Article Text

Abstract
Introduction An estimated 290 million people are living with hepatitis B virus (HBV) worldwide; in Spain, the prevalence of hepatitis B virus surface antigen (HBsAg) is 0.4%. In our setting, many HBsAg-positive individuals are not linked to care, which implies a barrier to receiving treatment and controlling the infection. The main objective of this project is to evaluate the performance of a programme designed to achieve appropriate linkage to specialist care of HBsAg-positive individuals, newly tested or previously tested and lost to follow-up.
Methods and analysis This is a retrospective and prospective study in which all HBsAg-positive cases recorded in the microbiology database will be identified. The retrospective phase will include cases detected between 2018 and 2020, and the prospective phase will run from January 2021 to June 2022. The project will be carried out in a tertiary university hospital covering the northern health area of Barcelona with a catchment population of 450 000 inhabitants and 16 affiliated primary care centres. The central laboratory detects approximately 1200 HBsAg-positive individuals every year; therefore, we expect to identify around 4000 patients over the duration of the project. The medical records of HBsAg-positive individuals will be consulted to identify and retrieve those who have not been appropriately linked to care. Candidates will be contacted to offer specialist disease assessment and follow-up. A website will be created to provide HBV-related information to primary care physicians, and a mobile phone application will be available to patients to improve the linkage circuits and ensure follow-up continuity.
Ethics and dissemination The Vall d’Hebrón Hospital Ethics Committee (PR(AG)201/2021) and the Spanish Agency of Medicines and Medical Devices approved this study. The findings will be disseminated through peer-reviewed publications and conference presentations. This programme could increase the number of HBsAg-positive individuals properly linked to care and achieve better HBV monitoring, which will have a positive impact on WHO’s viral hepatitis elimination goals.
- VIROLOGY
- Telemedicine
- Hepatology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
A large number of hepatitis B virus surface antigen-positive individuals in a specific area will be included.
The tools used in the programme to facilitate healthcare communication and promote adherence to follow-up are based on information technology.
The potential impact of the COVID-19 pandemic on linkage to care is a limitation that may have been mitigated with the new tools applied.
Introduction
Hepatitis B virus (HBV) infection remains a major global health problem.1 Chronic HBV infection affects around 290 million people worldwide and is a leading cause of cirrhosis, hepatocellular carcinoma,2 liver transplantation requirement and liver-related deaths, accounting for more than 800 000 deaths annually.3 The Spanish population has an estimated hepatitis B virus surface antigen (HBsAg) prevalence of 0.4%,4 and this figure is likely to increase due to considerable immigration from regions where HBV is endemic.5 Although highly effective hepatitis B vaccines are available and prevention of viral transmission has improved,6 HBV infection remains a major cause of acute hepatitis7 and is associated with a high health and economic burden.8
Hepatitis B is usually an asymptomatic infection,9 and this may explain why a large percentage of infected individuals are unaware of their condition. In 2019, only 10% of people with HBV infection worldwide had been diagnosed, and 22% of them (6.6 million people) were receiving treatment,3 even though HBV therapy is orally administered, well tolerated and effective in suppressing viral replication in almost all cases.10 Elimination of hepatitis B is a goal of the WHO, and early identification of infected individuals and linkage to care are crucial to achieve this objective.11 Hence, it is essential to design new strategies that involve both the patient and the primary care physician (PCP) to ensure proper HBV management through regular contacts, motivational tactics and simplified access to the specialist linkage circuit.
Vall d’Hebrón Hospital in Barcelona is a tertiary university hospital with a catchment population of 450 000 inhabitants and 16 affiliated primary care centres. Around 1200 HBsAg-positive individuals are detected every year in its central laboratory, which receives samples from the hospital and primary care, and many of them do not reach appropriate specialist evaluation of their liver disease or the need for HBV treatment. Linkage of these patients to appropriate specialist follow-up will have a positive impact on the course of their infection and WHO’s viral hepatitis elimination goals.
The goal of this project, called LINK-B, is to achieve linkage to specialist care of documented HBsAg-positive patients in the Vall d'Hebrón health area. The secondary aims are to determine the barriers to linkage in patients with HBV and to set up comprehensive, effective, hepatitis B guidance and referral pathways in collaboration with primary care professionals.
Methods and study design
Study design
This will be a single-centre, two-part, retrospective and prospective study. In the retrospective part, a list of HBsAg-positive cases recorded in the laboratory between January 2018 and December 2020 will be reviewed, and in the prospective part all positive cases identified between January 2021 and June 2022 will be recorded (online supplemental figure S1). In total, we expect to collect around 4000 HBsAg-positive individuals. A dedicated registry will be set up to record their data. Patients’ medical records will be evaluated by a physician or expert nurse to determine whether they have been linked to specialist care.
Supplemental material

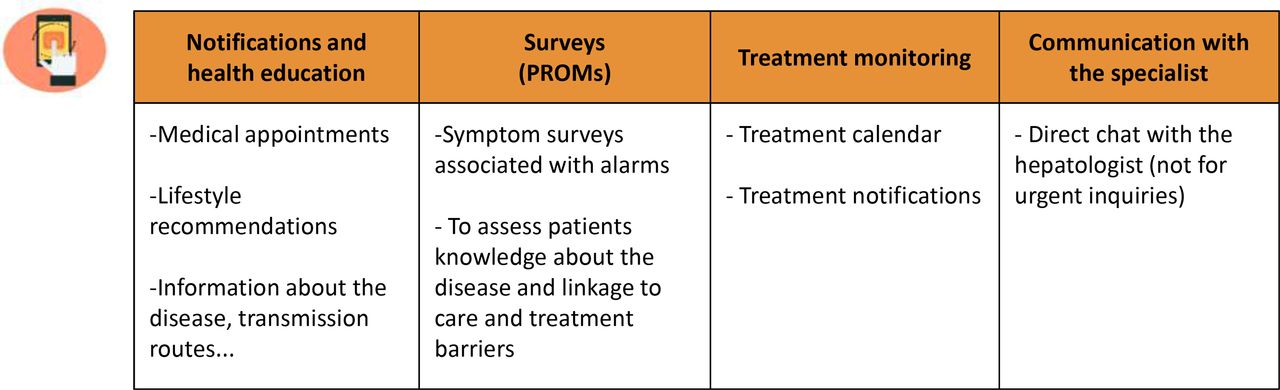
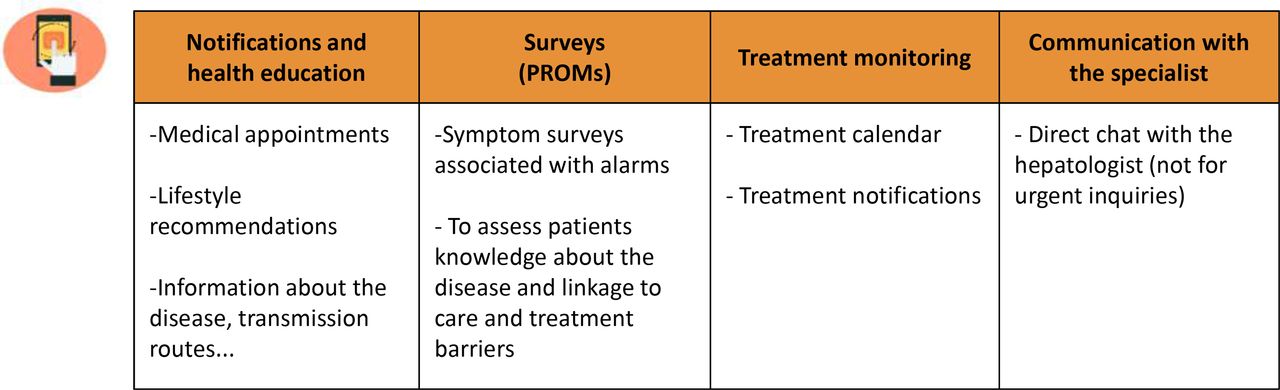
Information technology tools developed as part of the project and the main uses. HBV, hepatitis B virus.
A nurse will initially call patients who have not been linked (maximum of five attempts per patient). If patients cannot be contacted by telephone, a letter will be sent to their home address. In both the telephone and letter contact, patients will be informed of the date and time of their visit with a hepatologist to review their HBsAg-positive status (figure 1, online supplemental figure S2). In patients who meet the European Association for the Study of the Liver hepatitis B treatment criteria,1 oral nucleos(t)ide analogues will be provided according to clinical guidelines. Subsequent visits will be scheduled at the discretion of the hepatologist, depending on the clinical situation of each patient. In addition, a simplified referral pathway will be available to PCPs, who can directly contact the study nurse to set up the appointment with the hepatologist. In patients already linked to care and receiving adequate follow-up, no further interventions will be undertaken.
Supplemental material
{kind=link}
{kind=link}
Phone application (app) features shared with patients. PROMs, Patient Reported Outcomes Measures.
Information technology
New information and communication technologies have proven useful in medicine in promoting adherence to follow-up and treatment by personalising care and actively involving the patients.12 13 Use of these tools could improve follow-up of HBsAg-positive individuals.
A web-based site will be designed to provide medical information and enable direct contact between PCPs, nurses and hepatologists. Educational programmes, including scientific material and linkage pathways, will be designed in collaboration with PCPs and incorporated in the website to guide physicians in decision-making. The medical information provided will include answers to frequently asked questions about hepatitis B, algorithms for management of patients with HBV infection in various clinical situations, information on HBV prevention and indications for treatment, and news or new relevant information on viral hepatitis. To introduce the website to PCPs, a meeting will be held with representative physicians from all primary care centres belonging to the Vall d’Hebrón Hospital health area. The reasons for inadequate linkage will be documented by a patient-reported survey, taking into account the characteristics of the patients and the health providers. The website will be hosted on the general website of Vall d’Hebrón Hospital and will be accessible to all PCPs in the hospital’s health area.
In addition, a mobile phone application (app) will be created and offered to all patients who attend the first visit with a hepatologist at our centre and who meet the criteria required for its use (eg, they understand the language of the app, they correctly handle the mobile device). The app is an adaptation of an app called NORA previously designed by our hospital’s neurology department and used in patients who had stroke.13 It can be downloaded from all mobile servers, but requires credentials (given to each patient individually) for use. The app will provide information on HBV infection, remind participants about visits and blood tests, and monitor HBV therapy in those requiring medication (figure 2). The app will also allow communication between patients and the hepatology team on issues related to HBV infection through a chat that will be answered within 48 hours. Doubts or queries will be resolved by the nurse or by the hepatologist if necessary. The app also includes questionnaires regarding quality of life and adherence to medication, as well as patient surveys on linkage-to-care issues. Patients will be trained in the use of the app so they can take full advantage of its support.
Methods
Demographic and clinical variables will be recorded: sex, age, ethnicity, risk factors for HBV infection, social situation, comorbidities, geographical area, reference health centre, duration and stage of HBV infection, degree of fibrosis, presence of hepatocellular carcinoma (HCC), and HBV therapy (eg, duration, drugs, side effects). We will also record whether patients were aware of having HBV infection, whether they received a diagnosis but were not linked to care, and the reasons for lack of linkage and treatment.
Laboratory parameters will include HBsAg, quantitative hepatitis B surface antigen, hepatitis B e antigen, hepatitis B core-related antigen, HBV DNA levels, hepatitis B e antibodies, hepatitis B surface antibodies, hepatitis B core antibodies, HIV antibodies and hepatitis C virus antibodies, as well as haematological and biochemical parameters such as platelet count, prothrombin time, international normalised ratio, bilirubin, creatinine, alanine aminotransferase, aspartate aminotransferase, gamma-glutamyltransferase, alkaline phosphatase, albumin, gamma globulin, FIB-4 score and APRI. In addition, liver imaging results (ultrasound, CT), liver stiffness measurement, and endoscopy and liver biopsy findings will be collected. Data will include information recorded at the time of the diagnosis and during monitoring and treatment of all HBsAg-positive individuals.
Patients meeting the linkage criteria will be scheduled for a blood test and a visit with the hepatologist at the hospital. In the initial visit, a thorough anamnesis will be performed. All analytical parameters will be reviewed and fibrosis will be evaluated by non-invasive methods (serology and transient elastography). In patients whose condition requires treatment, nucleos(t)ide analogues will be prescribed. In addition, patients will be informed about the app and offered the possibility to use it by creating a user account. The next visits and complementary examinations will be scheduled at the discretion of the hepatologist. Patients who are considered not to need follow-up in the hospital after appropriate evaluation by the specialist can be followed up by the PCP. Patients can also request this option.
Patient and public involvement
No patients were involved in the design, recruitment or performance of this study.
Statistical analysis
An Excel table will support all the data in coded form, in which patients’ personal data will not be identifiable. Normally distributed quantitative variables will be compared using Student’s t-test and expressed as mean±SD. Variables with a non-normal distribution will be analysed using the Mann-Whitney U test and expressed as median and IQR. Categorical variables will be compared using the χ2 test or Fisher’s exact test when frequencies are less than 5%, and expressed as frequencies and percentages. Statistical significance will be set at a p value of <0.05. All statistical analyses will be carried out using IBM SPSS V.20.
Ethics and dissemination
This study complies with the criteria of the Vall d’Hebrón Hospital Ethics Committee (reference number PR(AG)201/2021) and the Spanish Agency of Medicines and Medical Devices, and will be conducted according to the principles of the Declaration of Helsinki, Good Clinical Practice guidelines and local regulatory requirements. Informed consent forms will be provided to participating individuals and all data will be anonymised.
Study outcomes
The primary endpoint of the study will be the number of HBsAg-positive individuals identified retrospectively and prospectively and linked to specialist care through our dedicated programme for this purpose. Linkage to care is defined as attendance to the first visit with a hepatologist. The secondary outcomes will include the number of patients meeting the treatment criteria and the number who initiate treatment. We also wish to evaluate the impact of information technology on the success of linkage to care and on PCPs’ knowledge of the referral circuit. Hence, additional outcome measures will include the number of patients using the app, the degree of adherence to follow-up and treatment, the use of the website by PCPs, the number of patients referred to the hepatologist by PCPs and the number of patients who initiate treatment through the established circuits. The degree of adherence to follow-up and treatment will be evaluated through records of medical visits attended by the patient, as well data from the app section that allows monitoring of medication intake. Finally, to detect critical points that limit linkage to care and potential solutions to improve access to treatment, we will record the specific reasons why each patient has not been linked, together with their demographic and clinical characteristics.
Applicability
Even though our publicly funded healthcare system provides an adequate interconnection between primary and specialised care that facilitates patient linkage, it is expected that a substantial percentage of HBsAg-positive individuals will not have been appropriately linked to specialist consultation. This programme could be the first step to develop a community service for hepatitis B similar to the highly successful programmes developed for patients with hepatitis C virus.14 15
The COVID-19 pandemic has had a considerable impact on access to healthcare, and this situation lends importance to projects aimed at actively linking patients to follow-up. In circumstances where face-to-face meetings are complex or even risky, information platforms that can help PCPs resolve doubts and make decisions regarding HBV infection are of particular value. Furthermore, the use of mobile phone apps that contribute to patients’ autonomy and comfort can be very useful in reinforcing adherence to medication and follow-up.
In summary, this project aims to ensure adequate linkage to follow-up and treatment of patients with HBV infection, while investigating the use of information and communication technologies to improve the care of these patients. One of the main contributions will be to establish an appropriate, simplified referral circuit in collaboration with PCPs in order to improve communication between professionals and ensure correct identification and care of patients with HBV.
If the circuit and information tools employed show positive results in relation to the management and follow-up of individuals with hepatitis B infection, this programme is also expected to have a positive impact on the course of their infection and on WHO’s elimination targets.
Ethics statements
Patient consent for publication
Acknowledgments
English writing support was provided by Celine Cavallo.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
ABD and AR are joint first authors.
Contributors ABD, MB and MR-B conceived the project. ABD, MB and MR-B drafted the project protocol. AB drafted the first version of the manuscript with assistance from MB and MR-B. ABD, AR, AF-P, AP, FR-F, EV-A, JV-R, NP, MR-B, RE and MB have reviewed the full draft of the article and subsequent revisions and have approved the final version for submission.
Funding This project is supported by Gilead Sciences through the competitive research 'HBV Treat' (protocol number IN-ES-320-6107).
Competing interests MB has served as a speaker and advisory board member for Gilead, Roche and Arbutus. MR-B has served as a speaker for AbbVie and Gilead. RE has served as a speaker and advisory board member for Gilead, Roche and Arbutus.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.