more frequent in the HF-NDP group. Both patients with HFmrEF and HFpEF had higher proportions of combination therapy with BB and RAASi at baseline, being 32% and 31%, respectively. Of the 4936 patients with RAASi, there were 45 patients with ARNI. Regarding the HF therapy strategies, 70% of patients with HFrEF had either double or triple therapy, compared with 63% for HFmrEF, 44% for HFpEF and 30% in the HF-NDP group as illustrated in figure 1.
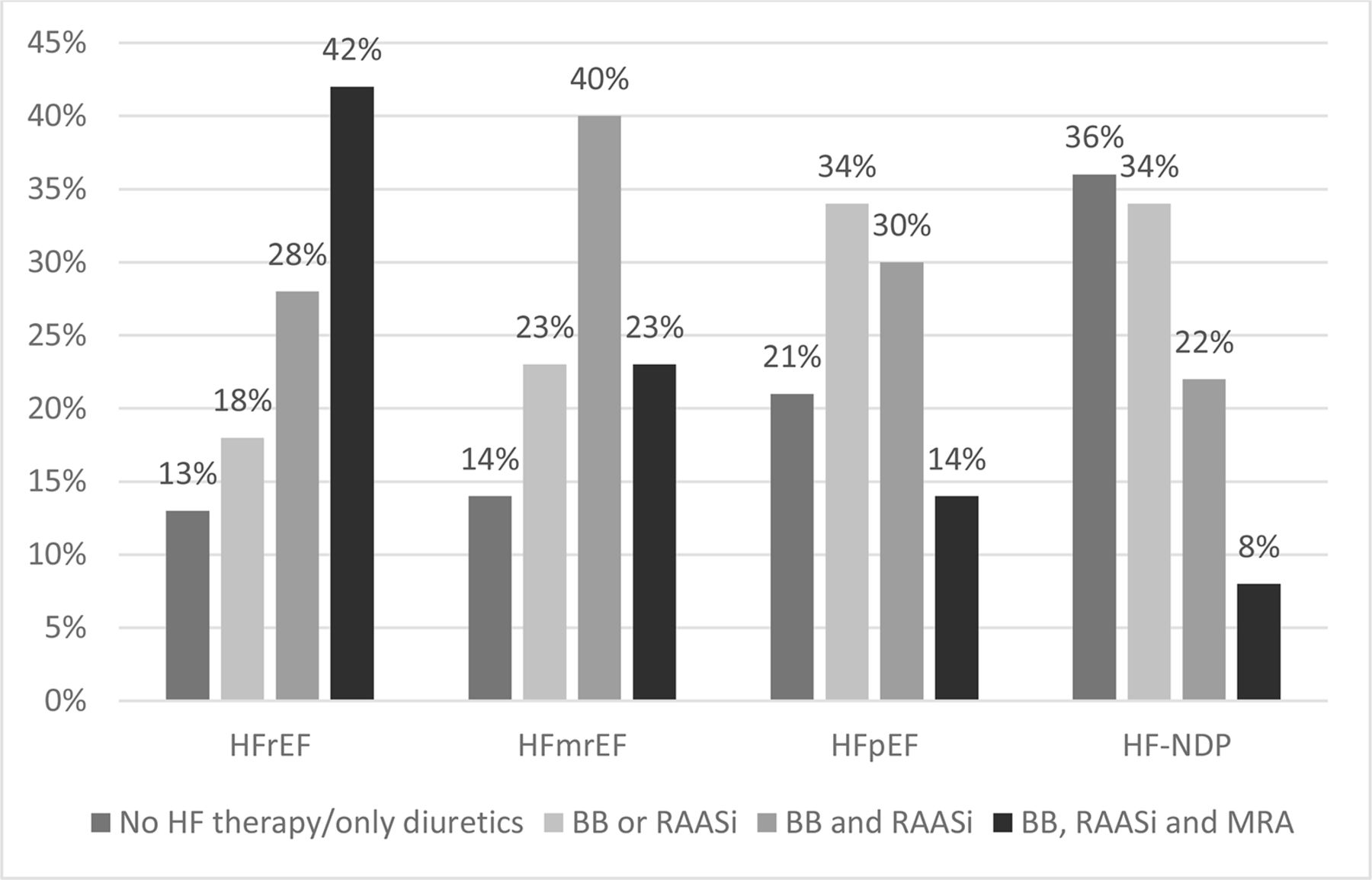
{kind=link}
Illustrates the differences in heart failure (HF) therapy from index separated into HF phenotype and the HF with no defined phenotype (HF-NDP) group without echocardiography. The treatment is defined by picked up medication. BB, beta-blockers;HFrEF, HF with reduced ejection fraction; HFmrEF, HF with mildly reduced ejection fraction; HFpEF, HF with persistent ejection fraction; MRA, mineralocorticoid receptor antagonists RAASi, renin-angiotensin-aldosterone system inhibitor;.
Renal function, as defined by mean creatinine and eGFR levels, did not differ between the groups. However, the proportion of patients with impaired renal function was significantly higher in the HF-NDP group compared with the other groups in which echocardiography was performed. The proportion of patients with impaired renal function was similar in the three echocardiography groups. Fifty-nine per cent of the HF-NDP group had decreased renal function defined as eGFR <60 mL/min/1.73 m2, whereas 13% had an eGFR <30 mL/min/1.73m2 (table 2). In the group with HFrEF, NT-proBNP was elevated in 92%, normal in 3% and missing in 6% of cases. In the group with HFpEF, the corresponding proportions were 82%, 8% and 10%, respectively. In the HF-NDP group, NT-proBNP was missing in 25% of the cases and 67% were elevated. The mean value for eGFR was lowest in the HF-NDP group (50.5 mL/min/1.73 m2) and highest in the HFrEF group (56.0 mL/min/1.73 m2). With regard to NT-proBNP levels, a higher proportion of the patients in the echocardiography groups had elevated levels compared with the HF-NDP group. The HF-NDP group also had more missing values.
In the HF-NDP group, 39% of patients were first diagnosed at a PHC facility. Among patients in which echocardiography had been performed, 20% were diagnosed at a PHC facility. In patients first diagnosed when admitted to hospital, 49% were part of the HF-NDP group, while 58% were diagnosed based on conclusive echocardiography. Five per cent of patients diagnosed in outpatient care at the hospital were considered HF-NDP, while 15% had a conclusive echocardiogram.
Mortality and association with performed echocardiography
The all-cause mortality in the total cohort was 7% within 14 days from index, 15% within 90 days and 35% after 1 year. The 1-year all-cause mortality for HFrEF, HFmrEF, HFpEF and the HF-NDP groups is illustrated in table 1. Mortality was high in the HF-NDP group with 9% deceased within the first 14 days from index and 19% within 90 days. The all-cause mortality for patients with echocardiography was 8% within 14 days and 11% within 90 days. When comparing patients with defined EF and those in the HF-NDP group, the HR for all-cause mortality was 1.26 (95% CI 1.17 to 1.36) when adjusted for age, gender, NT-proBNP, renal function, comorbidities and treatment strategies (table 3). Among deceased patients, the CCI was 4.0 for those that had undergone echocardiography and 3.4 for the HF-NDP group (p<0.001).
All-cause mortality ratio by Cox regression comparing those with echocardiography and those with no echocardiography, defined as heart failure with no defined phenotype (HF-NDP)
Mortality and association with EF
A Cox regression analysis comparing patients with HFrEF, HFmrEF and HFpEF showed no significant difference in HR (table 4). When adjusted for age, gender, NT-proBNP, renal function, comorbidities and treatment strategies, the HR for all-cause mortality for HFmrEF was 0.88 (95% CI 0.77 to 1.01) and for HFrEF it was 0.98 (95% CI 0.86 to 1.12). Increased age, elevated NT-proBNP levels and presence of comorbidity were associated with increased mortality risk, while HF therapy with BB and RAASi showed a significantly decreased HR.
All-cause mortality ratio by Cox regression comparing according to HF phenotype
Discussion
This unselected population-based study including all patients with HF in Southwest Sweden provides important insights on the distribution of HF phenotypes, which varies from those in selected HF registries, with fewer patients with HFrEF and more patients with HFpEF. A conclusive echocardiography to define HF phenotype was performed in 57% of the patients, a relatively high number that allows a greater understanding of the clinical characteristics and distribution of HF phenotypes in the community. Using a novel RE algorithm, it was possible to extract EF data from 97% of echocardiograms performed during the study period with 99% accuracy. The remaining 43% of patients were categorised as HF-NDP, diagnosed based on clinical criteria. One-year all-cause mortality was significantly higher within this group, highlighting the importance of echocardiography in HF diagnostics.
A conclusive echocardiography is crucial to the diagnosis of HF and the determination of HF phenotypes which in turn can affect therapeutic strategies. EF is a dynamic measurement that changes over time in response to medication and remodelling. An echocardiography performed >1 year prior to index may not truly reflect the EF at the time of diagnosis and hence, is considered outdated for determination of HF phenotype. In the present study, 57% of patients had performed echocardiography. A previous study examining the adequacy of HF diagnosis in Sweden found that 30% of patients had undergone echocardiography, while a more recent Swedish study demonstrated that 36.6% had performed echocardiography to determine HF phenotypes.8 27 The discrepancies could be attributed to the availability of echocardiography on a regional level. However, the number of patients diagnosed based on clinical criteria remains alarmingly high, which carries a risk for incorrect diagnosis and incorrect therapy.
Among patients with a conclusive echocardiography, 35% had HFrEF, 27% had HFmrEF and 38% had HFpEF. Previous studies based on HF registry have determined the distribution of HF phenotypes to be 48%–53% HFrEF, 17%–21% HFmrEF and 18%–26% HFpEF.15 17 As opposed to most registry-based studies, the current study is based on a fully unselected population showing a more even distribution of HF phenotypes with greater homogeneity. Patients in HF registries are typically younger males and are often enrolled in conjunction with hospitalisation, which increases the likelihood of being examined with echocardiography.17 Conversely, the diagnosis of HFpEF is more commonly seen in women.6 13 14
The presence and distribution of comorbidities observed in the current study population did not vary from previous published results.8 17 27 28 The most common comorbidities detected prior to the onset of HF were hypertension and IHD. The percentage of patients with diabetes and atrial fibrillation was also similar to findings in other studies.
HF treatment with a combination therapy restricted to BB and RAASi, without MRA, was seen in 27% of patients with HFrEF, while 44% had triple therapy consisting of BB, RAASi and MRA. Consequently, there were 71% treated with BB and RAASi, regardless of additional MRA. In the HFpEF group, 30% were treated with BB and RAASi, while 14% had triple therapy with the addition of MRA. This may be partly explained by the lack of treatment indication for patients with HFpEF.6 Patients with double HF therapy consisting of both BB and RAASi had a significantly lowered HR of 0.5 (95% CI 0.45 to 0.61), indicating a lower risk for all-cause mortality regardless of HF phenotype. One might expect triple HF therapy with BB, RAASi and MRA to further lower the HR. However, this was not seen in the current study (HR 0.55 (95% CI 0.47 to 0.65)). This is likely attributed to the fact that patients receiving MRA had more severe HF when treated in accordance with European Society of Cardiology (ESC) guidelines from 2016.6
The prognosis for patients with HF is poor and previous studies estimate mortality to be approximately 50% within 5 years, while a further study showed a 92% survival rate within 30 days of diagnosis.29–31 These findings are consistent with our results. The 1-year all-cause mortality in the present study was 35% for the total cohort. This finding is considered consistent when compared with a previous HF registry study.27 However, other similar studies have shown mortality to be as low as 8.2%.14 31 The difference is attributed to the fact that mortality in the present study is calculated from the first day of HF diagnosis, whereas comparable HF registry studies do not take the date of diagnosis into consideration. Patients without echocardiography have a remarkably high mortality of 42% within the first year after index and are likely diagnosed when they are in a late phase of life. When considering only those patients with conclusive echocardiography, the mortality is more consistent with other studies.3 14 27 In the present study, the 1-year all-cause mortality among the HF phenotypes was 31% for HFrEF, 30% for HFmrEF and 30% for HFpEF. The mortality rates are higher when compared with findings from an analysis of the ESC HF long-term registry, which showed 8.8% for HFrEF, 7.6% for HFmrEF and 6.3% for HFpEF.32 Again, the difference is likely attributed to the unselected population of a real-world study versus a relatively selected HF registry cohort.
Strengths and limitations
The major strength of this study is the comprehensiveness of the data in this unselected population-based cohort including patients with HF from both primary and secondary care, with <10 opting not to participate in the study. The population includes patients with HF providing a heterogeneous real-world patient population.
Nonetheless, it should be emphasised that the results of this observational study are descriptive and cannot provide causal conclusions.
The results must be addressed in light of some limitations regarding data quality and potential biases. First, the inclusion criteria for HF were based on ICD-10 codes, which to date have not yet been validated nationally in Sweden. However, a study from Sahlgrenska University in Gothenburg showed the overall validity of HF diagnosis for patients admitted during 2000–2012 to be high, which may indicate a high diagnostic validity in the Swedish patient register.31 There is a high specificity and positive predictive value for HF in other countries, but the sensitivity is lower according to published validation studies.19–21 Second, definition of HF phenotypes was based on EF values from the extracted echocardiographic examinations. It is possible that some patients were diagnosed using other techniques, but this would only apply to a very small group of patients and would not likely affect the results. Furthermore, the results of an echocardiography may be incorrectly registered or performed in another region and therefore not detectable. However, we do not anticipate the number of such cases to be great enough to impact final outcomes and therefore the risk is considered negligible. Overall, we expect the study participants to represent the general community-based HF population. There may exist subtle differences in regional healthcare management routines based on tradition and one should exercise caution when generalising the results of this cohort on a larger scale, particularly in terms of pharmacotherapy. Lastly, despite the comprehensiveness of the data, we cannot rule out residual unmeasured confounders. The group with no echocardiography is especially heterogeneous with higher age and mortality and lack recommended HF treatment to a greater extent. In this group, it is more uncertain whether the HF diagnosis is correct. These patients are usually not included in HF studies, which makes evaluation of the group more difficult. However, several studies have shown that the diagnostic workup is poor and seen in light of the validations studies, we expect the results are generalisable.
Conclusion
In this comprehensive real-world community-based cohort of patients with HF, EF was determined with echocardiography in 57%. Of these, 35% had HFrEF, 27% had HFmrEF and 38% had HFpEF. The remaining 43% of patients with HF-NDP were associated with higher all-cause mortality when adjusting for age, gender, NT-proBNP, renal function, comorbidities and treatment strategies. Efforts should be made to include the widespread use of echocardiography as part of a structured diagnostic workup for all patients with suspected HF, to adequately guide disease management based on HF phenotype and ultimately improve the prognosis of patients with HF.
Data availability statement
No data are available. The data underlying this article cannot be shared publicly as the data are retrieved from patient medical records which are protected under the Swedish Health and Medical Services Act and the Secrecy Act in accordance with Swedish legislation. The data may be shared on reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Swedish Ethical Review Authority with reference number 2020-00455. As this is a retrospective study, based on pseudo-anonymised data from the Region Healthcare Information Platform, individual patient consent was not required in accordance with the approval. All the methods and procedures in this study were conducted in accordance with relevant guidelines and regulations.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors BA and JD were involved in planning the study. AA and MO designed and tested the algorithm. BA, JD, KMØ and MC-S were involved in data interpretation. JD, BA, KMØ, AA, MO and MC-S contributed to the writing of the manuscript and were furthermore involved in revising it critically for important intellectual content and final approval of the version to be published. JD, KMØ, AA, MO, MC-S and BA have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. JD is the author acting as guarantor.
Funding This work was funded by Novartis Sweden AB.
Competing interests KMO is a PhD-student at the University of Oslo and an employee of Novartis Norway AS. MCS is an employee of Novartis Sweden AB.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.