Article Text

Abstract
Objectives To examine the physical, psychological and pandemic fatigue during the COVID-19 pandemic, and to explore the correlates of fatigue using a representative, population-based, community sample of Chinese adults in Hong Kong.
Design Cross-sectional study.
Setting Telephone surveys in Hong Kong from December 2020 to January 2021 (during the fourth wave of COVID-19 outbreak).
Participants 1255 adults living in Hong Kong aged 18 years or older sampled using a multistage approach (53% women).
Main outcome measures Physical and psychological fatigue: The Fatigue Assessment Scale (with a cut-off score of 22). Pandemic fatigue: Adherence to six disease prevention measures (DPM) recommended by the government.
Results About 25.7% of the participants were feeling fatigued physically and psychologically. Physical and psychological fatigue was not directly associated with pandemic fatigue, and their association was fully mediated by self-perceived disruptions of COVID-19-related restrictions in daily life. Results from the hierarchical regression analysis showed that higher levels of fatigue were associated with economically inactive status (B=0.18, SE=0.04, p<0.001), having family or friend infected with COVID-19 before or during the study (B=0.17, SE=0.01, p<0.001), lower acceptability of DPM (B=−0.16, SE=0.03, p<0.001), greater disruptions in daily life (B=0.22, SE=0.02, p<0.001), and greater trust in authorities in ending the pandemic (B=0.11, SE=0.02, p<0.001).
Conclusions Fatigue affected many individuals during the pandemic. Disruptions of DPM in daily life may serve as a mediator in the association between pandemic fatigue and physical and psychological fatigue, reflecting the need of effective interventions to reduce self-perceived disruptions of COVID-19-related restrictions in the general population. Resources should be allocated to provide sufficient services to individuals vulnerable to fatigue during the prolonged pandemic.
- COVID-19
- Public health
- MENTAL HEALTH
Data availability statement
Data are available upon reasonable request. Relevant anonymised manuscript level data are available on reasonable request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to assess the levels of fatigue among the general Chinese population during an epidemic wave of the COVID-19 pandemic in Hong Kong.
One of the major strengths is the use of a comprehensive approach to examine different aspects of fatigue, including physical, psychological and pandemic fatigue, in a population-based, community sample.
The investigations on the correlates of fatigue and the mediating effect of self-perceived disruptions in daily life provide insights on the design and implementation of future disease preventive measures and restrictions.
The measurement of pandemic fatigue was indirect because there was no validated, direct assessment scale available at the time of the study.
The cross-sectional nature of the study did not allow the investigation of causal relationships among variables.
Introduction
Since its outbreak in December 2019, the COVID-19 pandemic has become a serious global threat. As of September 2022, the number of confirmed cases has reached 601 million, including almost 6.5 million deaths worldwide.1 Data show that COVID-19 and its related issues are associated with various physical, psychological, social and economical consequences (eg, fear or distress due to the loss of beloved ones, fear of unemployment, financial crisis).2 Among various negative consequences, fatigue is one of the most commonly reported health issue overlooked by existing research.3 4 Fatigue is a condition occurring during exercise, a symptom of a disease, a pathological reaction or a psychological reaction to stress and other negative emotions.5 6 It can be classified into three main categories7: (1) subjective feeling of physical or psychological tiredness that can be related to a health condition, sustained activities, deprivation of sleep or physical or mental exertion; (2) reduced ability to perform a task due to insufficient physical or mental resources; and (3) negative feelings as a result of prolonged exposure to aversive circumstances. In the case of COVID-19, fatigue can be a mere symptom of the disease, an indicator of the underlying psychological problems (eg, stress and anxiety related to the pandemic) or both.8 In addition to the general distressing conditions resulting from the disease, the COVID-19 prevention measures adopted worldwide, such as lockdowns, curfews and social distancing regulations, may impose further negative influences on the physical and psychological well-being.9 Hampered well-being, together with anxiety, worries, social isolation and the lack of physical movement resulting from those prevention measures, may lead to a long-term state of physical and psychological fatigue during the pandemic. In addition to the physical and psychological fatigue, a fourth category, namely pandemic fatigue, has been observed across countries over the course of the pandemic. According to the WHO,10 pandemic fatigue refers to ‘distress as a reaction to sustained and unresolved adversity which may lead to complacency, alienation and hopelessness, emerging gradually over time (p.7)’, which can lead to a drop in motivation to follow recommended protective behaviours or to accept disease prevention measures and restrictions. Pandemic fatigue is regarded as a ‘natural’ reaction to the current crisis that has been dragged on for too long.11 12 Individuals are forced to adopt a different lifestyle; and the negative emotions related to the long-term personal, social and economical changes and the disruptions in life plan caused by various pandemic responses and restrictions are likely to accumulate over time. As a result, behavioural fatigue and demotivation may emerge.10
Hong Kong is among the first places in the world in which COVID-19 cases were detected. Since the first confirmed case reported on 23 January 2020, the city has been greatly affected by the COVID-19 and related disease prevention measures (DPM). As of September 2022, over 1.5 millions of citizens have contracted the disease (approximately 21% of the population), and almost 10 000s of them died.13 To follow the ‘zero-COVID’ policy implemented by the Chinese central government, the Hong Kong government has been imposing ‘some of the world’s strictest’ regulations and restrictions on social distancing, travel, quarantine and mask wearing.14 For example, during the fourth epidemic wave of COVID-19 from late 2020 to early 2021, face-to-face classes at schools were all suspended, and some districts were temporarily ‘lockdown’ for several days for compulsory quarantine. Flights from certain countries (eg, UK) were banned, and overseas residents who returned to the city must undergo 21 days of quarantine. From time to time, bars, clubs, cinemas and beauty salons were ordered to suspend operations while restaurants were not allowed to provide dine-in services. To date, some of the strict social distancing restrictions still remain effective in the city. Whether the long-term implementation of strict DPM may reduce public adherence is of concern. Literature has suggested that public adherence to DPM could greatly affect the effectiveness in controlling the spread of COVID-19,15 and pandemic fatigue and disruptions in daily life can be the most determining factors that lead to demotivation of accepting and following the recommended DPM.7 10 A recent population-based telephone survey in Hong Kong revealed a decline in the compliance with social distancing measures in the general population, reflecting a possible state of pandemic fatigue in the city.16
Despite the preliminary research efforts that demonstrated various degrees of fatigue during the pandemic, empirical studies on the general populations were scarce. In particular, physical and psychological fatigue experienced by the general populations has received little attention in the COVID-19 literature, and fatigue has rarely been examined as a psychological problem or as a correlate of issues related to COVID-19.3 For example, the 2021 study conducted in Hong Kong focuses on the trend of adherence to DPM, and does not include any analysis on the associated factors of the adherence/non-adherence.16 Understanding how pandemic fatigue and other aspects of fatigue are affected by different factors, and exploring effective strategies to reduce fatigue are the key to successful disease preventive measures during the prolonged pandemic. This study aimed to fill this research gap by investigating the physical, psychological and pandemic (behavioural) fatigue, and examining their associated factors using a population-based, random sample during one of the biggest epidemic waves in Hong Kong. Our primary research questions were: (1) how individuals were affected by physical and psychological fatigue; (2) whether pandemic fatigue, which could be reflected by the non-adherence to DPM, appeared in the general population; (3) how pandemic fatigue could be associated with physical and psychological fatigue; and (4) what factors affected the levels of fatigue among individuals in Hong Kong.
Methods
Study design, setting, and participants
This cross-sectional study was a population-based telephone survey conducted from December 2020 to January 2021 in Hong Kong. During that time, Hong Kong was experiencing one of the biggest epidemic waves, and relevant DPM and restrictions implemented by the government were strict. Participants were Chinese-speaking adult residents (aged 18 years or above) in Hong Kong during the study period. In this study, Hong Kong residents referred to individuals who possessed a Hong Kong Identity Card issued by the Immigration Department of Hong Kong, and covered both permanent residents and those working or studying in the city on a short-term basis. Due to the nature and language requirements of the telephone survey, individuals who could not communicate in Chinese (Cantonese or Mandarin) or those who did not possess a mobile or landline phone were excluded. According to the 2016 Population By-census in Hong Kong,17 there was a population of 6.48 million aged 18 or above, of which 96.7% were able to communicate in Chinese. With regard to this, our target sample size was 1250, giving a maximum sampling error of 3% at the 95% confidence.
We employed a multiphase procedure to sample and recruit participants. First, telephone numbers were drawn randomly from a list of landline and mobile directories provided by the government. These randomly drawn numbers were then used as ‘seeds’ to generate another set of telephone numbers with the ‘±one/two’ method. The second set of telephone numbers was then compared with the first to remove any duplicated number. Using the final set of numbers, trained interviewers contacted all eligible participants and invited them to join the survey via telephone calls under close supervision by our research team. Interviewers made telephone calls from 09:00 to 21:00, from Monday to Sunday. Each number on the final set was called at least five times on different days before being classified as ‘non-contact’.
All participants provided oral consent before the structured telephone interview began. Data were collected anonymously with a computer-assisted telephone interview system which allowed real-time data capture and consolidation. The survey comprised about 50 items, and took approximately 30 min to complete. To ensure data quality, 15% of the successful interviews were counter-checked by our research team. All data were handled anonymously in aggregate. Participants were allowed to omit any question or withdraw from this study at any point of the interview.
The final set of this study comprised of 2784 telephone numbers. A total of 1255 participants completed the telephone interviews (response rate=45%). Among those unsuccessful cases, the majority was non-contact (35%), followed by refusal to participate (19%) and language barriers (1%).
Patient and public involvement
Patients and the public were not involved in the research design, conduct, reporting or dissemination plans.
Main outcome and other variables
Fatigue was assessed with the 10-item Fatigue Assessment Scale (FAS),18 a self-reported tool which measured physical and psychological fatigue in the general population. Participants were asked to rate their level of fatigue on a 5-point Likert scale, from 1 (never) to 5 (always), on each of the items (eg, ‘I get tired very quickly’ and ‘I feel no desire to do anything’). The total score ranged from 10 to 50, with a higher score indicating a higher level of fatigue. The FAS achieved a good internal consistency in this study, with a Cronbach’s alpha of 0.87. It had been used in a previous study on fatigue during COVID-19 pandemic,8 and a cut-off score of 22 was used to indicate individuals with fatigue. We adopted this cut-off score and classified participants as feeling fatigued when their FAS total score was 22 or above.
Pandemic fatigue was operationalised as a low level of adherence to DPM. Levels of adherence to six DPM recommended by the Hong Kong government, including wearing of masks in public areas; proper hand washing after using the toilet; use of hand sanitiser before eating food; social distancing and avoidance of group gathering; avoidance of touching eyes, nose and mouth before washing hands; and participation in voluntary COVID-19 testing when in need, were assessed. Participants reported their level of adherence to each DPM on a 5-point Likert scale, from 1 (‘never/almost never’) to 5 (‘always’). Item scores were averaged to create an overall adherence level, with a higher score indicating a greater adherence to DPM. The adherence scale had a satisfactory reliability in this study (Cronbach’s alpha=0.68).
Apart from the actual adherence to DPM, we also assessed participants’ acceptability of those measures recommended in Hong Kong. Six items were used (eg, ‘Mask mandate is acceptable and reasonable’ and ‘Prohibition on group gathering is acceptable and reasonable’), and participants were asked to rate each item on a 5-point scale, from 1 (‘strongly disagree’) to 5 (‘strongly agree’). Item scores were averaged, and higher scores reflected higher levels of acceptability of DPM. Cronbach’s alpha of the scale was 0.85.
Disruptions in daily life related to COVID-19 were measured with a list of nine items. Participants rated, on a 5-point scale from 1 (‘never’) to 5 (‘always’), the degree of disruptions in different aspects of their living routines caused by or related to the COVID-19 pandemic. Sample items included (‘My social life has been affected by the COVID-19 pandemic’) and (‘My use of medical and social services has been affected by the COVID-19 pandemic’). Average item scores were obtained to indicate the level of disruption: the higher the score, the greater the level. The internal consistency of the disruption scale was good, with a Cronbach’s alpha of 0.88.
Trust in authorities was assessed with two items: (‘I trust the government in handling the COVID-19 pandemic’) and (‘I trust the medical and healthcare professionals in controlling the spread of COVID-19’). Items were rated on a 5-point scale, from 1 (‘strongly disagree’) to 5 (‘strongly agree’). A higher average score reflected a greater level of trust in authorities in general.
In addition to the above variables, demographic characteristics, which included participants’ gender, age, highest education attainment and economic activity status, were captured in the telephone survey. Participants were also asked to report whether any of their family members or friends had ever been infected by COVID-19. Data were recorded as 1 (‘None have been infected by COVID-19.’) or 2 (‘At least one of them have been infected before.’).
Data analysis
To ensure the representativeness of the final sample, the raw data collected were rim-weighted according to the latest sex-age distribution of the Hong Kong adult population. We summarised the descriptive statistics of the demographic variables, and computed the mean scores and SD of the main outcomes and other variables. To explore the correlates of physical and psychological fatigue among the general public during the pandemic, we performed a hierarchical multiple regression analysis with four blocks of independent variables. The first block covered demographic variables (ie, gender, age, highest education attainment and economic activity status) and the infection status of one’s family and friends; the second included adherence to DPM and acceptability of DPM; the third was disruptions in daily life; and the fourth was trust in authorities. To reduce possible confounding effects, all parameter estimates were adjusted for the variables in the previous block(s). Multicollinearity was checked to ensure that independent variables in the regression model were not intercorrelated.
All analyses in this study were conducted with SPSS V.26.0, and two-sided p values smaller than 0.05 were considered statistically significant. Missing data were handled with listwise deletion to ensure the completeness of the data set.
Results
Participants’ characteristics
In this study, 47.0% of the participants in this study were men (table 1). The majority was senior residents who were 55 years old or older (41.3%), followed by those between 35 and 54 years of age (35.0%) and those between 18 and 34 years (23.7%). Over two-thirds (68.6%) of the participants had at least completed secondary education. Most were economically active during the study period (65.7%), while about 4.9% were students, 11.3% were home-makers and 17.9% were retired.
Demographic characteristics of study participants
Fatigue and its correlates
The mean score of fatigue was 26.45 (SD=7.35). Using the cut-off score of 22, we found that about one in four participants (25.7%) were feeling fatigued. In this sample, women reported significantly greater fatigue than men (women: 26.95, men: 26.02, t=2.34, p<0.05), while there was no significant gender difference in the proportions of feeling fatigue using the cut-off score of 22 (men: 25.4%, women: 26.95, χ2=0.07, p=0.79).
Mean score of adherence to DPM was 4.12 out of a 5-point scale (SD=0.60), reflecting that participants usually or always adhere to the six DPM recommended by the government. Similarly, participants reported a high level of acceptability of DPM (mean=4.40, SD=0.66) as they agreed or strongly agreed that the six DPM were acceptable and reasonable. The mean scores of disruptions in daily life related to COVID-19 and trust in authorities were 3.37 (SD=0.89) and 3.72 (SD=0.78), respectively, indicating a moderate-to-high level of perceived disruptions and trust in authorities.
Results of the hierarchical regression analysis (table 2) showed that adherence to DPM and acceptability of DPM, together with the four demographic characteristics and the infection status of family and friends, predicted approximately 21.8% of the variance of fatigue (F7, 1247 = 50.93, p<0.001). After adjustment of demographic characteristics and the infection status of family and friends, adherence to DPM was positively associated with fatigue (B=0.11, SE=0.04, p<0.01), while acceptability of DPM was negatively associated with fatigue (B=−0.18, SE=0.03, p<0.001). In other words, higher levels of fatigue could be predicted by a higher level of adherence to DPM and/or a lower acceptability of DPM.
Hierarchical multiple regression model predicting fatigue among study participants (N=1255)
Adding disruption in daily life related to COVID-19 in the regression model gave a total predictive power of 28.4% (F8, 1246 = 63.23, p<0.001). Disruption in daily life was a positive predictor of fatigue (B=0.23, SE=0.02, p<0.001), reflecting that participants would report higher levels of fatigue with more disruption experienced. In this model, acceptability of DPM remained as a negative correlate of fatigue (B=−0.13, SE=0.03, p<0.001); however, the association between adherence to DPM and fatigue became non-significant (B=0.03, SE=0.04, p=0.60).
The final model, with the addition of trust in authorities, accounted for 29.8% of the variance of fatigue in this study (F9, 1245 = 60.08, p<0.001). In this model, higher levels of fatigue could be predicted by an economically inactive status (B=0.18, SE=0.04, p<0.001), an experience of family or friends being infected with COVID-19 (B=0.17, SE=0.01, p<0.001), a lower acceptability of DPM (B=−0.16, SE=0.03, p<0.001), greater disruptions in daily life related to COVID-19 (B=0.22, SE=0.02, p<0.001) and/or a greater trust in authorities (B=0.11, SE=0.02, p<0.001).
Mediating effect of disruptions in daily life
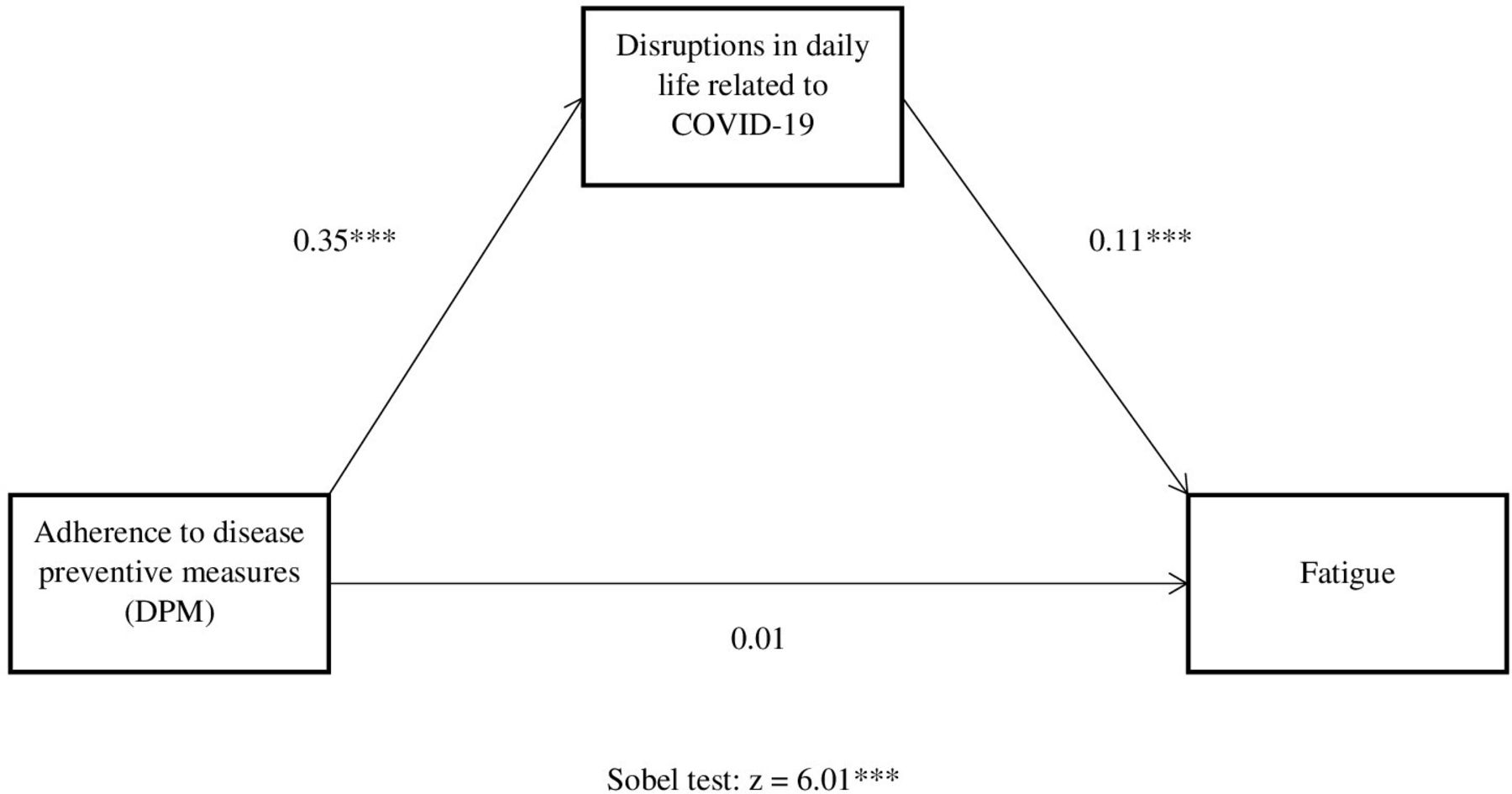
To further investigate the possible mediating effect of disruptions in daily life on the association between adherence to DPM and fatigue as observed in the regression models, we conducted a Sobel test. Results showed that, after controlling for other variables, the association could be fully mediated by disruptions in daily life (z=6.01, p<0.001, figure 1).
{kind=link}
Mediating effect of disruptions in daily life on the association between adherence to disease preventive measures and fatigue. *p<0.05, **p<0.01, ***p<0.001.
Discussion
Using a population-based sample recruited during one of the biggest epidemic waves of COVID-19 in Hong Kong, this study revealed that more than one-fourth (25.7%) of the general population were feeling fatigued physically and psychologically. Despite the long-term implementation of different DPM, such as mandatory mask-wearing and social distancing restrictions, the general population in Hong Kong reported high adherence and acceptance levels to them. This might reflect a low level of pandemic fatigue, a behavioural fatigue that would possibly lead to demotivation of complying with DPM, about 1 year after the first outbreak of the COVID-19. Our findings demonstrate the mediating role of self-perceived disruptions of DPM in daily life on the association between pandemic fatigue and physical and psychological fatigue. Besides, fatigue was associated with economically inactive status, experience of family or friends being infected with COVID-19, low acceptability of DPM and high levels of trust in authorities in ending the pandemic.
Comparison with other studies
Compared with the rates of fatigue during the pandemic in other countries,3 8 our findings revealed a relatively low proportion of individuals feeling fatigued. For example, in a US online survey on 260 Facebook adult users between August and September 2020, fatigue was found in as many as 75% of the respondents3; while in another Turkish study on 3672 adults between March and June 2020, the rate of fatigue was 64%.8 Only 25.7% of our participants were identified as ‘fatigued’ when the same cut-off score as the Turkish study was applied. The discrepancy in the rate of fatigue might be due to the differences in research design, methodologies or the time (which may correspond to different epidemic waves in the study location) during which the data were collected. Higher levels of fatigue found in other research might be resulted from tougher restrictions in different epidemic waves or different countries. Unfortunately, empirical evidence for the change in fatigue over time is lacking. Whether the discrepancy can be attributed to the divergence in the research time period and methodologies or the true difference in populations is inconclusive. Longitudinal research is clearly needed to explore whether rate of fatigue changes with the COVID-19 restrictions in the future.
Although the rate of fatigue was relatively low when compared with other existing studies, it was still higher than those found in previous research in Hong Kong before the emergence of the COVID-19 pandemic. As one of the very few studies that investigate chronic fatigue among the general public, a survey on 5001 adults in 2012 found that approximately 11% of the individuals experienced chronic fatigue in the past 6 months.19 In a more recent pre-COVID-19 study conducted in early 2019,20 researchers investigated fatigue among 112 patients who had a stroke using the FAS, the assessment scale that was used in this study, and reported mean scores of fatigue as 22.14–22.85 (SD=5.29–7.15), which were lower than the mean score we observed (ie, 26.46 (SD=7.35)). This might provide some preliminary evidence that both the proportion of individuals feeling fatigued and the level of fatigue increased during the pandemic.
In congruence with the data in other COVID-19 studies,7 21 our findings did not provide supportive evidence for the presence of pandemic fatigue in Hong Kong in the midst of the pandemic. Unlike other populations studied in some previous research,22 23 most individuals in Hong Kong were still complying with the prolonged DPM, including social distancing and mandatory mask wearing, during the time when relevant restrictions and rules have been implemented for approximately a year. However, limited by the cross-sectional nature of this study, comparisons of adherence levels across time were not allowed. In a longitudinal study using multiple surveys in Hong Kong,16 a declined adherence was observed, from mid 2020 to late 2020, in some of the social distancing behaviours examined. The authors suggested that pandemic fatigue might have possibly appeared in the general population, leading to a drop in motivation to comply with COVID-19 prevention measures.
In this study, physical and psychological fatigue was not associated with pandemic fatigue when disruptions in daily life were taken into consideration. Findings showed that self-perceived disruptions fully mediated the relationship between the two aspects of fatigue. Literature suggests that prolonged DPM and other restrictions related to COVID-19 could adversely affect individuals’ ways of life and coping, which might in turn lead to serious negative impacts on one’s physical and mental well-being.24 25 However, there is a lack of research that empirically examines the mechanism underlying the negative health consequences of DPM and restrictions, and how those they contributed to the influences on well-being are unknown. Our findings might provide some valuable insights on this issue, that long-term adherence to DPM and restrictions might be linked to exhaustion or fatigue through the overwhelming disruptions in one’s daily routines and activities.26
Our findings replicated some previous data and suggested that acceptability of DPM was a strong correlate of fatigue.8 27 A study in Argentina revealed that mental fatigue and other mental health issues were significantly related to intolerance or subjective issues to lockdown restrictions but not to adherence to the lockdown.27 In that case, mental fatigue might manifest at the emotional or psychological level, rather than the behavioural level. Similarly, our study showed that individuals feeling fatigued were more likely to show lower acceptability of DPM; while the low acceptability of DPM might not necessarily be escalated to a non-adherence or pandemic fatigue. A plausible explanation can be that the main drivers of pandemic fatigue were psychological, social or cultural factors amid its negative psychological consequences. For example, perceived risks of the COVID-19, fear of contracting the disease and awareness of one’s responsibility to prevent the spread of the virus are possible drivers which may counteract the influence of fatigue and help maintain high adherence to strict DPM and restrictions.23
Implications of the findings
The prolonged nature and the intensity of the COVID-19 and related restrictions could lead to a downstream torrent of negative health outcomes. These negative outcomes could be greatly reinforced by the unique adverse circumstances during the pandemic, such as threats of unemployment and fear of losing beloved ones, and cause serious physical and psychological disturbances to individuals.2 Yet, there was no conclusive evidence in this study that pandemic fatigue appeared in the city almost 1 year after the implementation of DPM and other restrictions. Despite the high levels of physical and psychological fatigue, most individuals still strongly adhered to DPM. However, before effective pharmaceutical solutions are available, our long-term fight against the COVID-19 and its variants continues. Pandemic fatigue can emerge any time in the future. To prevent this from happening, future research may focus on the identification of main drivers to increase one’s motivation to comply with DPM and other restrictions.
Our findings highlighted the relevance of developing interventions for specific group of individuals in order to reduce future fatigue during the prolonged pandemic. The increase in proportion of individuals feeling fatigued has highlighted an urgent need for public health strategies to ensure a sufficient coverage of the unprecedented physical and psychological health necessities caused by the pandemic. More resources should be allocated to increase the detection of individuals in need and the provision of health services and treatments to vulnerable groups. Findings of our study call for a need to support individuals who are economically inactive, who have family or friends being infected with the disease, who show low acceptability of DPM and who experience greater disruptions of the COVID-19 in daily life. Our data also showed that trust in authorities in ending the pandemic could be a correlate of fatigue. The government and stakeholders should strive to promote public trust, and to maintain a balance when implementing various restrictions in order to minimise disruptions in daily life of the general population.
Strengths and limitations of this study
One of the major strengths of this study is the comprehensive investigation of multiple aspects of fatigue in the general population during the COVID-19 pandemic. Previous research either focused on one aspect of fatigue only and failed to examine the associations between physical and psychological fatigue and pandemic fatigue,23 28 29 or used clinical or specific groups of participants (eg, stroke patients or healthcare professionals).20 30 To the best of our knowledge, this study is one of the first in its kind in the COVID-19 literature. Findings do extend current knowledge on the negative health outcomes caused by this global public health challenge. Besides, the use of a population-based, community sample maximised the generalisability of current findings, while the use of validated assessment tools for the primary outcome (ie, fatigue) would facilitate data comparison in future studies.
Like other studies, this study was prone to some specific methodological limitations. First, it was a cross-sectional survey and did not allow comparisons of variables over time. Inferences about temporal precedence of the associations among variables is limited. Second, the assessment of pandemic fatigue in this study was indirect. Since there had yet been any validated measures for pandemic fatigue available during the study period, the variable could only be operationalised as the non-adherence to DPM. Validity of the variable might be an issue that limited the interpretation of our findings. The third limitation involves the use of telephone surveys and the exclusion of non-Chinese-speaking populations (approximately 0.8% of the approached participants). These procedures inevitably excluded individuals who did not own a phone number or who could not communicate in Cantonese or Mandarin. Yet, telephone survey was one of the safest and most pragmatic approaches to reach out to our target participants during the biggest epidemic wave back then in December 2020. The response rate was 45% in this study, which is highly comparable with other modes of data collection procedures.31 The last limitation concerns the use of self-reports. Responses could have been affected by recall bias or social desirability. It could be expected that social desirability might be particularly influential to individuals’ responses during the study period, as adherence to mask wearing and some social gathering restrictions was enforceable under law. The assurance of anonymity at the beginning of the surveys should have mitigated this problem.
Conclusions
The COVID-19 pandemic has unparalleled impacts on individuals worldwide. It has been regarded as a global stressor that is induced by threats to health and well-being, economic crisis and disruptions in daily routines. Mandatory DPM and other restrictions may on one hand help slow down the spread of the disease, yet on the other hand they may lead to considerable physical and psychological disturbances in life. Findings shed lights on the needs for interventions and healthcare services targeting vulnerable groups. More resources should be allocated to provide services to individuals who have trust in authorities but experiencing great disruptions in daily life and low acceptability of DPM in order to minimise their physical and psychological fatigue in the long-term fight of the pandemic.
Data availability statement
Data are available upon reasonable request. Relevant anonymised manuscript level data are available on reasonable request from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by The Hong Kong Polytechnic University Human Subject Ethics Committee (Reference No: HSEARS20200814002). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors EY, DWLL and VWPL designed the study and acquired funding for the project. EY analysed and interpreted the data. EY and HKLN drafted the original paper. EY and HKLN revised the paper. All authors gave final approval of the current version of the paper. EY is responsible for the overall content as the guarantor.
Funding This work was supported by the Health and Medical Research Fund (HMRF) by the Government of Hong Kong Special Administrative Region (COVID190216).
Disclaimer The funding body has no role in research design, data collection, data analysis and interpretation, or preparation of the manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.