Article Text

Abstract
Objective To explore the prevalence and patterns of multimorbidity in population with different genders and age ranges.
Design A cross-sectional study.
Setting National Health and Nutrition Examination Surveys database.
Participants 12 576 patients.
Primary and secondary outcome measures The prevalence and patterns of multimorbidity.
Results High cholesterol had the highest prevalence in all population (33.4 (95% CI: 32.0 to 34.9)) and males. In females <65 years, the most prevalent disease was sleep disorder (32.1 (95% CI: 29.6 to 34.5)) while in females ≥65 years, hypertension was the most prevalent disease (63.9 (95% CI: 59.9 to 67.9)). Hypertension and high cholesterol were associated with the highest support (occur together most frequently) in all population regardless of genders. Hypertension displayed the highest betweenness centrality (mediating role in the network) followed by high cholesterol and arthritis in all population. For males aged <65 years, hypertension and high cholesterol presented the highest betweenness centrality. In males ≥65 years, hypertension, high cholesterol and arthritis were the top three diseases of degree centrality (direct association with other conditions). As for females ≥65 years, hypertension showed the highest betweenness centrality followed by high cholesterol and arthritis. The associations of hypertension, arthritis and one other item with high cholesterol presented the highest support in all population. In males, the associations of depression, hypertension with sleep disorders had the highest lift (the chance of co-occurrence of the conditions and significant association). Among females, the associations of depression, arthritis with sleep disorders had the highest lift.
Conclusion Hypertension and high cholesterol were prevalent in all population, regardless of females and males. Hypertension and high cholesterol, arthritis and hypertension, and diabetes and hypertension were more likely to coexist. The findings of this study might help make plans for the management and primary care of people with one or more diseases.
- EPIDEMIOLOGY
- Hypertension
- DIABETES & ENDOCRINOLOGY
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The findings of this study might provide a reference for making new primary care strategies and complex family care plan to address the specific needs of different subgroups.
All data of the subjects were collected from National Health and Nutrition Examination Surveys database, and some of the data were self-reported, which might result in bias.
The results were based on the data in the population from the USA, whether the findings were suitable for the population from other regions remains to be elucidated.
Introduction
Multimorbidity refers to the presence of two or more diseases in an individual.1 Nowadays, the prevalence of multimorbidity is rising as the increase of population ageing.2 Previous studies indicated that nearly 15% of American adults were suffered from multimorbidity, and worse still, the multimorbidity is occurring at more and more younger people.3 4 Multiple studies agreed that individuals with multimorbidity were associated with worse quality of life, increased functional decline, higher risk of psychological distress or depression and even increased risk of death.5 6 Additionally, the medical expenses of multimorbidity also caused substantial burden to the society.7 More attention should be paid to identify patients with high risk of multimorbidity and disease screening should be conducted to early identify multimorbidity.
Identifying the specific patterns can help clinicians predict the risk of multimorbidity in patients and provide timely interventions to prevent the occurrence of multimorbidity.8 Previously, several studies have focused on exploring the multimorbidity patterns. Lee et al identified that the prevalence of multimorbidity in the overall population was 34.8%, and hypertension had the highest prevalence in both men and women based on the data from Korea Health Panel.9 Another study found that the most prevalent multimorbidity patterns among adults were cardiorespiratory, metabolic and mental-articular diseases.10 Researches also revealed that the multimorbidity patterns might differ due to the influences of sociodemographic characteristics, and socioeconomic status, regions or behavioural lifestyles.11 The multimorbidity patterns in different regions still need investigation. Currently, studies have explored the prevalence of multimorbidity in population from the USA.12 13 However, the detailed multimorbidity patterns and the association with frequency diseases in the USA were still unclear.
In previous studies, the main analytical methods for the epidemiological studies were to describe the simple prevalence and data of diseases or use cluster analysis.14 15 Association rule mining is a data mining technique for identifying association rules by extracting simple structures from large transaction databases, which helps discover hidden associations among frequent patterns of items in the database.16 Network analysis was extensively applied in human disease as network graphics directly show the connections of diseases in multimorbidity.17 This study was aimed to explore the prevalence of different frequency diseases and the associations with frequency diseases in population with different genders and different age ranges from the USA via the association rules and network analysis based on the data from National Health and Nutrition Examination Surveys (NHANES).
Methods
Patient and public involvement statement
Not applicable.
Study design and population
In total, 17 192 people aged ≥20 years with data on each disease were involved in this cross-sectional study and their data were extracted from NHANES database from 2013 to 2014 (n=5924), 2015 to 2016 (n=5735) and 2017 to 2018 (n=5533). NHANES, conducted by the Centers for Disease Control, is a continuous, biannual survey including non-institutionalised people in the USA among a nationally representative sample.18 After excluding patients without demographic data and patients without diseases information, 12 576 patients were finally included for further analysis. All private information of the participants has carried out the desensitisation.
Data collection
The data of all subjects were collected including age (years), age category (<65 years or ≥65 years), race (Mexican American, other Hispanic, non-Hispanic white, non-Hispanic black, non-Hispanic Asian or other race), education (less than 9th grade, 9–11th grade (including 12th grade with no diploma), high school graduate/general equivalent diploma or equivalent, some college or associate of arts (AA) degree or college graduate or above), marital status (married or not married), ratio of family income to poverty and numbers of morbidities.
The analysed diseases in the current study including hearing impairment, visual impairment, renal failure, asthma, arthritis, coronary heart disease (CHD), stroke, thyroid problems, gout, chronic bronchitis, liver problems, chronic obstructive pulmonary disease (COPD), malignant tumours and depression were selected according to the prevalence of non-communicable diseases from the GBD 2019 Data Input Sources Tool website (http://ghdx.healthdata.org/gbd-2019/data-input-sources). These conditions were reported with high prevalence based on the data on the GBD 2019. The GBD 2019 database included the statistical data of 369 diseases and 87 risk factors in 204 countries and territories.19 Some common diseases with high prevalence reported in previous studies were also analysed, including hypertension,20 heart failure (https://amj.amegroups.com/article/view/5475), emphysema,21 heart attack,22 kidney stones23 and sleep disorders.24 Finally, the analysed conditions in the present study were hearing impairment, visual impairment, renal failure, asthma, arthritis, CHD, stroke, thyroid problems, gout, chronic bronchitis, liver problems, COPD, malignant tumours, depression, hypertension, heart failure, emphysema, heart attack, kidney stones and sleep disorders. The codes of respective diseases are shown in online supplemental table 1.
Association rules analysis
Association rule learning was applied for exploring the associations between or among diseases.25 Association rule learning is a data mining technique showing how discrete variable values co-occur within datasets.26 For each participant in the data, each variable value is represented as observed or not observed. Variable values co-occurring in at least a specified proportion of the data sets (ie, ‘support’) are grouped together into ‘itemsets’. Rules (ie, ‘If the independent variable is observed, then the dependent variable is also observed’) are obtained from the itemsets in line with their confidence level (ie, the proportion of times the independent variable occurs that dependent variable also occurs). ‘lift’ demonstrates whether a rule adds knowledge about the likelihood of observing a variable value. Lift values >1.0 indicate that the dependent variable is more likely to be observed when the independent variable is also observed relative to when the dependent variable is ever observed in the dataset.
Social network analysis of centrality analysis
Social network analysis was conducted to identify the association between the frequent diseases in men and women. Centrality analysis assessed the relationship between the analysed conditions of the network structure and diseases that appear simultaneously. Degree, betweenness and closeness were indexes of centrality.27 In the network, the degree of centrality of disease refers to a direct association with other diseases. The betweenness of disease represents its mediating role in the network. The closeness of a disease refers to the number of steps from other diseases in the network. A higher closeness suggests a higher risk of being diagnosed with the associated disease with fewer steps. Further, the diameter of the node is proportional to the prevalence of the disease, and the thickness of the edge indicates the strength between two linked diseases.
Statistical analysis
The measurement data were expressed by Mean±SE, and comparisons between groups were performed by t-test. Categorical variables were described as n (%) and the comparisons between groups were performed by χ2 test. Statistical tests in the SURVEYFREQ and SURVEYMEANS were applied to calculate the weighted mean and frequency. The association rule analyses were completed by R V.3.6.3, analysed through R arules and R aruleViz and visualised by network analysis. All association rules were screened out by support >4% and confidence >60%. The random seed was 2021. Statistical analyses were performed using SAS V.9.4 via a two-sided test and α<0.05 was set as statistical significance.
Results
The characteristics of all subjects
The data of 17 192 participants were extracted from NHANES database. Among them, 3139 patients lacking the demographic data and 1477 patients lacking the diseases information were excluded. Finally, 12 576 patients were involved. The screen process is exhibited in figure 1. The average age of all participants was 47.5 years. In the total population, 4040 (32.6%) have some university degree or AA degree, 1801 (30.5%) of the males have some university degree or AA degree and 2239 (34.7%) of the females have some university degree or AA degree. The average ratio of family income to poverty in all people was 3.3 (table 1). The average number of morbidities was 2.4 in all subjects, 2.2 in the males and 2.5 in the females. Two thousand five hundred and seven (31.00%) people with multimorbidity were ≥60 years. Three thousand six hundred and eighty-nine (53.7%) participants with multimorbidity were females. Three thousand one hundred and fifty-six (72.4%) subjects with multimorbidity were non-Hispanic white. Two thousand two hundred and ninety-two (33.9%) of them had college experience or AA education. The average ratio of family income to poverty in patients with multimorbidity was 3.1 (table 2).
The characteristics of all subjects
Comparisons of the characteristics in people with and without multimorbidity

The screen process of the participants in our study. NHANES, National Health and Nutrition Examination Surveys.
The prevalence of diseases
Among all the included diseases, high cholesterol had the highest prevalence (33.4%), followed by hypertension (32.4%), sleep disorders (30.2%) and arthritis (26.8) (figure 2, table 3). Subgroup analysis in terms of gender and age showed that among males <65 years, high cholesterol had the highest prevalence (30.1%), followed by hypertension (27.1%) and sleep disorders (25.7%). Among males ≥65 years, high cholesterol (57.9%) and hypertension (56.5%) showed high prevalence, followed by arthritis (47.1%). The highest prevalence among women <65 years was sleep disorder (32.1%), followed by hypertension (24.6%) and high cholesterol (24. 6%). As for the number of conditions in all population, 24.0% of them had no multimorbidity included in our study, 21.8% of the subjects had one of the conditions and 16.4% of the participants had two of the multimorbidity (figure 3). The highest prevalence among women aged ≥65 years was hypertension (63.9%), followed by arthritis (63.4%) and high cholesterol (60.9%) (figure 4, table 4). Among males aged <65 years, 30.9% of them did not have the included multimorbidity, 25.2% of them had one multimorbidity and 17.2% of them had two multimorbidities. In males aged ≥65 years, 16.7% of them had four multimorbidities, 16.1% had three multimorbidities and 14.2% had two multimorbidities. Among females aged <65 years, 27.1% of them were without multimorbidity, 24.6% of them had one multimorbidity and 16.9% had two multimorbidities. In females aged ≥65 years, the proportions of subjects who had four multimorbidities, three multimorbidities and two multimorbidities were 19.0%, 16.8% and 12.6%, respectively (figure 5, table 4).

The prevalence of diseases in all population. COPD, chronic obstructive pulmonary disease.
The prevalence of diseases

The prevalence of number of conditions in all population.
Number of multimorbidities in the participants

The prevalence of diseases in people with different genders or ages. COPD, chronic obstructive pulmonary disease.

The prevalence of number of conditions in people with different genders or ages.
Association rules analyses between two diseases
The association rules were analysed between two diseases, and the results revealed that the probability for hypertension and high cholesterol was the highest, with a support of 36.2%, followed by arthritis and hypertension with a support of 29.4%, and diabetes and hypertension with a support of 18.1% (table 5). Among females, the probability for hypertension and high cholesterol was 34.6%, arthritis and hypertension was 33.1%, and diabetes and hypertension was 16.1% (table 6). In terms of males, the probability for hypertension and high cholesterol was 38.0%, arthritis and hypertension was 25.2%, and diabetes and hypertension was 20.3% (table 7).
Association rules analyses between two diseases in total population
Association rules analyses between two diseases in total population in females
Association rules analyses between two diseases in total population in males
Network analysis of the associations between two diseases
The centrality analysis was applied to show the visualisation of each node’s influence within the network. Hypertension displayed the highest betweenness centrality followed by high cholesterol and arthritis (figure 6). In females, hypertension, arthritis and high cholesterol were the top two diseases of degree centrality (figure 7). In males, the highest degree betweenness centrality was hypertension followed by high cholesterol (figure 8). For males aged <65 years, hypertension and high cholesterol presented the highest betweenness centrality (figure 9). In males ≥65 years, hypertension, high cholesterol and arthritis were the top three diseases of degree centrality (figure 10). In females <65 years, only three association rules were identified, which were diabetes and high cholesterol, diabetes and hypertension, and depression and sleep disorder (figure 11). As for females ≥65 years, hypertension showed the highest betweenness centrality followed by high cholesterol and arthritis (figure 12).

Network diagram of multimorbidity in all population. Bigger dot indicated higher support and deeper colour indicated higher lift. COPD, chronic obstructive pulmonary disease. LHS: left-hand-side, RHS: right-hand-side.

Network diagram of multimorbidity in females. Bigger dot indicated higher support and deeper colour indicated higher lift. COPD, chronic obstructive pulmonary disease. LHS: left-hand-side, RHS: right-hand-side.

Network diagram of multimorbidity in males. Bigger dot indicated higher support and deeper colour indicated higher lift. COPD, chronic obstructive pulmonary disease. LHS: left-hand-side, RHS: right-hand-side.

Network diagram of multimorbidity in males aged <65 years. Bigger dot indicated higher support and deeper colour indicated higher lift. COPD, chronic obstructive pulmonary disease. LHS: left-hand-side, RHS: right-hand-side.

Network diagram of multimorbidity in males ≥65 years. Bigger dot indicated higher support and deeper colour indicated higher lift. LHS: left-hand-side, RHS: right-hand-side.

Network diagram of multimorbidity in females aged <65 years. Bigger dot indicated higher support and deeper colour indicated higher lift. COPD, chronic obstructive pulmonary disease. LHS: left-hand-side, RHS: right-hand-side.

Network diagram of multimorbidity in females ≥65 years. Bigger dot indicated higher support and deeper colour indicated higher lift. LHS: left-hand-side, RHS: right-hand-side
Multiplematrix of the associations among diseases
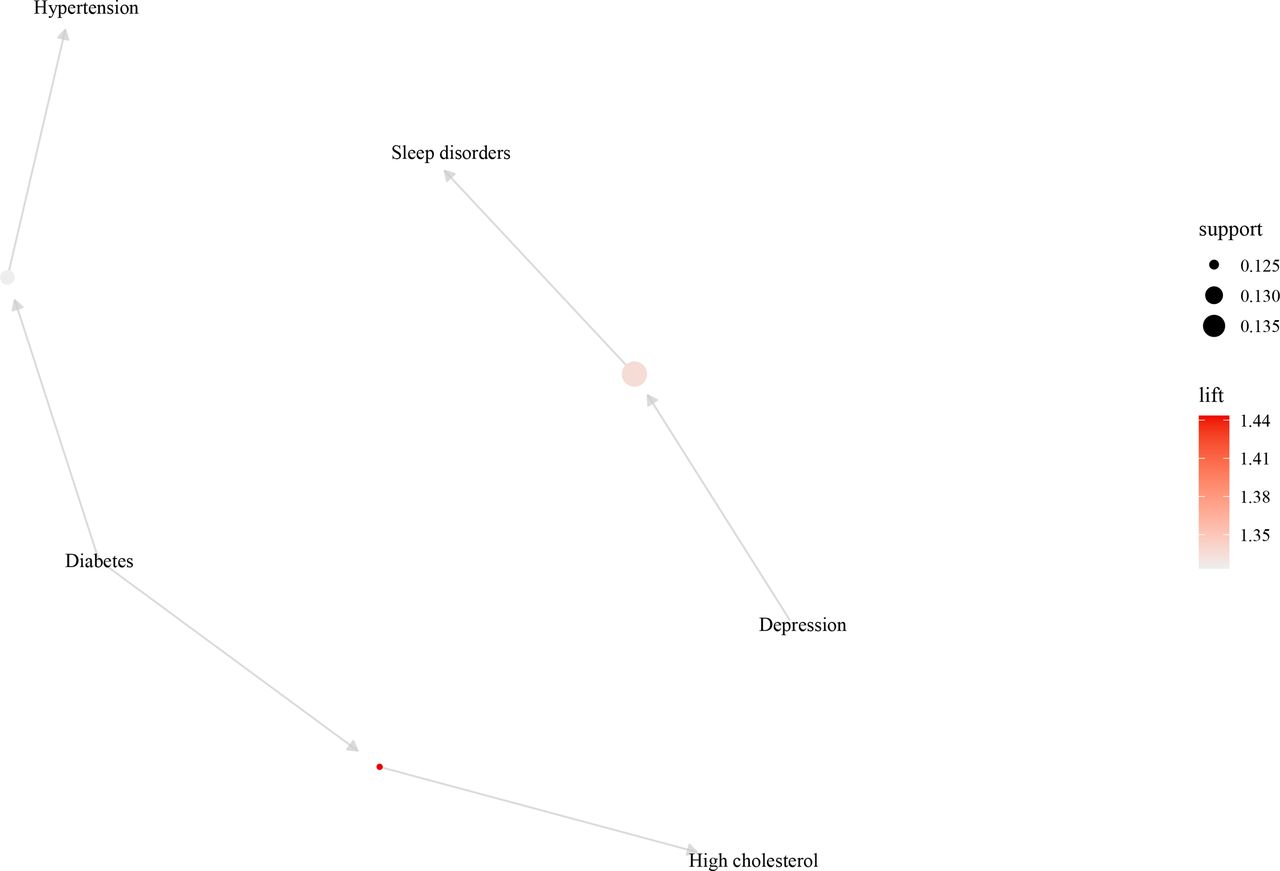
When observing the associations among multiple diseases, the associations of depression with sleep disorder had the highest lift and high support. The associations of hypertension, arthritis and one other item with high cholesterol presented the highest support (figure 13). In males, the associations of depression, hypertension with sleep disorders had the highest lift, the associations of hypertension, kidney stones, two other items with high cholesterol, and the associations of sleep disorders, kidney stones and other two items with hypertension showed high support (figure 14). Among females, the associations of depression, arthritis with sleep disorders had the highest lift, the associations of kidney stones, vision problems, other five items with hypertension exhibited the highest support (figure 15). In males <65 years, the associations of emphysema with COPD had the highest support, followed by heart attack, high cholesterol with CHD (figure 16) while in males ≥65 years, the associations of hypertension, sleep disorder with arthritis exhibited the highest lift (figure 17). In females <65 years, the associations of arthritis, depression and one other item with sleep disorder presented the highest lift followed by depression, high cholesterol and one other item with sleep disorder (figure 18). In terms of females ≥65 years, the associations of chronic bronchopneumonia, sleep disorders with asthma had the highest lift, followed by chronic bronchopneumonia, arthritis with pneumonia (figure 19).

Multiplematrix of the associations among diseases in all population. Bigger dot indicated higher support and deeper colour indicated higher lift. More arrows pointed to the disease indicated the disease had higher possibility to co-occur with other disease. COPD, chronic obstructive pulmonary disease.

Multiplematrix of the associations among diseases in females. Bigger dot indicated higher support and deeper colour indicated higher lift. More arrows pointed to the disease indicated the disease had higher possibility to co-occur with other disease. COPD, chronic obstructive pulmonary disease.

Multiplematrix of the associations among diseases in males. Bigger dot indicated higher support and deeper colour indicated higher lift. More arrows pointed to the disease indicated the disease had higher possibility to co-occur with other disease. COPD, chronic obstructive pulmonary disease.

Multiplematrix of the associations among diseases in males aged <65 years. Bigger dot indicated higher support and deeper colour indicated higher lift. More arrows pointed to the disease indicated the disease had higher possibility to co-occur with other disease. COPD, chronic obstructive pulmonary disease.

Multiplematrix of the associations among diseases in males ≥65 years. Bigger dot indicated higher support and deeper colour indicated higher lift. More arrows pointed to the disease indicated the disease had higher possibility to co-occur with other disease. COPD, chronic obstructive pulmonary disease.

Multiplematrix of the associations among diseases in females aged <65 years. Bigger dot indicated higher support and deeper colour indicated higher lift. More arrows pointed to the disease indicated the disease had higher possibility to co-occur with other disease.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Multiplematrix of the associations among diseases in females ≥65 years. Bigger dot indicated higher support and deeper colour indicated higher lift. More arrows pointed to the disease indicated the disease had higher possibility to co-occur with other disease.
Discussion
In our study, the prevalence of multimorbidity and the associations between or among multimorbidity were assessed with a large sample size from the US population. We initially explore the multimorbidity patterns through association rules analysis, which can identify the associations among frequent patterns of items in the database. The results depicted that for males aged <65 years, hypertension and high cholesterol presented the highest possibility to have most number of multimorbidity while in males ≥65 years, hypertension, high cholesterol and arthritis were the top three diseases of possibility to be associated with other diseases. As for females ≥65 years, hypertension showed the highest possibility to have most number of multimorbidity followed by high cholesterol and arthritis. In males <65 years old, the associations of emphysema with COPD had the highest possibility to occur with other diseases, followed by heart attack, high cholesterol with CHD while in males ≥65 years, the associations of hypertension, sleep disorder with arthritis exhibited the highest chance to co-occur. In females ≥65 years, the associations of chronic bronchopneumonia, sleep disorders with asthma had the highest chance to co-occur, followed by chronic bronchopneumonia, arthritis with pneumonia. The findings of our study might help the clinicians identify patients with high risk of multimorbidity and provide reference for making plans and trageties to better manage people who already had one or more conditions.
Herein, the prevalence of multimorbidity was about 55.3% in all participants. Previous studies reported that the prevalence of multimorbidity was 69.5% in Mexican aged 25–75 years28 and 72.7% in adults at a primary care centre in Portugal.29 Weiss et al idenitifed that the majority of participants experiencing each disease had at least one other coincident disease among older adults in the USA.30 Ward et al revealed that 64% of adults have multiple chronic conditions among US adults.31 These results were higher than our study, which may result from the differences in age or regions. In this study, the prevalence of multimorbifity in females was higher than in males, which was supported by several studies. Yao et al identified that the prevalence of individual chronic diseases and multimorbidity was higher in females than males in Chinese population.15 Another cross-sectional analysis on Iranian people also revealed that women were at 2.11-fold higher risk of multimorbidity.32 In previous studies, high cholesterol was commonly reported to be a prevalent disease in many countries and peoples.33 34 Hypertension was another prevalent disease with more than 1.2 billion patients all over the world.35 Koroukian et al found that among individuals aged 50–64 years, the most common condition was hypertension (50.0%), whether presenting with or without the co-occurrence of any other condition.36 Sleep disorders were a frequently identified disease in more and more people.37 These studies were allied with the findings in our study, which depicted that high cholesterol had the highest prevalence, followed by hypertension, sleep disorders. Additionally, we also identified that arthritis was more prevalent than sleep disorders in males ≥65 years. This was evidenced by previous studies, delineating that the older age was associated with increased risk of arthritis.38 39 Interestingly, in females <65 years, sleep disorders were the most prevalent diseases in the current study. Carone et al identified that females were associated with low-quality sleep and awakenings.40 This may be because of the influence of hormonal changes in females.41
In the present study, association rules analyses showed that hypertension and high cholesterol presented the highest probability of coexisting. Hypertension and high cholesterol levels were the most prevalent diseases in people.42 Previously, there was a study indicated that hypertension, hyperlipidaemia and CHD, which together were present in 37% of men and hypertension, hyperlipidemia and arthritis were co-occurred in 25% of women.43 A Polish multicentre national health survey discovered that comorbid hypertension and hypercholesterolaemia was high in participants aged 19–99 years (2037 patients among 5939),44 which gave support to the results in this study. There was evidence showing that hypertension was independently associated with arthritis.45 Quiñones et al identified that hypertension and arthritis was one of the most prevalent combinations,46 which was allied with the results in our study, revealing that arthritis accompanied with hypertension was the second prevalent multimorbidity. Quiñones et al also found that hypertension, arthritis and diabetes was another prevalent combination, this may be because the included samples were older adults aged ≥65 years. These findings suggested that when people had one of these conditions, frequent detection and timely interventions such as lifestyle changing should be provided to prevent the occurrence of multimorbidity. Yamazaki et al reported that diabetes mellitus and hypertension are frequently present together.47 This provided evidence to the findings in the current study, which found that diabetes mellitus complicated with hypertension were prevalent patterns of multimorbidity. In addition, network analyses in the current study discovered that the possibility of complicating with hypertension was the highest followed by high cholesterol regardless of age. In this study, the analysis on associations in two or more than two diseases revealed that depression and sleep disorders had the highest association among all the diseases in all participants. In males, depression, hypertension and sleep disorders presented the highest associations and in females, depression, arthritis and sleep disorders exhibited the highest associations. These suggested that depression was closely associated with sleep disorders in both males and females. Sleep problems are frequently regarded as one of the major diagnostic criteria for many mental disorders including depression, and continuous sleep problems might increase the risk of relapse, recurrence in depression patients.48 For people with sleep disorders, appropriate medications should be provided to alleviate sleep problems, improve sleep quality and prevent the occurrence of depression.
The multimorbidity was more than two common diseases with high prevalence, which influenced large numbers of people all over the world. To deep investigate the detailed multimorbidity patterns can help identify people having one or more of these diseases with high risk of developing into multimorbidity. Previous epidemiological studies mainly explored the simple prevalence and just interpret the incidence data.49 Association rules analysis and social network analysis of centrality could discover and predict rules between diseases and help identify highly connected conditions in multimorbidity networks, respectively.17 50 Association rules analysis and social network analysis of centrality could help easily identify the prevalence of two or more conditions, as well as the high prevalence of multimorbidity, or the most prevalent condition in those with multimorbidity. More attentions should be paid on patients who had one of these conditions and appropriate measures should be taken to prevent the occurrence of multimorbidity. Frequent detection should also be conducted to early identify the multimorbidity and provide timely treatments for improving the prognosis of these patients. In addition, subgroup analyses were performed in terms of gender and age, and diseases prevention and treatment can be more targeted to different groups of people.
There were several limitations in the present study. First, all data of the subjects were collected from NHANES database. Some of the data were self-reported, and the survey was conducted long time after the information occurred, and the participates might not clearly remember the actual results, which might result in recall bias between the accuracy or completeness and the real situation. Second, the results were based on the data in the population from the USA, whether the findings were suitable for the population from other regions remains to be elucidated. Third, currently, there was still no methods to incorporate complex sampling design effects into association rules. In the future, studies with large scale of sample size were required to verify the results in this study.
Conclusions
In the current study, the prevalence and patterns of multimorbidity in the US population were investigated. Subgroup analyses were conducted in different genders and ages. The results delineated that hypertension and high cholesterol were prevalent diseases in all population, regardless of females and males. Hypertension and high cholesterol, arthritis and hypertension, and diabetes and hypertension were more likely coexisting. The findings of this study might provide a reference for making new primary care strategies and complex family care plan to address the specific needs of different subgroups.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study did not need to be approved by the Institutional Review Board of the Daping Hospital, Army Medical University because the data were accessed from NHANES (a publicly available database).
References
Footnotes
Contributors ZZ and LC designed the study. ZZ wrote the manuscript. YX, JH, XS and RZ collected, analysed and interpreted the data. LC critically reviewed, edited and approved the manuscript. All authors read and approved the final manuscript. LC is responsible for the overall content as guarantor.
Funding This work is supported by research funding from the National Key Research and Development Program of China (2018YFA0800802), the National Natural Science Foundation of China (No. 81830075, 82122044, 81772306, 81721001) and Key research and development projects of science and technology innovation of social undertakings and people's livelihood security in Chongqing (cstc2017shms-zdyfX0027)
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.