Article Text

Abstract
Introduction Research on the needs and preferences of patients with poorly controlled type 2 diabetes mellitus (T2DM) with mobile health (mHealth) service is limited. With the principles of co-production, this study aims to address this research gap by exploring the health needs of Chinese patients with poorly controlled T2DM.
Methods and analysis This study uses a three-phase, exploratory sequential mixed-method design. Phase 1 aims to assess the health needs of patients with poorly controlled T2DM by conducting semi-structured interviews with patients, doctors and nurses. Participants will be recruited by purposive sampling with maximum variation. Content analysis will be employed. Phase 2 will form item generation and develop the mHealth need scale. The scale will be subject to pilot testing and psychometric evaluation, including content validity, construct validity, discriminant validity, internal validity and test–retest reliability. Phase 3 will explore the priority of health needs perceived by patients with poorly controlled T2DM through a cross-sectional study. The measurement tools include an mHealth needs scale, the Summary of Diabetes Self-care Activities Questionnaire, the Diabetes Empowerment Scale-Short Form, the Diabetes Health Literacy Scale and the eHealth Literacy Scale. Multiple regression techniques with a hierarchical block design will be used for the model building to identify the factors contributing to the heterogeneity of the perceived mHealth needs. The findings of phase 1 and phase 3 will be integrated using data correlation, comparison and consolidation.
Ethics and dissemination The Ethics Committee of the School of Nursing, Sun Yat-sen University, has approved this study (No. 2021ZSLYEC). The results of this study will be disseminated through conference presentations and peer-reviewed publications.
- General diabetes
- General endocrinology
- MEDICAL EDUCATION & TRAINING
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study uses a sequential mixed-method design and a co-production philosophy from multistakeholder perspectives to improve the robustness and credibility of the findings.
This study will develop a simple and easy-to-use instrument with sound psychometric properties to evaluate the mobile health needs of patients with poorly controlled type 2 diabetes for clinical research in the future.
Participants will be recruited from two tertiary hospitals in the first-tier city of China, which may limit the generalisability of the study results.
Introduction
Type 2 diabetes mellitus (T2DM) is the most common type of diabetes mellitus in China. The guidelines of the International Diabetes Federation and American Diabetes Association recommended that the ideal goal of the glycated haemoglobin A1c (HbA1c) value is less than 7.0% for adult patients with diabetes.1 2 However, a retrospective longitudinal study from five countries in Europe and the USA showed that 81.9%~96.6% of the patients with diabetes in different countries had not reached the ideal HbA1c goal.3 Similarly, about 76% of the patients with diabetes have not achieved the glycaemic target in China.4
Poor glycaemic control will lead to various potentially life-threatening microvascular and macrovascular complications,5 6 and a series of psychological problems, such as anxiety,7 depression symptoms8 9 and diabetes distress.10 Several studies observed that patients with poorly controlled T2DM tended to have a high level of negative disease appraisal and psychological distress compared with their counterparts.11–13 Besides, they will also have prolonged hospitalisation, frequent consultations and increased healthcare expenditure.13 14
There has been a burgeoning interest in integrating new technology into developing diabetes interventions to promote patients’ active self-management engagement. Mobile health (mHealth) technology, especially mobile applications, is becoming one of the mainstreams to deliver high-quality and permeable healthcare services.15 16 An increasing number of reviews have revealed that mHealth-assisted self-management interventions are effective in improving health literacy, self-efficacy and self-management activities among patients with diabetes in the short-term.17 18 However, literature investigating the effectiveness of mHealth interventions among patients with poorly controlled diabetes remains scarce.19 Patients with poorly controlled T2DM usually suffer from comorbidities, making their needs more challenging and complicated, which consequently poses a significant challenge in prompting complex and continuous care.13 20 So far, there is limited evidence about how the mHealth interventions address the needs perceived by patients with poorly controlled diabetes and engage them in self-management commitment. A robust investigation of the health needs of patients with poorly controlled T2DM must guarantee that the mHealth intervention fully matches users’ characteristics and produces added value in the trajectory of diabetes self-management.
Using a user-centre co-production approach is helpful to obtain more breadth and depth information about the health needs of patients with poorly controlled T2DM. Inspired by the co-production philosophy, patients are not merely recipients of health services but also contribute to designing and delivering health services as partners of healthcare professionals.21 Patients and healthcare providers (HCPs) have different roles and work together to various degrees in diabetes management. Patients play a core role in helping to identify complex and changeable unmet health needs.22 HCPs provide medical services and professional guidance in the co-production of health services.
Therefore, this study aims to address the aforementioned research gaps by using the co-production approach to explore the health needs of patients with poorly controlled T2DM from multistakeholder perspectives in the area of mHealth.
Aims
The project aims to: (1) explore the health needs of patients with poorly controlled T2DM under mHealth background using a co-production approach; (2) develop the mHealth needs scale and establish the psychometric properties of the prototype tool; (3) explore the priority of health needs of patients with poorly controlled T2DM; and (4) explore the role of self-management behaviour, self-efficacy, health literacy and eHealth literacy on the health needs of patients with poorly controlled T2DM.
Methodology
Design
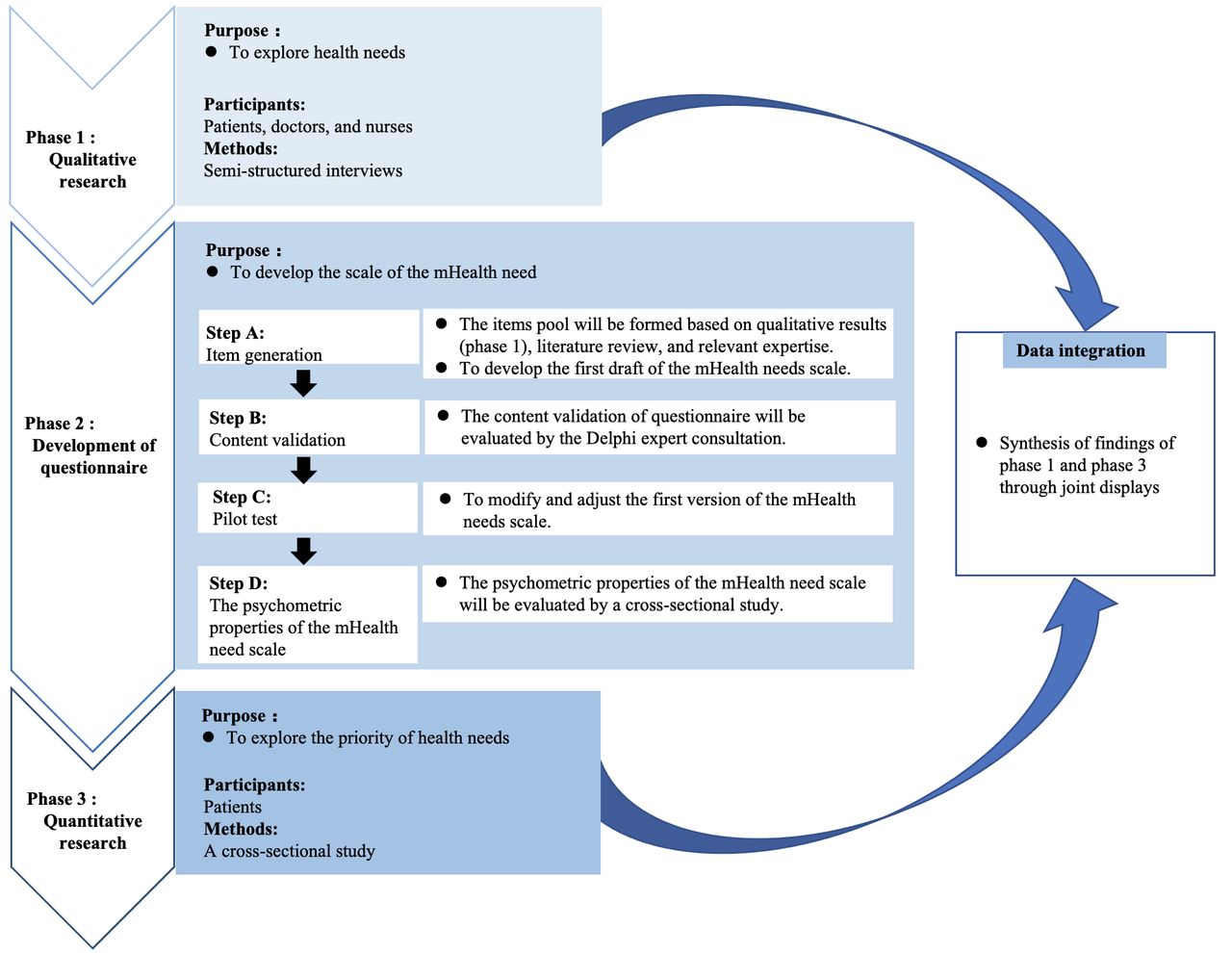
This sequential three-phased mixed-method study will mainly explore the health needs of patients with poorly controlled T2DM (figure 1). During phase 1, data will be collected from multistakeholder perspectives, including patients, doctors and nurses. In phase 2, a self-developed questionnaire will be designed to assess the mHealth needs based on qualitative interview results, relevant literature reviews and a panel of expert consultations. In phase 3, a cross-sectional study will be carried out among poorly controlled patients with T2DM to explore the priority of different health needs.

{kind=link}
Conceptual framework of the exploratory sequential mixed-method study.
Phase 1: to explore the health needs (qualitative research)
Participants, recruitment and setting
Participants, including patients with poorly controlled T2DM, doctors and nurses, will be recruited from the tertiary hospitals’ outpatient and endocrinology departments through purposeful sampling with the maximum variation.23 Patients will be eligible if they meet the following criteria: (1) adults (age ≥18 years) patients diagnosed with T2DM, (2) with HbA1c ≥7.0% in the last 3 months and (3) being able to provide informed consent. Exclusion criteria are as follows: patients with a malignant tumour, sensory or mental disability and severe acute or chronic complications (such as end-stage renal disease, blindness and heart failure). Interviews with doctors and nurses could facilitate a multidisciplinary analysis of diabetes care. The inclusion criteria for doctors and nurses are (1) registered nurse or registered doctor with a bachelor’s degree or above, (2) more than 5 years of work experience in the endocrinology department and (3) being able to provide informed consent. Recruitment continues until the result achieves thematic saturation in the analysis. We anticipate conducting interviews with approximately 30 patients and 20 HCPs.
Data collection
The semi-structured interview guides will be developed based on the constructs of the Capability, Opportunity, Motivation, and Behaviour (COM-B) model (online supplemental file 1).24 The COM-B model proposes three interacting domains (competence, opportunity and motivation). The patients and HCPs will provide information related to questions about capability (knowledge and skills, opinions towards mHealth technology), opportunity (support from mHealth technology) and motivation (emotion, confidence and intention) that may influence patients’ behaviours. The interview guide will be pilot tested among patients (n=3), doctors (n=3) and nurses (n=3) to identify the coverage and relevance of the content of the preliminary guide and to explore the possible need to modify questions. Interviews with patients and HCPs will be conducted in parallel to explore emerging themes across the participant groups.
Supplemental material
After obtaining demographic information and informed consent, a research assistant will conduct a face-to-face and semi-structured interview with eligible participants in a private and quiet place. Each interview will last for about 40–60 min. All interviews will be audio-recorded. Telephone interviews through WeChat, the most widely used social media platform in China, will be offered as an alternative to face-to-face interviews. Within 24 hours after the interview, the researcher will create the verbatim transcript. Respondents will confirm the data to ensure accuracy. All data will be managed and analysed by NVivo V.12 software.25
Qualitative data analyses
The content analysis approach will be used to analyse qualitative data.26 This involves a coding process of meaningful units and developing categories and themes. Two investigators (QX and YW) will transcribe the interview and gain a sense of the whole by reading the transcripts iteratively. Coding will be performed by identifying meaningful words or statements. The investigators will make margin notations with labels, and the referenced texts will be marked throughout by highlighting. Relevant codes with similar meanings or traits will be grouped into categories. All the data will be coded via line-by-line analysis. The two investigators will compare and discuss codes and categories. In case of disagreement, the viewpoint will be sought from a third investigator (LC). Participants’ suggestive non-verbal behaviours, including facial expression, mood and body language, will be considered in the data analysis. Themes will be refined to represent essential and relevant aspects of the research questions.
Rigour
The investigators will use several strategies to ensure the rigour and trustworthiness of qualitative research.27 28 First, pre-interviews will be conducted to improve the interview outline and interview process. In the research process, the investigators will be encouraged to have a critical reflection on the research, such as writing field notes and reflective diaries to discover and clarify personal biases. The memo dates will be marked how the researcher’s thinking changed over time, which is an essential part of the audit trail. Member checks will be confirmed whether the research materials and the interviewees’ results are consistent. Finally, this research will triangulate data sources, collect and compare data and conduct regular peer reports and discussions with qualitative research experts.
Phase 2: to develop the scale of the mHealth need
The development and evaluation process of the scale will be performed in four steps:
Item generation. The items pool will be formed based on the qualitative results (phase 1) and relevant literature reviews. This step will lead to the first draft of the scale of the mHealth need specifically for patients with poorly controlled T2DM.
Content validation. A panel of experts (n=15) will assess the content validity of the draft scale by a modified Delphi technique. The experts include diabetologists, endocrinologists, nurse diabetes educators, diabetes specialist nurses, nursing education managers and psychologists with expertise in diabetes care, who have worked over 5 years. Using purposive sampling, we will select experts from academic institutes, hospitals and diabetes nursing associations in Guangdong, China, and invite them by email. Experts will need to rate the relevance and clarity of each candidate item in the draft scale using a 4-point Likert scale by a modified Delphi technique. This 4-point Likert scale consisted of four responses: 1=Strongly disagree, 2=Disagree, 3=Agree, and 4=Strongly agree.
Pilot test. A pilot test (n=30) will determine the scale’s usability and readability, assess the clarity of the scale’s instructions and evaluate completion time from the patient’s perspective. Participants will also need to comment on the layout and format of the scale. This step will identify a preliminary tool for investigating the mHealth need.
Final evaluation of psychometric properties (n=500). A sample size of 500 will be sufficient as we anticipate exceeding the minimum number of respondents required by the exploratory factor analysis (EFA) and the rule of thumb of using 10 times the number of proposed items. We will assess test–retest reliability by inviting a subsample of 25 subjects who will complete the instrument again at a 2-week interval. Patients with poorly controlled T2DM will be selected through convenience sampling from the tertiary hospitals’ outpatient and endocrinology departments. The inclusion and exclusion criteria for patients will be the same as in phase 1.
Data analyses
We will exclude questionnaires with >10% missing responses or with a repetitive response pattern. Statistical analysis will be performed by IBM SPSS V.26 (IBM, Armonk, New York, USA). Descriptive statistics will be used to determine the demographic characteristics. Validity analysis includes content validity, construct validity and discriminative validity. The content validity of the questionnaire will be evaluated by calculating the content validity index (CVI) through the Delphi expert consultation. Exploratory factor analysis (Principal Components Analysis with varimax rotation) will be used to guide item reduction process and establish the factorial construct validity. Bartlett’s test of sphericity and the Kaiser-Meyer-Olkin measure of sampling will be used to test the suitability of the data for EFA. Factor retention will be based on the following criteria: (1) eigenvalues one or greater, (2) scree plot, (3) items with loadings above 0.30 and (4) interpretability of factors. The derived factor solution will then be used for subsequent reliability analysis. The internal consistency of the scale will be examined by Cronbach’s α coefficients. The intraclass correlation coefficient will be used as a measure of test–retest reliability.
Phase 3: to explore the priority of health needs (cross-sectional study)
Participants, recruitment and setting
In phase 3, participants (n=500) will be invited to complete the questionnaires (approximately 15 min) through convenience sampling from the tertiary hospitals’ outpatient and endocrinology departments.
Patients will be eligible if they meet the following criteria: (1) adults (age ≥18 years) patients diagnosed with T2DM, (2) with HbA1c ≥7.0% in the last 3 months and (3) being able to provide informed consent. Exclusion criteria are as follows: patients with a malignant tumour, sensory or mental disability and severe acute or chronic complications (such as end-stage renal disease, blindness and heart failure).
Data collection
The survey consists of three sections: (1) demographics, (2) clinical data and (3) patient-centred outcomes, including mHealth needs, self-management behaviours, self-efficacy, health literacy and eHealth literacy.
Patient-related demographic characteristics and disease-related information involve age, gender, education, marital status, employment, region of residence, monthly income level, smoking status and drinking status.
Clinical data include diabetes duration, Charlson Comorbidity Index, treatment, number of hospital admissions due to diabetes, family history of diabetes, ways to gain diabetes knowledge and whether patients have participated in diabetes health education.
The measurement tools include a self-developed health needs questionnaire with mHealth, the Summary of Diabetes Self-care Activities Questionnaire (SDSCA), the Diabetes Empowerment Scale-Short Form (DES-SF), the Diabetes Health Literacy Scale (HLS) and the eHealth Literacy Scale (eHEALS).
Measurements
The SDSCA is a self-reporting instrument assessing diabetes self-management in the last 7 days.29 The 12-item SDSCA includes general diet, specific diet, exercise, blood-glucose testing, foot care and smoking. Each dimension is rated on an 8-point Likert scale and scored each dimension separately. The average score of each item in each dimension indicates the performance of self-management ability in each behavioural dimension. The Chinese version of SDSCA has an acceptable internal consistency, with Cronbach’s α range from 0.62 to 0.98.30
The DES-SF measures the psychosocial empowerment of patients with diabetes.31 The 8-item DES-SF employs the 5-point Likert scoring system. A higher score indicates a better empowerment level. The Chinese version of DES-SF of Cronbach’s α is 0.77.31
The HLS is used to understand the ability and behaviour of patients with diabetes to accept and deal with diabetes-related health knowledge.32 The 14-item HLS includes three dimensions: functional health literacy (five items), communication health literacy (five items) and critical health literacy (four items). Each item uses a 4-point Likert scale with response options ranging from ‘never’ to ‘most’, and the score of functional health literacy is reverse coded. A higher level of the score indicates better health literacy. The Chinese version of the HLS of CVI (Scale-CVI) of HLS is 0.99, and Cronbach’s α is 0.868, with high internal consistency reliability.33
The eHEALS measures a person’s perceived skills in seeking and applying network health knowledge in health management.34 The 8-item eHEALS has three dimensions, including the application ability of network health information and service (five items), judgement ability (two items) and decision-making ability (one item). The score of each item is a 5-point Likert scale, and a higher score indicates better eHealth literacy. The Chinese version of eHEALS has an excellent internal consistency with Cronbach’s α of 0.913.35
Quantitative data analyses
Statistical analysis will be performed by SPSS V.26.0. The statistical significance level will be defined as two-tailed with a p value of <0.05. Continuous variables are present as means and SD—categorical variables are present as counts or percentages. The correlation between each variable and mHealth needs will be analysed by Pearson or Spearman correlation. The univariate analysis will be performed using the χ2 test and independent samples t-test as appropriate. The priority of mHealth needs will be explored and articulated by subgroup analyses. Multiple regression techniques with a hierarchical block design will be used for the model building to identify the factors contributing to the heterogeneity of the perceived mHealth needs.
Data integration: phase 1 and phase 3
Integration at the methods level occurs through the merging approaches,36 which combines the qualitative data (phase 1) and quantitative data (phase 3) for analysis and comparison. Integration at the interpretation and reporting level occurs through joint displays.36 The findings of the two databases will be mapped together based on thematic relevance in a matrix table, which is visual to draw out the priority of health needs of patients with poorly controlled T2DM.37
Patient and public involvement
Patients and the public were not involved in this study’s design, reporting and dissemination plans.
Discussion
This mixed-methods study broadens the limited evidence on the mHealth needs of patients with poorly controlled T2DM. Integrating qualitative and quantitative research will provide novel insights by summarising the key factors to be addressed in future mHealth-enhanced interventions. In addition, this study will also provide the health needs prototype tool, which would be beneficial to categorise and prioritise the mHealth needs in a precise and scientific manner. Ultimately, this study will advance our knowledge relating to the mHealth needs and shed light on the development of mHealth-based interventions to improve the self-management engagement of patients with poorly controlled T2DM.
This study has several advantages. First, using the co-production approaches, we involved the key stakeholders as co-researchers to reveal comprehensive health need types and convergences. Second, our mixed-methods study identified the characteristics of patients’ unmet health needs by efficiently integrating and synthesising qualitative and quantitative data. If the results from the qualitative interview and the cross-sectional study are mutually corroborated, we can consider the results more valid and scientific. The valuable information from data integration can guide the development of the mHealth-enhanced intervention specifically targeting patients with poorly controlled T2DM. In the case that results are divergent from each other, new research questions or hypotheses may be warranted for future endeavours.
In addition, this study has some methodological limitations. First, due to the questionnaire’s items not yet being developed, the calculation of sample size related to the final evaluation of psychometric properties has some deviation in phase 2. We anticipate a sample size of 500 will be sufficient, exceeding the minimum number of respondents required by the EFA and the rule of thumb of using 10 times the number of proposed items. Similarly, we also anticipate a sample size of 500 will be sufficient in phase 3. The final sample size will be adjusted based on the development of the item of the scale of the mHealth need. Second, convenience sampling will be used to select patients with poorly controlled T2DM to complete the questionnaires in phase 2 and phase 3, which may make the sample lack representativeness. Finally, the self-report data will be used as primary data sources in this study, which may have some biases (eg, recall bias) that affect the accuracy of the study results.
Ethics and dissemination
The Ethics Committee of the School of Nursing, Sun Yat-sen University, has approved this study (No. 2021ZSLYEC). The investigator will clearly explain the purpose of the research, potential risks and benefits and confidentiality issues to each participant. Signed informed consent outlined by the Helsinki declaration will be obtained from all respondents. Each participant could withdraw from the study at any time. The research team will facilitate the co-production process by involving the key stakeholders and motivating individuals’ engagement during and beyond the study. The results of this study will be disseminated through conference presentations and peer-reviewed publications. A final report will be submitted to the Chinese government to inform the campaign against poor glycaemic control.
Ethics statements
Patient consent for publication
Acknowledgments
We thank Sun Yat-sen University for their support of this research.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors QX, JP and LC conceived the study. QX, XH, YW, JP and LC contributed to the study design and methods. QX wrote the manuscript. JP and LC contributed to the revisions. All authors approved the final manuscript.
Funding We obtained support for this work from the National Natural Science Foundation of China (Grant No. 71904214) and the Guangzhou Basic and Applied Basic Research Foundation (Grant No. 202201011549).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.