Article Text

Abstract
Introduction Helicobacter pylori infection rates are high in China and worldwide, and maintaining good hygiene is effective in preventing H. pylori infection. Childhood is a critical stage for developing good hygiene practices. Therefore, in this study, we aimed to explore whether a comprehensive hygiene intervention can prevent H. pylori infection in primary schools in China.
Methods and analysis The School-based Hygiene Intervention to Prevent HelicObacter Pylori infection among childrEn study is a cluster-randomised controlled trial, which will include approximately 2400 children in grades 2–4 from 60 classes in 10 primary schools of Linqu County, Shandong Province. Schools will be randomly assigned (1:1) via a computer-generated list, to receive either comprehensive hygiene intervention (intervention) or the usual health education lessons (control), with stratification by area (urban or rural). The interventions will include the following: (1) Children’s education: lessons and cartoon books designed to provide basic knowledge about hygiene, H. pylori, hand hygiene, diet and oral hygiene will be provided to children; (2) Caregiver’s education: children will be empowered to share hygiene-related knowledge with their caregivers as homework; caregivers will be also invited to the school for hygiene lessons; (3) School hygiene promotion: suggestions will be provided for improving the hygienic environment. Children in control schools will receive usual health education lessons according to the arrangements of each school. The primary outcome is the prevalence and incidence of H. pylori infection among children at 1-year follow-up. The secondary outcomes are H. pylori and hygiene knowledge, family eating customs and hygiene practices among children and their caregivers, as well as school absences owing to diarrhoea. Additionally, growth in children is set as an exploratory outcome. General linear mixed models will be used to analyse differences between the intervention and control schools.
Ethics and dissemination Ethics approval has been obtained from the Institution Review Board of Tsinghua University (No: 20220020). Written informed consent will be obtained from each child and one of their caregivers. The findings of this study will be actively disseminated through scientific publications and conference presentations.
Trial registration number ChiCTR2200056191.
- Public health
- Community child health
- Epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study will assess a comprehensive hygiene intervention to prevent Helicobacter pylori infection among children.
Outcomes include the prevention of H. pylori infection as well as an increase in H. pylori and hygiene knowledge and practices among children and caregivers, reduction in diarrhoea incidence in children, and improved children’s growth.
To recognise the importance of the knock-on effects of health communication, children will be encouraged to impart hygiene-related knowledge to their caregivers in this study.
In comprehensive health interventions, it is difficult to distinguish the effect of each specific intervention.
The impact of COVID-19 restrictions and lockdowns could affect the progress and quality control of this project.
Introduction
Helicobacter pylori is a gram-negative bacterium that primarily colonises the human stomach and is transmitted by gastro–oral, oral–oral or faecal–oral routes.1 It is estimated that more than 50% of the world’s population is infected with H. pylori, with an infection rate as high as 70% in low-income and middle-income countries.2 3 H. pylori infection has harmful effects on several gastrointestinal diseases, such as duodenal or gastric ulcers, gastric cancer and gastric mucosa-associated lymphoid-tissue lymphoma.4 5 In recent years, increasing studies have revealed that H. pylori infection also has a wide range of impacts on health through extragastrointestinal effects, such as iron-deficiency anaemia, chronic immune thrombocytopenic purpura and growth in children.6 7 Therefore, solutions to reduce H. pylori infection are urgently needed.
In 2015, the Kyoto global consensus report on H. pylori gastritis recommended that all H. pylori-infected individuals should be offered eradication therapy unless there are competing considerations.8 This recommendation was subsequently adopted in other updated guidelines or expert consensuses for the management of H. pylori infection.9–13 However, large-scale treatment of H. pylori in the general population is not feasible. First, more than half the global population is infected with H. pylori, making the cost for therapy immeasurable. Second, triple, or quadruple concomitant therapies for H. pylori eradication are very complicated,8 9 11 and there are problems with drug incompliance and antibiotic resistance.14 15 Moreover, antibiotic treatment could alter the normal gastrointestinal flora in the body and cause multiple adverse effects on health.16
In addition to eradication therapy, another cost-effective and feasible way to reduce the prevalence of H. pylori among the general population is to take measures to prevent infection with H. pylori. Although the risk factors of H. pylori infection have been well-studied,17–19 there is little intervention research on how to prevent H. pylori infection in daily life. The known modifiable risk factors of H. pylori infection include inadequate sanitation, unhealthy hygiene practices, and infection among family members.20 Therefore, it is possible to prevent H. pylori infection by changing behaviours and lifestyles and improving environmental hygiene through hygiene intervention for susceptible populations.
Hand hygiene is considered to be one of the most effective ways to reduce infectious diseases. A meta-analysis suggested that handwashing can significantly reduce the risk of diarrhoeal disease by 40%.21 Studies have found that improving hand hygiene could promote children’s growth and reduce absence owing to illness among children in educational settings.22 23 Because the oral cavity is an extragastric reservoir of H. pylori and the bacterium is mainly spread via the mouth, it is very important to maintain good oral hygiene.24 25 A study from China reported that the positive rate of H. pylori infection decreased significantly owing to a special toothpaste treatment (p<0.01).26 Additionally, disinfecting toilets, using serving chopsticks, providing individually served meals and drinking boiled water are also important ways to prevent infectious gastrointestinal diseases.27 Given that H. pylori infection is caused by multiple factors, it is necessary to develop comprehensive hygiene intervention to prevent H. pylori infection.
Studies have shown that the high incidence of adult H. pylori infection and gastrointestinal diseases is closely related to childhood H. pylori infection.28–30 Because childhood is an important stage of human growth and development as well as a critical period for the development of good hygiene practice, it is of great importance to establish comprehensive hygiene interventions to prevent H. pylori infection during childhood.
We, therefore, designed the School-based Hygiene Intervention to Prevent HelicObacter Pylori infection among childrEn (SHIP HOPE) study with the aim to explore whether a comprehensive hygiene intervention implemented in primary schools could reduce the incidence of H. pylori infection in children.
Methods and analysis
Study aims
The SHIP HOPE study was approved in July 2021, with the aim to implement a comprehensive hygiene intervention in primary school students to reduce H. pylori infection. Because children have a substantial influence on their family members in China, this intervention would also encourage the delivery by children to their caregivers of H. pylori and hygiene information; thus, knowledge and hygiene practice among caregivers would also be evaluated.
It is hypothesised that (1) school-based comprehensive hygiene interventions can increase hygiene knowledge and improve hygiene practice among children; (2) comprehensive hygiene interventions can help enhance hygiene knowledge and impact the hygiene practice of caregivers and (3) the incidence of H. pylori infection will be significantly lower in the intervention group than in the control group among children.
Study design
Because most hygiene interventions will be provided at the school and class levels, and it is difficult to evaluate the impact of intervention on the incidence of H. pylori in a self-controlled study. Therefore, the design of a cluster randomised controlled trial was adopted in this study, with primary schools as randomisation units.
Setting
This study will be conducted in Linqu County, an underdeveloped region in Shandong Province, China. The region has been identified to be one of the areas with the highest incidence of gastric cancer in China, with an age-adjusted rate of 55 per 100 000 for men and 19 per 100 000 for women in 1980–1982.31 A previous meta-analysis showed that the relative risk of gastric cancer was 0.66 with H. pylori eradication (95% CI 0.46 to 0.95),32 suggesting that reducing H. pylori infection is effective in preventing gastric cancer. Therefore, preventing H. pylori infection is of great public health importance in this area of China.
This study has been registered in the Chinese Clinical Trial Registry (http://www.chictr.org.cn/index.aspx), with registration number ChiCTR2200056191.
Recruitment
Recruitment of schools
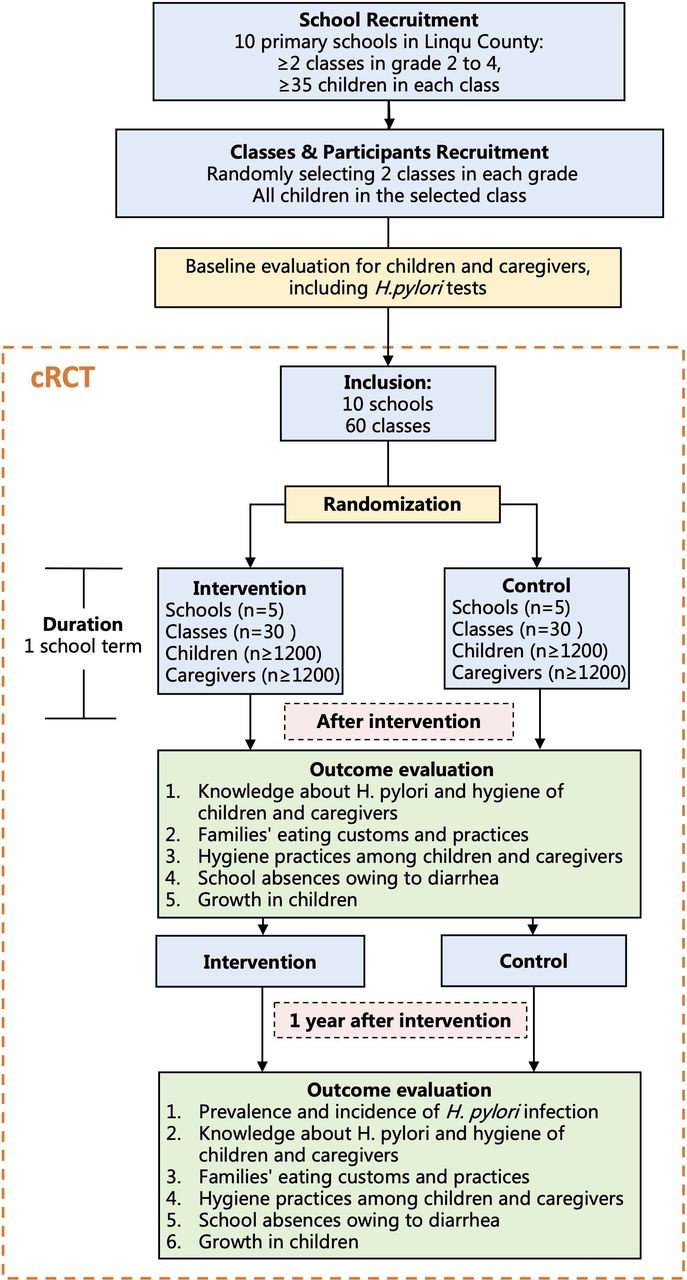
Like most areas of China, primary schools in Linqu have six grades in total, with children ranging in age from 7 to 12 years. Because children in the first grade have just started primary education and children in higher grades might have a higher rate of H. pylori infection at baseline, this study will be carried out among children in grades 2–4 (approximately ages 8–10 years). The eligibility criteria for schools are as follows: (1) the principal and teachers in the school are willing to participate in the study and can adhere to the randomised results; (2) the number of classes in each school from grade 2 to grade 4 is ≥2 and (3) the number of students in each class is ≥35 (figure 1).

Flow diagram for the SHIP HOPE trial. SHIP HOPE: School-based Hygiene Intervention to Prevent HelicObacter Pylori infection among childrEn. cRCT, cluster randomised controlled trial
A total of three steps will be implemented to recruit participating schools. First, researchers will calculate the number of clusters required for school and class recruitment. Second, we will cooperate with the Linqu Center for Disease Prevention and Control and the Education and Sports Bureau of Linqu to contact and recruit eligible primary schools. Third, a final list of 10 eligible schools and classes will be provided to the principal investigator and schools will be invited to participate in the study.
Recruitment of participants
According to our estimation, at least 2400 children from 10 schools will be recruited in the study. Additionally, we will recruit one caregiver (parent or grandparent) from each child’s family to participate in this study (figure 1). Before conducting the baseline assessment, written informed consent will be obtained from all students and their caregivers (parents or grandparents). If children or their caregivers refuse to participate in the survey, they will be excluded. For children or caregivers who refuse to participate, children can decide whether to receive the intervention courses or the related educational materials.
Baseline evaluation
The infection status of H. pylori will be detected using H. pylori stool antigen (HpSA) assay. All tests will be performed by the clinical lab of Weifang People’s Hospital using a commercial double-antibody sandwich ELISA (InTec PRODUCT, Xiamen, China), which is proven to have a sensitivity of 96.34% and a specificity of 96.81%. Stool samples will be destroyed immediately after H. pylori testing.
A structured questionnaire for children at baseline includes items on demographic variables, medical history (especially gastrointestinal disease history), hygiene practices and knowledge about H. pylori and hygiene. The baseline questionnaire for caregivers includes demographic variables, education level, occupation, family information, medical history (especially gastrointestinal disease history), family cancer history, eating customs and practices, hygiene facilities at home, hygiene practices and knowledge about H. pylori and hygiene. Anthropometric indicators of all children will be measured at baseline, including height, sitting height, weight, chest circumference, waist circumference, hip circumference and blood pressure. Additionally, the hygiene environment of each school and the status of health education courses will also be investigated at baseline.
Randomisation
Participating schools will be randomly divided into the comprehensive intervention group and the control group at a ratio of 1:1, stratified by area (urban or rural) at school level. Randomisation will be carried out using a computer-generated random number system by a researcher who is not involved in the study and is blinded to the identity of the schools.
Blinding
Owing to the nature of the intervention, all children, caregivers and teachers who provide lessons will not be blinded to the assignments. Investigators who will conduct the baseline and follow-up surveys and tests will be blinded. All investigators will be recruited from Weifang Medical College, Shandong, China.
Interventions
Comprehensive hygiene intervention (‘Good Hygiene Practice Package’) will be implemented in this study, which includes three sections: children’s education, caregiver’s education and school hygiene promotion. Details of these three sections are as follows.
Children’s education
Children in the intervention group will be provided information that includes basic knowledge of hygiene, H. pylori, hand hygiene, diet and oral hygiene. Eight hygiene education lessons (table 1) and cartoon books that include seven stories (table 2 and figure 2) have been designed to incorporate this hygiene information. While learning this content, children will be encouraged to make posters or draw illustrations to share their knowledge and experiences with each other. The contents of the lessons are designed and produced by teachers from the Vanke School of Public Health (VSPH), Tsinghua University and are polished by teachers from the Institute for Culture Creativity, Tsinghua University. Then, researchers from the VSPH will provide course training to the teachers from schools receiving the intervention. At least two outstanding teachers will be recommended for this training from each school in the intervention group. All teachers are required to be assessed and will be given pre-lectures prior to giving formal lessons. In addition to teachers who provide the lessons, class teachers and the vice principal in charge of health will also be invited to participate in the project, to coordinate all events.
Hygiene education courses for children and their caregivers
Cartoon books designed for children

Depiction of the designed cartoon books (A) Book cover. (B) Helicobacter pylori cartoon character in the book. These two pictures were drawn by Jiajing Wang, from the Institute for Culture Creativity, Tsinghua University (permission granted for publication).
Caregiver’s education
Children will be empowered to share their hygiene-related knowledge with their caregivers as homework. Caregivers will be invited to the school to learn how to prevent H. pylori infection in daily life, such as via hand hygiene, using serving chopsticks, providing individually served meals, disinfecting the toilet and drinking boiled water.
School hygiene promotion
Suggestions will be provided to schools for improving the hygiene environment according to the results of evaluation at baseline.
Controls
Children in the control schools will receive the usual health education lessons according to the arrangements of each school.
Outcome evaluation
The primary outcomes are the prevalence and incidence of H. pylori infection among children at 1 year after the intervention. The prevalence of H. pylori infection at 1 year after intervention will be evaluated in the whole study population. The incidence of H. pylori will be evaluated among baseline H. pylori negative children. The secondary outcomes are H. pylori and hygiene knowledge, families’ eating customs and practices, and hygiene practices among children and caregivers at the end of intervention and 1 year after intervention. Because the hygiene intervention could also have an impact on the transmission of other enteric pathogens that cause diarrhoea, school absences owing to diarrhoea are considered as a secondary outcome in this study. Additionally, because studies have reported that H. pylori infection can affect children’s growth, indicators of growth, such as height and weight, are also included as exploratory outcomes.
The infection status of H. pylori will be measured by the same HpSA assay used at baseline. Hand hygiene practices will be assessed according to the frequency of handwashing and frequency of using hand sanitiser based on the questionnaire. The questionnaire will also be used to evaluate families’ eating customs and practices as well as knowledge about H. pylori and hygiene among children and caregivers. School absence owing to diarrhoea will be recorded by teachers on the event record cards and via children’s self-report. Anthropometric measurements will be collected by trained investigators during the on-site surveys.
Retention
To promote participant retention and complete follow-up, there are two main considerations. For school levels, we will cooperate with the Education and Sports Bureau of Linqu, which oversees schools, to improve compliance. School officials and teachers will be regularly informed of the status of the study and plans for the next phase. The benefits and public health implications of the study will also be presented to them in detail, to obtain their full support. For children and caregivers, the results regarding children’s H. pylori infection status will be fed back to school officials and caregivers will be free to decide whether to receive these results. Students and caregivers will be informed of upcoming data collection and the intervention in advance. A small gift will be given to children at the baseline survey.
Data management
The collected data will be checked every day during the investigation, and missing data will be requested from children and caregivers by telephone. The information obtained from the questionnaire and the infection status of H. pylori will be double-recorded by trained staff using EpiData V.3.1 (EpiData Association, Odense, Denmark); inconsistent records will be checked against the original data for confirmation. In total, 5% of participants’ records will be randomly selected and checked against the original data to confirm the accuracy of the information. Finally, all collected data will be entered into an electronic database containing deidentified information. This database will be accessed by designated staff using a password.
Sample size
First, we calculated the sample size using incidence as the outcome indicator. According to a meta-analysis, the annual incidence of H. pylori infection is estimated to be 4% among children aged 6–14 years.33 Considering the high prevalence of H. pylori in the general population of Linqu, we assumed that the annual incidence of H. pylori infection is 5% in the control group and 2% in the intervention group, the number of children without H. pylori infection is 30 in each class, the intragroup correlation coefficient is 0.01, the alpha level is 0.05 and statistical power is 0.80. Thus, at least 26 classes in the intervention group and 26 classes in the control group are needed to detect differences.
Additionally, we calculated the sample size using prevalence as the outcome indicator. A meta-analysis reported that the prevalence of H. pylori infection is 33.9% in children aged 7–12 years.34 Therefore, we assumed that the prevalence of H. pylori infection is 34% in the control group and 27% in the intervention group, the number of children is 40 in each class, the intra-group correlation coefficient is 0.01, the alpha level is 0.05 and statistical power is 0.80. Thus, at least 24 classes in the intervention group and 24 classes in the control group are needed to detect differences.
After comprehensive consideration, two classes will be selected from each of three grades (grades 2–4) from 10 schools. In this study, 30 classes from 5 schools receiving comprehensive hygiene intervention and 30 classes for another 5 schools as the control group will be recruited.
Statistical analyses
Descriptive data will be presented as mean±SD, median (IQR), or number (percentage). General linear mixed models will be used to analyse differences between the intervention and control schools, with the covariance structure appropriately adjusted for variability both between clusters (schools and classes) and within a cluster (students within the same classes). For binary outcomes, we will report preintervention/postintervention percentages for the intervention and control groups and adjusted ORs and 95% CIs between groups. For continuous outcomes, we will report preintervention/postintervention means for the intervention and control groups and model-adjusted mean differences between groups.
Subgroup analysis will also be conducted based on children’s grade, school area (urban/rural), frequency of handwashing, frequency of using hand sanitiser and level of hygiene knowledge, etc.
Statistical analyses will be performed using SAS V.9.4 (SAS Institute). All statistical tests will be two sided at the 5% level of significance. For variables with missing data, we will impute the missing values using the sequential regression multiple imputation method if the percentage of missing data exceeds 5%.
Trial status
The initial proposed start date of this study was March 2022. However, the COVID-19 epidemic and local control policies led to postponement of this study. We are well prepared to conduct this study and plan to start the study in early November 2022 and complete data collection in December 2023.
Patient and public involvement
None.
Ethics and dissemination
Ethics approval was obtained from the Institution Review Board of Tsinghua University (No: 20220020). Written informed consent will be obtained from each child and one of their caregivers (online supplemental material). Because all children included in this study are under 16 years old, the consent form for children will be signed under the supervision of their caregivers and signed consent will be obtained from both children and caregivers. The results from the trial will be disseminated through manuscript publications and conference presentations. Once proven effective, our intervention strategy can be generalised to other primary schools in China, and the designed cartoon books will be published and made available to the public.
Supplemental material
Discussion
The harmful effects of H. pylori infection have been well recognised since it was isolated and reported in 1983 by Barry Marshall and Robin Warren. Based on evidence regarding the role of H. pylori in gastric cancer, the International Agency for Research on Cancer classified H. pylori as a class I carcinogen in 1994.35 In December 2021, H. pylori infection was first listed as a carcinogen in the 15th Report on Carcinogens of the US Department of Health and Human Services. It is estimated that H. pylori infection contributes to 780 000 new cancer cases each year, approximately 6.2% of all cancer cases worldwide.36 Consequently, a growing number of guidelines recommend a ‘test and treat’ strategy, which requires eradication therapy once H. pylori infection is confirmed, unless there are competing considerations. However, large-scale treatment of H. pylori in the general population is not feasible. Therefore, finding new solutions is warranted for this global public health problem.
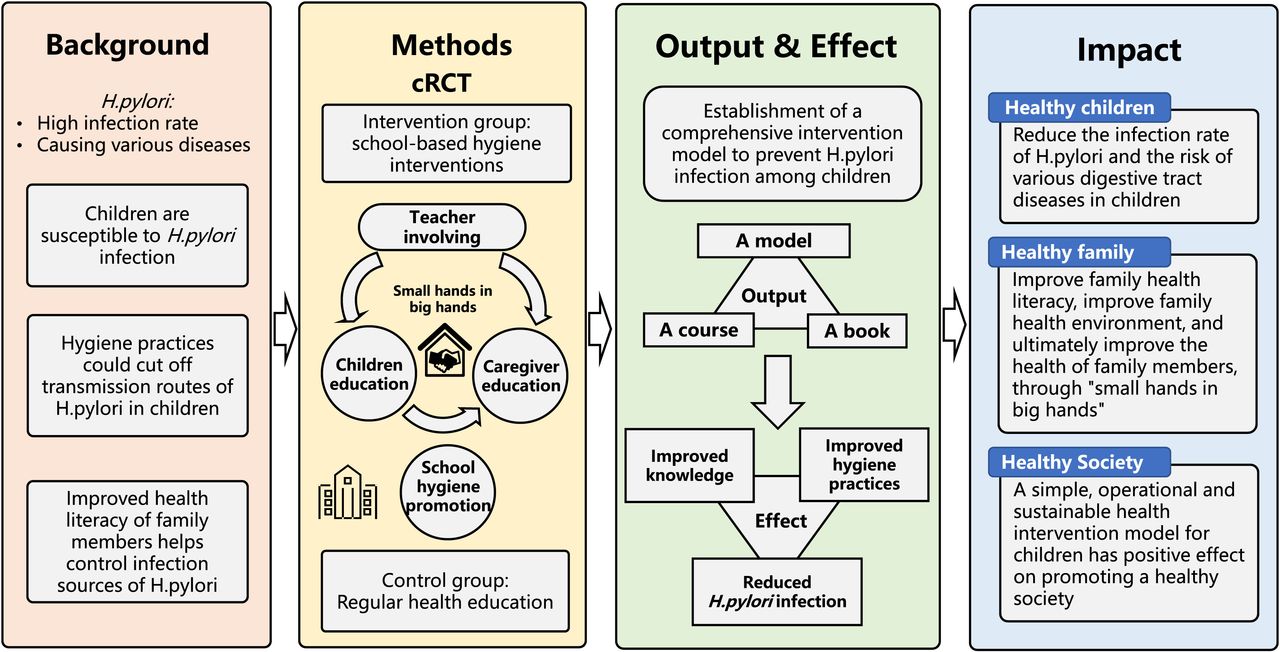
To our knowledge, the SHIP HOPE study is the first to propose a comprehensive hygiene intervention for the prevention of H. pylori infection among children. We will use the social ecological model to identify intervention elements in this study.37 We not only target risk factors at individual level but also at family and school environment levels, with the aim to improve knowledge, attitudes and behaviours among children, family members and teachers to promote a healthy society (figure 3). This study also has several other special and distinguishing features. (1) We have selected Linqu County, which is an underdeveloped area in China with a high rate of H. pylori infection and a high risk of gastric cancer, to implement this study. Therefore, the study can be generalised to other underdeveloped regions that have higher rates of H. pylori infection to obtain greater benefits of hygiene intervention. (2) Although the reduction of H. pylori infection is our main goal, the benefits of hygiene interventions are extensive and varied. (3) The components of the intervention are diverse but easy to implement. Once proven effective, a wider range of promotion can be carried out. (4) Children in different grades will be considered in this study; thus, we can explore the best time to provide the intervention.

{kind=link}
{kind=link}
{kind=link}
Study profile. cRCT, cluster randomised controlled trial.
There are also some limitations and challenges in the implementation of this study. First, according to the study design, it is difficult to distinguish the effect of each specific intervention in this study. Second, the COVID-19 epidemic is ongoing around the world. Although the epidemic in China has been well controlled, sporadic cases and local epidemics may still affect on-site investigations in schools. Some response strategies and alternatives in the investigation have been prepared in advance. Our on-site investigation work will be adjusted according to the COVID-19 epidemic situation and epidemic prevention policies in Shandong Province. We will try our best to avoid teaching online, considering the teaching effect and interaction. During the time of intervention, if schools are closed because of the epidemic, our intervention will be terminated until the schools reopen. Because the normal quarantine time is 14 days, a short pause in our intervention will have a minimal influence on the effect of the intervention. However, if the schools cannot resume normal classes for more than 1 month, we will adopt online teaching. We will select a time when the epidemic is completely under control in Shandong to conduct on-site investigation and intervention to reduce the probability of the above-mentioned situation. Additionally, the enhanced hygiene education provided during the COVID-19 epidemic may weaken the effect of the intervention.
In conclusion, this SHIP HOPE study will determine whether a comprehensive hygiene intervention to prevent H. pylori infection among children is effective. If effective, the intervention might not only reduce the incidence rate of H. pylori infection but could also reduce the risk of other gastrointestinal diseases, improve the health literacy of children and caregivers, and improve household hygiene, which in turn will improve the health level of the whole population.
Ethics statements
Patient consent for publication
Acknowledgments
We acknowledge the contribution of all children and their caregivers who will participate in the study and the support of all partners, including the Linqu Center for Disease Prevention and Control, the Education and Sports Bureau of Linqu, Weifang Medical School, Health Commission of Weifang and Institute for Culture Creativity and Tsinghua University.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
MZ and YZ contributed equally.
Contributors FC contributed to the conception and design of the study, gave final approval for publication, and is accountable for all aspects of the work. MZ and YZ contributed to the conception and design of the study, literature search, drafting and critical revision of the manuscript, development of intervention materials, and implementation of this study. YX, SL, JQ, GZ, YS and YG contributed to the literature search, designing the study, revision of the manuscript, and implementation of this study. All authors read and approved the final manuscript.
Funding This project is funded by the Incubation Fund of Vanke School of Public Health, Tsinghua University (2021PY002).
Disclaimer The sponsor has no role in the study design, analyses, interpretation of the data, or drafting of the manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.