Article Text

Abstract
Introduction Postmenopausal osteoporosis, caused by ageing and oestrogen deficiency, seriously threatens women’s physical and mental health. Postmenopausal osteopenia is the transition from healthy bone to osteoporosis, and it may be the key period for preventing bone loss. Moxibustion, a physical therapy of Traditional Chinese Medicine, has potential benefits for osteoporosis treatment and prevention, but it has not been adequately studied. This study aims to explore the clinical effects and safety of moxibustion in delaying bone loss in postmenopausal women.
Methods and analysis In this parallel-design, randomised, patient-blind and assessor-blind, controlled clinical study, 150 women with osteopenia at low fracture risk will be randomly assigned to a moxibustion treatment (MT) group or a placebo-moxibustion control (PMC) group in a 1:1 ratio. In addition to the fundamental measures (vitamin D3 and calcium) as recommended by the guidelines, participants of the two groups will receive MT or PMC treatment for 42 sessions over 12 months. The primary outcome will be the bone mineral density (BMD) of the lumbar spine at the end of the 12-month treatment, and secondary outcomes will be the BMD of the femoral neck and total hip, T-scores, bone turnover markers, serum calcium levels, serum magnesium levels, serum phosphorus levels, serum parathyroid hormone levels and 25-hydroxyvitamin D levels, intensity of bone pain, quality of life, incidence of osteoporosis and fractures, usage of emergency drugs or surgery, participant self-evaluation of therapeutic effects and the rate of adverse events. All statistical analyses will be performed based on the intention-to-treat and per-protocol principle.
Ethics and dissemination Ethics approval has been obtained from the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University (permission number: 2021-1243). The results are expected to be published in peer-reviewed journals.
Trial registration number ChiCTR2100053953.
- Bone diseases
- COMPLEMENTARY MEDICINE
- Protocols & guidelines
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study will be the first randomised controlled trial to investigate the clinical effects and safety of moxibustion in delaying bone loss in postmenopausal women with osteopenia.
The risk of bias will be reduced by rigorous methodology, including adequate randomisation, placebo-moxibustion control, blinded evaluation and proper statistical methods.
Because the double-blind of moxibustion is difficult to achieve for operators and patients who have had moxibustion treatment experience, the relatively feasible placebo moxibustion method will be adopted in this study.
This trial will not be a multicentre study and the results of the study may be influenced by geography.
Introduction
Osteoporosis (OP) is a common skeletal disease with pathological characteristics of decreased bone mass, destroyed bone microstructure, increased bone fragility and proneness to bone fracture.1 Primary OP can occur in both men and women at any age, but it most commonly occurs in women after menopause as endogenous oestrogen levels decline. Postmenopausal bone loss is closely related to oestrogen withdrawal.2 Oestrogen deficiency leads to increased secretion of receptor activator of nuclear factor kappa B ligand (RANKL) and decreased osteoprotegerin (OPG) in bone marrow mesenchymal stem cell,3 osteoblasts, osteocytes4 and bone lining cells.5 RANKL binds to RANK to recruit tumour necrosis factor (TNF) receptor-associated factor 6 and activate the downstream nuclear factor kappa and mitogen-activated protein kinase pathways, which in turn activate nuclear factor of activated T cells cytoplasmic 1, resulting in enhanced differentiation from bone marrow monocytes/macrophages to osteoclasts.6 7 Lack of oestrogen leads to low-grade inflammation, characterised by evaluated levels of interleukin (IL)-1, IL-6, IL-17 and TNF α (TNF-α).8–10 These inflammatory factors stimulate T cells, B cells, stromal cells and osteoblasts to secrete RANKL, indirectly enhancing the differentiation and proliferation of osteoclasts.11 12 In addition, oestrogen deprivation can trigger oxidative stress, which is a critical regulator for increased inflammatory factors and osteoclast inducible factors.13 14 Overall, oestrogen deficiency enhances osteoclast-mediated bone resorption and inhibits osteoblast-mediated bone formation, resulting in osteoblast-osteoclast imbalance and bone loss. The latest prevalence study from China has reported that the prevalence of OP was 20.6% among women aged 40 years or older, and as high as 32.1% in perimenopausal women.15 There is little reduction in bone mineral density (BMD) during premenopause or early perimenopause.16 However, BMD declines rapidly from late perimenopause to 5–10 years after menopause, resulting in a 10% reduction in bone mass compared with the young-adult mean (equivalent to a decrease of approximately 1.0 T-score unit) with an average loss of 1%–5% BMD per year.16–19 Because postmenopausal osteoporosis (PMOP) seriously threatens women’s physical and mental health,17 18 effective prevention of PMOP has important clinical, scientific and social value.
Calcium and vitamin D (CaD) comprise the basic prophylactic treatment in the management of postmenopausal osteopenia, which can decrease hip fracture occurrence compared with placebo control in postmenopausal women.20 Oestrogen, raloxifene and bisphosphonates are currently recommended as drugs to prevent PMOP.21 Hypo-oestrogenaemia of postmenopausal women is generally recognised as a major risk for PMOP. As a result, hormone replacement therapy (HRT) has been used to treat postmenopausal bone loss for almost 50 years.22 HRT protects bone during the treatment, especially increasing the distal radius BMD,23 but the protective effect rapidly diminishes after treatment cessation. With the increasing understanding of the side effects of oestrogen-related therapies on cardiovascular diseases and carcinogenesis of oestrogen receptor-α rich tissue, such as breast, ovary and uterus,24 25 oestrogen therapy has been rarely used clinically to prevent PMOP. Raloxifene, one of the selective oestrogen receptor modulators, has been approved by the FDA for preventing PMOP as well as for the reduction of breast cancer risk in women with PMOP.19 Previous studies have demonstrated that Raloxifene reduces the risk of spine fractures,26 but not the risk of nonvertebral or hip fractures.27 Increased occurrences of venous thromboembolic diseases and fatal stroke are the main side effects of raloxifene,28 which should be weighed against bone benefits in the clinic. Although considered the first-line drugs for OP, bisphosphonates are not recommended for patients with osteopenia who do not meet the diagnostic criteria of OP or have no history or high risk of fracture. Many patients are also reluctant to accept the treatment due to some unpleasant side effects, such as gastrointestinal (GI) discomfort, atypical femoral fractures and mandibular necrosis.29 30 Although not observed in clinical trials, upper GI intolerance (including GI intolerance, oesophageal irritation or oesophageal erosion) has been reported as a common adverse event (AE) of oral bisphosphonate in the clinical practice, if administered incorrectly.31 Approximately 50%–60% of administered bisphosphonate is excreted unchanged by the kidneys. The effect of bisphosphonates on renal function is also a concern. Bisphosphonates are associated with a 12% excess risk of chronic kidney disease progression in patients with stage 3B+ chronic kidney disease,32 and bisphosphonates are contraindicated in patients with stage 4+ chronic kidney disease. In addition, atypical femoral fractures and osteonecrosis of the jaw (ONJ) are rare bisphosphonate-related AEs in the clinic. The estimated prevalence of ONJ and atypical fractures are 0.0004%–0.10% and 0.05%–0.22%, respectively, which also affect the patients’ willingness to use bisphosphonates in the long term.29 Therefore, it is imperative to identify a safe and effective therapy that acts synergistically with CaD for cases of postmenopausal osteopenia to delay or reverse bone loss to prevent OP and osteoporotic fracture.
Moxibustion is a traditional Chinese therapy used to treat disease with smoke and heat produced by burning herbs, such as mugwort leaves.33 Previous studies have shown that moxibustion relieves back pain and improves the quality of life in patients with primary oOP,34 and when combined with acupuncture, moxibustion also reduces immune inflammation via decreasing TNF-α and immunoglobulin M (IgM) in spinal cord injury patients with secondary OP.35 Systematic reviews have found that moxibustion in combination with conventional therapy (anti-OP medicine) may be more effective in alleviating pain, enhancing BMD and increasing the level of osteoprotegerin and bone alkaline phosphatase compared with conventional therapy alone, but evidence has been limited and of relatively low quality.36 37 Moreover, there is a lack of clinical studies on the use of moxibustion to delay bone loss and prevent OP or osteoporotic fracture in patients with osteopenia, and the role of moxibustion in osteopenia is still uncertain.
Therefore, we devised a rigorous, parallel-design, randomised, patient-blind and assessor-blind, controlled clinical study to explore the therapeutic effectiveness of moxibustion on osteopenia. This study is expected to identify a safe and ideal therapy to delay postmenopausal bone loss and prevent OP.
Methods and analysis
Study design
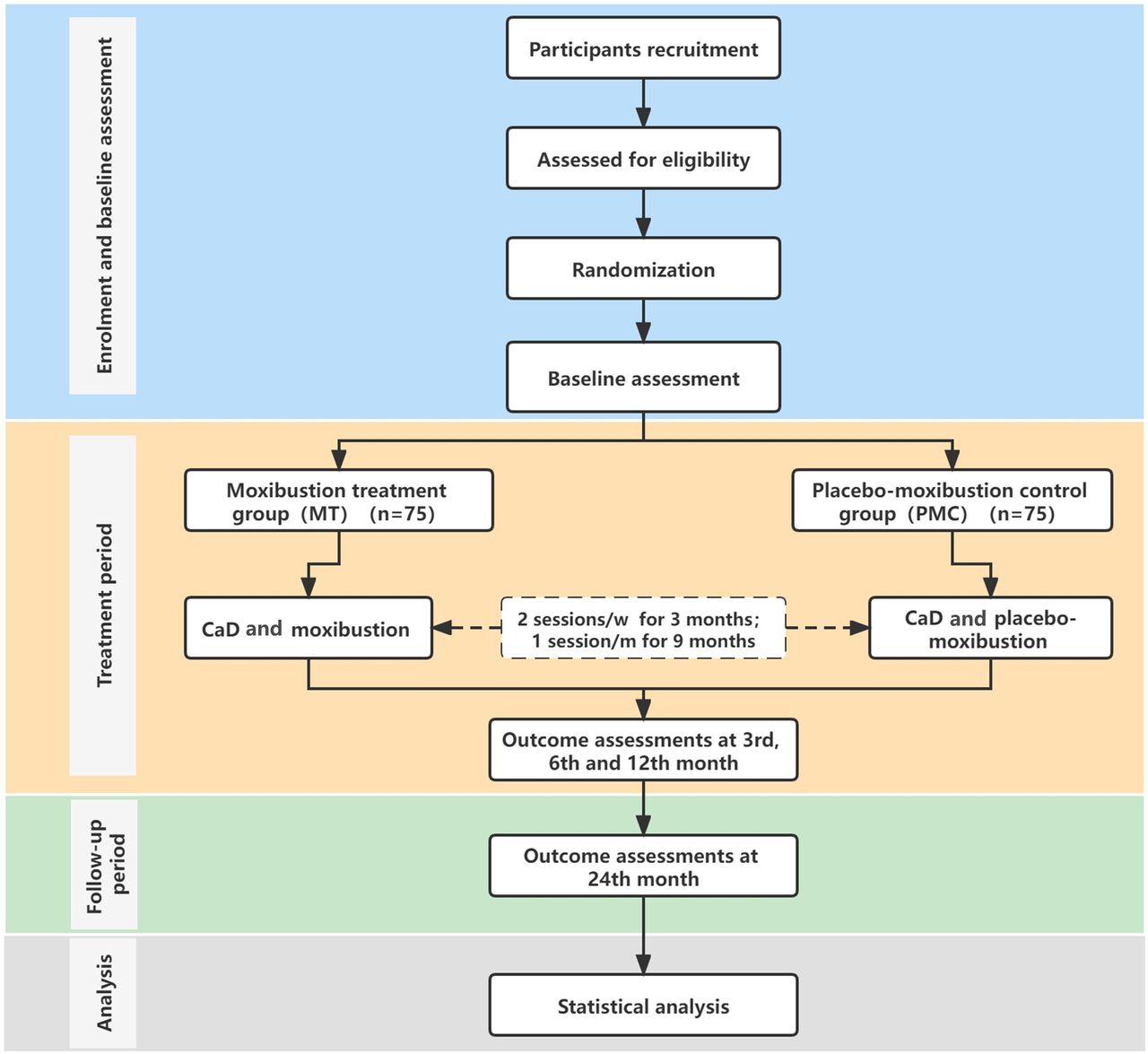
This study is a parallel-design, randomised, patient-blind and assessor-blind, controlled clinical study. One hundred and fifty eligible participants will be randomly assigned to a moxibustion treatment (MT) group or a placebo-moxibustion control (PMC) group in a 1:1 ratio. The total observation period is about 2 years, including a 2-week baseline period, a 12-month treatment period and a 12-month follow-up period. Participants will receive 42 sessions of moxibustion or placebo-MT over 12 months (two sessions per week in the first 3 months and two sessions per month in the following 9 months). During baseline, treatment and follow-up periods, participants will not be allowed to take any anti-OP drugs (eg, alendronate, zoledronic acid, salmon calcitonin or denosumab) in addition to CaD, which complies with the guidelines. However, necessary analgesics (eg, ibuprofen, paracetamol and ibuprofen) will be permitted when ostealgia is unbearable. The type, dose and time of administration will be recorded in the case report form (CRF). Assessments will be conducted at baseline and at 3, 6, 12 and 24 months after randomisation. The Consolidated Standards of Reporting Trials and the Standard Protocol Items: Recommendations for Intervention Trials have been used as frameworks of methodology for designing this protocol. A flow chart of the trial procedure is presented in figure 1. The planned study period is from 1 January 2022 to 31 December 2025.

Flow chart of the study procedure. CaD, calcium and vitamin D; MT, moxibustion treatment.
Recruitment
Patients with osteopenia will be recruited by reviewing and screening outpatients at the West China Hospital of Sichuan University as well as through media releases andcommunity advertisement including distribution of leaflets via regular community health counselling and media campaigns.
Participants
Sample size
We will recruit osteopenia subjects who meet the diagnostic criteria specified in the American Association of Clinical Endocrinologists/American College of Endocrinology (AACE/ACE) Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis-2016.19 According to a previous similar study, the mean and SD of BMD after treatment in the western medicine treatment group was 0.77 and 0.08, while the BMD in the western medicine combined with the MT group was 0.83 and 0.12.38 In this study, assuming a significance level of 0.05 and a study power of 0.9, 62 participants are required to reject the hypothesis that moxibustion is equivalent to the placebo moxibustion. Considering a 20% attrition bias, a total of 150 participants should be recruited, with 75 in each group.
Inclusion criteria
Eligible participants should conform to the diagnostic criteria of osteopenia in the AACE/ACE guidelines19 and those who meet the following inclusion criteria will be included:
Females aged 40–65.
Females within 5 years of menopause.
Patients with a T-score between –1.0 and –2.5 in the spine, femoral neck, total hip or 33% radius.
Patients whose 10-year probability of hip fracture <3% and any major osteoporotic fracture <20% predicted by the fracture risk assessment tool.
Patients who agree to participate in this study and provide written informed consent.
Exclusion criteria
Participants meeting any of the following criteria will be excluded:
Patients with osteoporotic fractures.
Patients who have used or are using anti-OP drugs (such as bisphosphonates, calcitonin).
Patients who have taken other drugs affecting bone metabolism (such as oestrogen, glucocorticoid) in the last 3 months.
Patients who have an abnormal anatomy of the lumbar spine or hip and whose BMD cannot be accurately measured by DXA detection.
Patients who have endocrine diseases related to secondary OP (such as diabetes, hyperthyroidism, hypothyroidism, thyroid cysts).
Patients suffering from rickets, rheumatoid arthritis and other diseases affecting the balance of bone metabolism.
Patients who have undergone a hysterectomy or ovariectomy.
Patients with serious heart, liver, kidney and mental diseases.
Patients with drug or alcohol dependence or abuse.
Patients participating in other clinical trials.
Drop-out criteria
The researcher may stop treatment and observation of a participant according to the prescribed criteria, and participants can drop out voluntarily at any time. Drop-out criteria are as follows.
Serious AEs occur, which should be assessed by OP specialists.
Symptoms become worse, or serious complications (eg, fracture) or other serious diseases occur, and emergency measures are needed during the study period.
Patients or a legal representative demand cessation of the trial because of unsatisfactory effects or withdrawal of consent.
Patients who fail to continue for at least 24 sessions of treatment and cannot finish the visits of the first year.
Randomisation and allocation concealment
Randomisation will be performed via a computerised random number generator operated by a statistician who has no clinical involvement in this trial. The random list will be concealed by sequentially numbered, opaque, sealed envelopes. Group information will be placed into the envelopes. On completion of baseline screening, the researcher will notify the statistician to open the envelope according to the participant’s screening sequence number, and then assign the participant into the MT group or the PMC group.
Blinding
This is a patient-blind and assessor-blind trial, as it is difficult for practitioners to be blinded in moxibustion manipulation. Therefore, practitioners are not allowed to take part in the assessment procedure. Participants in different groups will receive treatment in different therapeutic rooms and be blinded to their treatment allocations. Blind evaluation of participants will be conducted at the end of the observation period. The outcome assessors, data collectors and statisticians will be blinded to group allocations during the study.
Interventions
Conventional treatment protocol
All patients with osteopenia with low fracture risk will receive bone-protective drugs during the entire study period as recommended by the guidelines, including 600 mg of calcium supplements and 800 IU of vitamin D3 per day orally. The drug name, dosage and usage will be recorded in the CRF.
Moxibustion and placebo-MT protocol
Moxibustion will be added to the conventional treatment described above. Guanyuan (RN4), Mingmen (DU 4), bilateral Shenshu (BL 23) and bilateral Zusanli (ST 36) were selected as the standard acupoints in the moxibustion therapy (figure 2). The above acupoints will be divided into two groups as follows: one group will include RN 4 and ST 36, and the other will include BL 23 and DU 4. The two groups of acupoints will be stimulated in alternating sessions. For example, in one session of treatment, a patient will be asked to take a supine position, and her RN 4 and ST 36 will be stimulated; in the next session, the same patient will be asked to take a prone position and BL 23 and DU 4 will be stimulated.

Moxibustion on guanyuan (CV 4), mingmen (GV 4), bilateral Shenshu (BL 23) and bilateral zusanli (ST 36). The diagram is provided by 3D Body software.
We will apply the novel moxibustion device (Happyall, BX-A002, Chongqing Happyall Medical Equipment) for MT (figure 3). This device is composed of the following four parts: an adhesive plaster, a cylindrical pedestal, a cylindrical cap and a moxa stick with a magnet in the top. The base of the device is an adhesive membrane (figure 3A). The moxibustion device (figure 3B), as the container for the moxa sticks, will be used for patients in the MT group, while a handmade placebo moxibustion container will be used for the participants in the PMC group. The handmade placebo-moxibustion device has a similar appearance to the active moxibustion one, except that it has a thermal insulation board and tinfoil to prevent smoke and most of the heat from radiating to the skin (figure 3C). Both treatments will be performed by licensed acupuncturists with more than 3 years’ experience. Participants in all groups will receive 42 sessions of MT over 12 months (twice a week in the first 3 months and twice a month in the following 9 months), and each session will last 30 min.

{kind=link}
{kind=link}
{kind=link}
Diagram of the moxibustion and placebomoxibustion devices. (A) The moxibustion device is comprised of the following components: (1) an adhesive plaster; (2) a pedestal; (3) a cap with a magnet for fastening the moxa stick; (4) a moxa stick with a magnet at the top and (5) the whole device (B) Operation of the moxibustion container requires the following methods: (1) fix the moxa stick on the cap of the device; (2) ignite the moxa stick; (3) cover the cap on the pedestal; and (4) adhere the device on the acupoint. (C) The placebomoxibustion device is the same as the active one, except for a thermal insulation board placed on the bottom of the pedestal to block smoke and heat. The placebomoxibustion device is composed of the following components (1) a thermal insulation board; (2) a pedestal; (3) the placebo device and (4) the active device.
Outcome measures
Primary outcome measure
The primary outcome measure will be BMD of the lumbar spine (L1–4) at the end of the 12-month treatment. The BMD will be measured using dual-energy X-ray absorptiometry (DXA) (iDXA, GE Lunar, USA) before and after treatment.
Secondary outcome measures
The following secondary outcomes will be included: (1) BMD of the lumbar spine at the end of the 12-month follow-up period; (2) BMD of the femoral neck and total hip at the end of the 12-month treatment period and 12-month follow-up; (3) T-score of the lumbar spine, femoral neck and total hip at the end of the 12-month treatment period and a 12-month follow-up; (4) bone turnover markers (β-CTX, P1NP and bone-specific alkaline phosphatase); (5) serum calcium, magnesium, phosphorus, parathyroid hormone (PTH) and 25-hydroxyvitamin D levels; (6) Visual Analogue Scale of bone pain; (7) assessment of health-related quality of life via the 16-item Assessment of Health-Related Quality of Life in Osteoporosis and the 12-item Short Form Health Survey; (8) incidence of OP or fractures captured via imaging examinations (X-rays or CT, eg, vertebral, non-vertebral and hip); (9) usage of emergency drugs or surgery related to bone loss; (10) participants’ self-evaluation of therapeutic effects (‘no help’, ‘little help’, ‘average help’, or ‘great help’) and (11) the rate of AEs (described as unfavourable or unintended signs, symptoms or diseases occurring after treatment) related to moxibustion or conventional drugs, which will be observed and reported by participants and practitioners during the entire research period. In addition, all AEs will be recorded in detail in the CRF by the corresponding research staff.
The BMD and T-scores from DXA will be measured at months 0, 12 and 24. Blood tests and assessments of bone pain and quality of life will be performed at months 0, 3, 6, 12 and 24. The remaining outcomes as specified above will be summarised at months 12 and 24. The outcome measurement time points are provided in detail in table 1.
Details of the planned visit schedule
Additional outcome measures
The additional indicators will be included: (1) evaluation content of moxibustion expectation value and its effect correlation with main outcome indexes at baseline and (2) evaluation of blinding after the last treatment.
Data collection
Data collection will be performed at baseline and at 3, 6, 12 and 24 months after intervention. All data will be input by special data collectors after clinical evaluation by outcome assessors. AEs of moxibustion or drugs will first be recorded in the CRFs by the physicians in charge. Data will be double-entered into electronic CRFs. Personal information and study data of all participants will be recorded in CRFs. Moreover, data involving patient privacy will be anonymised, protected by code and securely kept in a locked cabinet accessed only by the research team. In principle, clinical data will not be released without the permission of the principal investigator, with the exception of emergencies or as required for monitoring and auditing by the data monitoring centre. Data for use or analysis following study completion will be available from the corresponding author on reasonable request. The study results will be presented at national and international scientific conferences, as well as submitted for publication in a peer-reviewed journal.
Statistical analysis
Primary analysis will be based on an intention-to-treat population, including participants with at least one assessment of the primary outcome and one moxibustion session. Per-protocol (PP) analysis will be performed to test the robustness of the primary analysis. The PP population will include participants receiving at least 24 sessions of moxibustion and they be assessed at month 12. Missing values will be imputed using the multiple imputation method (n=5).
Continuous variables with normal distribution will be expressed as the mean with SD; skewed variables will be expressed as median (95% CI); and categorical variables will be described as frequency (percentage). Student’s t-test for normally distributed variables, the Mann-Whitney U test for skewed variables and the χ2 test will be used to compare baseline data differences. Categorical variables will be analysed via χ2 tests for between-group comparisons. Between-group differences in BMD, T-scores, bone turnover markers, serum electrolytes, PTH and 25-hydroxyvitamin D levels will be tested using generalised linear models. Considering that efficacy might be affected by factors such as age, degree of disease and course of disease, all factors will be considered as covariates for covariance analysis.
All statistical analyses will be performed using Stata or R programs with a two-sided p<0.05 considered significant.
Patient and public involvement
Patients and/or the public were not involved in study design or conduct of the study. The present trial was developed by acupuncturists based on previous clinical experience and literature. The expected outcomes are commonly used to assess postmenopausal bone loss in clinical practice. The cost of interventions and outcome measurements will be maintained using the study funding; therefore, it was not considered a significant burden and met the patient preferences. The results will be disseminated to the participants via the WCHSU website.
Ethics and dissemination
Ethical approval
The study will be conducted in accordance with the Declaration of Helsinki. Ethics approval has been obtained from the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University (permission number: 2021-1243). Trained research assistants will provide participants with both verbal and written information describing the potential risks and benefits of the clinical study. Written informed consent will be obtained from all participants before enrolment. Any modifications to the protocol will be reported and approved by the ethics committee and will be communicated to the trial registry, investigators and data monitoring researchers.
Dissemination
The study results will be disseminated via conference presentations and papers published in academic peer-reviewed journals. The participants, healthcare professionals, the public and other relevant groups will also be informed of the study results.
Discussion
Postmenopausal osteopenia is the transition period from healthy bone to OP, and it may be the key period for remodelling bone homeostasis to delay or reverse bone loss. During this period, the guidelines do not recommend premature use of antiosteopathic drugs, which are recommended for PMOP or for people at high risk of fracture.19 Therefore, we intend to use postmenopausal women with osteopenia to identify a safe and effective PMOP prevention method.
Acupuncture and moxibustion therapy have demonstrated to be potential treatments for a variety of sex hormone-related diseases, such as premature ovarian failure and perimenopausal syndrome,39–42 as they can improve levels of oestrogen (estradiol, progesterone and prolactin)40 Moxibustion has been shown to regulate circulating levels of estradiol and follicle-stimulating hormone in the ovaries of perimenopausal rats as well as to inhibit ovarian granulosa cell apoptosis through the Forkhead box Protein O1 and JAK2/STAT3 pathway, similar to exogenous oestrogen supplementation.41 Moxibustion also improves the antioxidant stress-related genes HO-1 and NQO-1 and their protein levels, and enhances antioxidant capacity.43 44 In addition, moxibustion has anti-inflammatory potential, resulting in local or systematical reduction of IL-2, IL-6 and TNF-α levels,45 46 for the treatment of ulcerative colitis, lumbar disc herniation, periarthritis of shoulder and fatigue.45–48 Animal studies have shown that moxibustion increases BMD and bone strength in ovariectomised rats, and the mechanism may be related to the improvement of serum E(2) concentration, the decrease of serum alkaline phosphatase level concentration and the upregulation of Erα mRNA expression in MSCs.49 50 Therefore, we speculate that moxibustion is a potential treatment for delaying postmenopausal bone loss via increasing oestrogen level to resist oxidative stress and suppress inflammation. Clinical studies have reported that the combined therapy of moxibustion and oral calcium supplements improves BMD, relieve pains and decreases the urinary calcium to creatinine ratio in patients with primary OP.51 52 Previous systematic reviews have shown that moxibustion effectively may relieve the pain caused by OP and increase femoral neck BMD, however, evidence of clinical efficacy and safety remains inadequate due to the lack of high-quality studies.36 37 Therefore, it is important to design rigorous clinical studies to verify the clinical effect of moxibustion on preventing postmenopausal bone loss.
A fixed acupoint prescription will be applied in this study, to include Guanyuan (RN4), Mingmen (DU 4), bilateral Shenshu (BL 23) and bilateral Zusanli (ST 36), which are the most commonly used acupuncture points in the clinical treatment of OP mentioned in aprevious systematic review.36 The treatment course for moxibustion ranges from 3 to 12 months with a frequency of 1–5 sessions per week according to previous studies.36 37 Considering the characteristics of bone metabolism and patient compliance, we formulated a 12-month treatment plan containing a 3-month strengthening phase and a 9-month maintenance phase. Patients will be treated twice weekly during the strengthening phase, and once monthly during the maintenance phase.
Placebos play an important role in the evaluation of clinical efficacy, which can help separate specific and nonspecific effects as well as reduce bias by enabling blinding. However, it is extremely difficult to find or invent an inert method, indistinguishable from the true intervention, for physical therapy such as moxibustion. For this study, we modified an ordinary moxibustion box with a thermal insulation board and tinfoil over the iron wire gauze to block smoke, heat and radiation to be used as a placebo control. In addition, patients in the two groups will be set up in different rooms to receive treatments, in an effort to block communication between the two groups and reduce patients’ uncertainties regarding the different interventions. Moxibustion will be performed on fixed acupoints by two acupuncturists who have passed professional and training exams to reduce the influence of participants' psychological factors on clinical effects (especially on subjective efficacy evaluation indicators such as pain). At the end of the treatment, participants will be evaluated to confirm whether the blindness is successful. Through use of the methods described above, the clinical effect of moxibustion as an adjuvant method for delaying postmenopausal bone loss will be relatively accurately evaluated.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank to 3D Body software (ShangHai QiaoMedia Information Technology) for providing the diagram of the moxibustion treatment acupoints.
References
Footnotes
Contributors LL, XZ, QW, XY and NL participated in the conception and design of this trial, and in plans for the data. LL and XZ were responsible for planning the draft and revising the manuscript. XY and NL are monitors of this study. JL and XZ are responsible for the recruitment and/or treatment of patients. QW and LL are responsible for collecting the data. All authors have read the manuscript and approved the publication of this protocol.
Funding This work was supported by the National Natural Science Foundation of China (no. 81770875) and the Post-Doctor Research Project, West China Hospital, Sichuan University (no. 19HXBH053).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.