Article Text

Abstract
Objectives To summarise evidence on intrawork breaks and their associated effect on doctors’ well-being and/or performance at work.
Design Systematic review following Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 statement guidelines
Data sources Embase, PubMed, Web of Science (Core Collection) and PsychINFO were systematically searched on 6 June 2021.
Eligibility criteria No restrictions were placed on language, study design or date of publication.
Data extraction and analysis Methodological quality was appraised using Cochrane’s Risk of Bias (ROB-2), Cochrane’s Risk of Bias in Non-randomised Studies (ROBINS-I), and the Johanna Briggs Institute (JBI) checklists for cross-sectional, cohort and qualitative studies. Quantitative synthesis was not undertaken due to substantial heterogeneity of design and outcomes. Results are presented narratively.
Results Database searches returned 10 557 results and searches of other sources returned two additional records. Thirty-two papers were included in the systematic review, comprised of 29 unique studies, participants and topics and 3 follow-up studies. A variety of well-being and performance outcome measures were used. Overall, findings indicate that intrawork breaks improved some measures of well-being and/or work performance. However, methodological quality was judged to be low with a high risk of bias in most included studies.
Discussion Using existing evidence, it is not possible to conclude with confidence whether intrawork breaks improve well-being and/or work performance in doctors. There is much inconsistency regarding how breaks are defined, measured and the outcomes used to assess effectiveness. Future research should seek to: (a) define and standardise the measurement of breaks, (b) use valid, reliable outcome measures to evaluate their impact on well-being and performance and (c) minimise the risk of bias in studies where possible.
PROSPERO registration number CRD42020156924; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=156924.
- MENTAL HEALTH
- Human resource management
- OCCUPATIONAL & INDUSTRIAL MEDICINE
Data availability statement
Data supporting this study will be openly available from the University of Southampton public, open access repository following thesis submission in July 2023, as the work forms part of a PhD. Supplemental material. This content has been supplied by the authors. It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
No limits were placed on design, location, language or date of publication to ensure a comprehensive review of the subject area.
Review complies with Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 statement and was prospectively registered on the International Prospective Register of Systematic Reviews (PROSPERO) before commencement.
As meta-analysis was not possible, data are qualitatively synthesised.
Introduction
The overwhelming strain placed on health professionals across the globe in responding to the COVID-19 pandemic is well recognised.1 However, this is on the backdrop of increasing concern about the risk of burnout of doctors and the impact this may have on patient care.2–8 A report in 2019 by the British Medical Association2 suggested approximately 80% of UK doctors and doctors in training are at high or very high risk of burnout. Though figures vary depending on choice of outcome measure and health system, it is generally acknowledged that rates of burnout and psychiatric morbidity among doctors are worryingly high.3 Impairment to doctors’ well-being negatively affects patient care,4 patient outcomes5 and increases the chance of medical errors,6 7 notwithstanding an association with reduction in clinical hours and retention of doctors.8 9 As such, the well-being of doctors is a concern for many organisations, and recommendations have been formulated to address burnout and improve doctors’ well-being.10 11 These include the necessity to reduce doctor fatigue12 13 and many highlight the importance of breaks for reducing fatigue, improving patient safety and promoting well-being at work.13–15 In response to these recommendations and campaign efforts (eg, the BMJ’s ‘Give Us a Break’ campaign16) in the UK, investments have been made to improve rest facilities.17
What constitutes a ‘break’ within the work context is a wide and variably defined construct, including: holidays and annual leave, career breaks as well as the temporary reprieve taken within a given shift at work (intrawork breaks). A systematic review of the impact of intrawork breaks in industrial settings showed that intrawork breaks in that context maintained performance and helped mitigate fatigue and accident risk.18 However, it remains unclear whether intrawork breaks improve doctors’ well-being and performance as, to our knowledge, no review has been conducted on break-taking literature in this population. This systematic review seeks to specifically understand the impact of intrawork breaks on doctors’ well-being and/or their performance at work.
Method
This systematic review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 statement. The protocol was preregistered with the International Prospective Register of Systematic Reviews (PROSPERO).19
Patient and public involvement
This systematic review is part of a PhD thesis undertaken in the Centre for Workforce Wellbeing at the University of Southampton. As part of that process, there was significant engagement with junior doctors, consultants and patients about the priorities for doctors’ well-being and outcome measurement.
Eligibility criteria
The review included any empirical studies investigating the impact of intrawork breaks on doctors’ well-being and/or performance.
In the absence of an established definition of an intrawork break, we developed an operational one as follows: A cessation of work tasks for a period of up to an hour during a given shift, allowing the individual to temporarily remove themselves from the workspace, physically and/or mentally. An hour period was chosen, as this is typically the maximum duration of lunch breaks in other industries and, for sleep-related break interventions, this would differentiate shorter naps from the equivalent of overnight sleep.
Break ‘interventions’ could include opportunities to rest, mandating breaks, increased frequency of breaks, increased break duration, varied timing of breaks or break activities (eg, yoga, exercise).
Where the study design necessitated a comparator, this could include usual practice, missed work breaks, less frequent breaks, shorter break durations or other break activities.
We included any empirical study design or investigation, undertaken primarily in qualified medical doctors (doctors comprising at least 50% of the sample). Some papers might refer to junior doctors as ‘trainees’. Despite being fully qualified, this is a common term for doctors who are not yet consultants.
No restriction was placed on study design (quantitative or qualitative), language, location or date of publication.
Studies were excluded if:
The break under investigation occurred outside of work hours.
The break under investigation included a work-based activity (eg, reflective practice or administration).
Qualified doctors did not constitute the majority of the sample.
The design was not empirical (eg, opinion pieces, reviews, theoretical modelling).
The break duration was longer than an hour.
The primary outcome of the systematic review was the measured effect(s) of break taking on doctors’ well-being or work performance.
Search strategy
We searched, until 6 June 2021, Embase, PubMed, Web of Science (Core Collection) and PsycINFO databases, using Health Sciences Descriptors and Medical Subject Headings. Bramer et al.20 estimate that this combination should ensure at least 83% coverage of available literature, though this figure is likely to be higher due to PsycINFO being a comparatively more relevant database in this subject area than those included in their calculation. Reference lists of key research papers or reviews were also searched for additional papers not retrieved by the search strategy.
The search comprised three blocks of terms and their synonyms relating to: (1) medical doctors, (2) intrawork breaks and (3) an outcome measure of well-being (eg, burnout, stress, anxiety, fatigue, sleep) and/or work performance (eg, errors, job performance indicators, quality of care, staff absence). Syntactic variations were adapted for each database. See online supplemental material 1 for the search strategy used for each database.
Supplemental material
‘Well-being’ and ‘work performance’ are broad constructs that lack a single definition. As we aimed to be as broad as possible in this search, capturing the breadth of research in the field, we wished to encompass as many working definitions of these constructs as possible through a comprehensive list of search terms. Well-being outcomes referred to any measures of, or related to, mental health, physical health and quality of life. Work performance included any measures of, or related to, clinicians’ ability to carry out their duties, such as errors, adverse events, appraisals, patient feedback, quality of care, revalidation, ability to meet targets and so forth. Outcomes relating to well-being and work performance also often overlap (eg, sickness absence, perceived stress); therefore, it was not our intention to divide the two constructs but rather to be inclusive of any papers investigating either, or both, outcomes. We referred to research papers in the fields of occupational well-being and job performance to gather the extensive list of terms and a subject librarian was consulted throughout to ensure the comprehensiveness of the search.
Study selection
Search results were imported into EndNote X9 software and duplicates were automatically and manually removed. Each study title and/or abstract was assessed by two independent assessors against the inclusion criteria, with an agreement rate of 98.2%. If disagreements occurred between assessors, consensus was achieved through arbitration by a third senior author. Where abstracts indicated potential relevance to the review, corresponding full-text papers were screened for inclusion. If full-text articles were not available in accessible databases, through interlibrary loan, and/or relevant information was not fully explained in the text, authors were contacted for relevant data via e-mail (at least twice). If corresponding peer-reviewed reports were not available, even after request to the corresponding author, conference abstracts were assessed and those with sufficient information for data extraction were included.
Data extraction and analysis
We extracted: first author; year of publication; participant demographics (training level/seniority, specialty/department, gender); location; sample size; study design; definition/type of break; interventions/activities under investigation (and any comparators); evaluated outcome measurements and associated results. If reported, data extraction also included break prevalence, timing and duration of breaks and hindrances or facilitators to break taking. Data extraction for each study was completed by the primary author using a standardised table, and all data extraction was verified by a second, senior author throughout the extraction process.
Data were tabulated for cross-comparison and descriptive analysis. The outcomes of included studies were described according to whether they improve, reduce or have no effect on well-being and/or job performance outcome measures. Due to the substantial variability in study methods, populations and outcome measures used, no meta-analysis was conducted on the data.
Quality appraisals
An assessment of the risk of bias was made by two reviewers independently using the Cochrane risk of bias tool for randomised control trials (ROB-2).21 The Cochrane’s Risk of Bias in Non-randomised Studies (ROBINS-I) tool22 was used to assess non-randomised studies of interventions. Both Cochrane tools allow for an overall risk of bias assessment (ROB-2: low risk of bias, some concerns, high risk of bias; ROBINS-I: low, moderate, serious or critical risk of bias or no information).
For other experimental designs, risk of bias assessment was completed using the relevant Joanna Briggs Institute (JBI) checklists23 for cross-sectional, cohort and qualitative studies. Each question is answered with ‘yes’, ‘no’, ‘unclear’ or ‘not applicable’. The JBI checklists do not provide an overall risk of bias score, however, to allow for intrastudy and cross-study comparison, we have indicated the frequency (%) of possible ‘yes’ answers within each study and across studies. As JBI checklists contain less detail than Cochrane tools, our rationale for JBI ratings is given in online supplemental tables 1–3.
Follow-up studies were assessed separately if the design and/or participants were dissimilar to the original paper.
Results
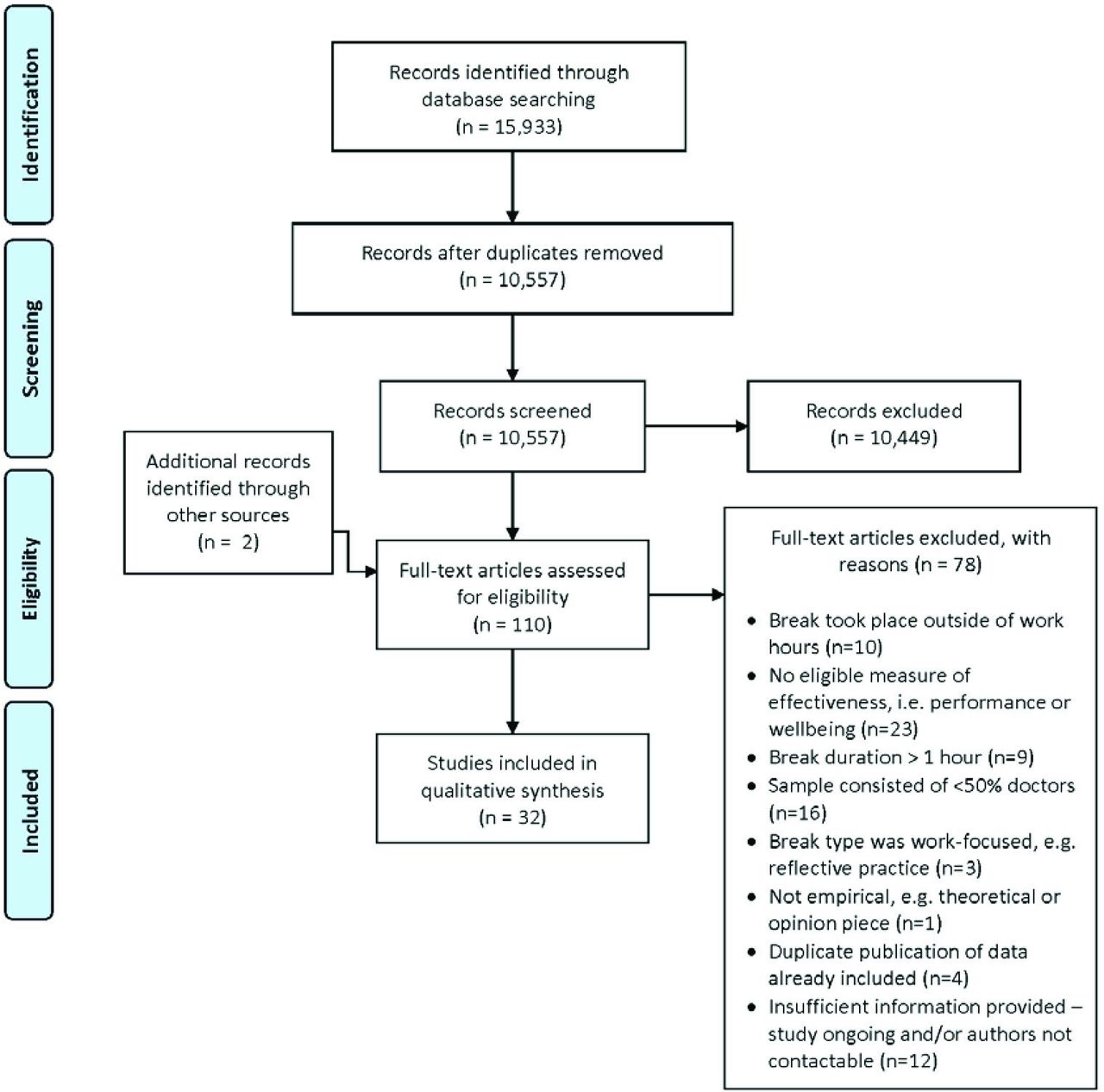
Following removal of duplicates, the titles and abstracts of 10 557 records were assessed for inclusion in the review (see figure 1). Supplementary searches yielded two further records. In total, 32 records met criteria for inclusion. Three records report follow-up data to original papers and as such 29 records contain unique participants and topics.

{kind=link}
PRISMA flow diagram of studies included in the review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis. Based on: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7): e1000097. doi:10.1371/journal.pmed1000097.
See online supplemental table 4 for the summary of results.
Records meeting the inclusion criteria ranged in publication date from the year 2002 to 2021. There was substantial heterogeneity in study design, including randomised control/crossover trials (n=7), non-randomised studies of interventions (n=7), cross-sectional surveys (n=7), cohort (n=4), qualitative (n=6) and mixed-method studies (n=1).
Intervention studies generally comprised relatively small sample sizes, ranging from 7 to 56 participants (median: 27). Of these, the six randomised control trials (RCTs) had sample sizes ranging from 7 to 49 participants (median: 37). Survey and cohort studies were moderately sized, ranging from 27 to 2805 participants (median: 294). Qualitative study sample sizes were varied, ranging from 5 to 116 participants (median: 25).
The break-related topics of investigation were also highly varied. Intervention studies investigated the effect of ‘microbreaks’ (particularly in the specialty of surgery), naps, yoga or exercise sessions and standard 30 min breaks. Surveys and cohort studies investigated a wide range of break-related topics, including the impact of breaks on digital eye strain, reaction time, burnout, stress, affect, vehicle and work-related accidents, inappropriate prescribing, emotional exhaustion, work−home conflict, report errors and healthy eating behaviours. Qualitative methods were used to appraise break interventions as well as to investigate diverse topics such as the importance of breaks to new mothers’ ability to continue breastfeeding following maternity leave, the potential of breaks to improve clinician well-being and fatigue, the culture surrounding breaks and clinician opinions on them. Mixed-method data investigated the role of breaks on ‘sharing ignorance’ (detecting and sharing unknown knowledge and learning from failures) and ‘hiding ignorance’ (deliberately preventing knowledge sharing).
Well-being and performance outcome measures were also dissimilar across studies. Given the substantial variability in types of intervention implemented and measures of outcome (see online supplemental table 4 for full details), inherent heterogeneity in the data meant that any quantitative synthesis could generate spurious findings, and therefore was not undertaken.
Impact of breaks on well-being and performance outcome measures
As study design and break types under investigation varied markedly, they are described here by topic and data type to aid clarity, including quantitative studies of standard 30 min breaks,24 25 sleep-related interventions (naps),26 27 yoga and mindfulness interventions,28–31 microbreaks in surgery,32–35 other microbreak interventions,36 37 surveys38–44 and cohort studies.45–48 Qualitative data are grouped into qualitative evaluations of interventions49 50 and other qualitative studies,51–54 and a single German sequential mixed-method study investigating the impact of breaks on opportunities for physicians to share (or hide) ignorance55 (see online supplemental table 4).
Quantitative study findings: break interventions
Results for standard 30 min breaks were mixed. A German double-blind cross-over trial24 saw no changes to attention, sleepiness or anxiety measured during the shift, while an Australian before/after study25 found breaks improved clinicians’ tiredness, fatigue when measured at the end of each shift and departmental performance (time to see patients, triage and target admission times).
Two sleep-related interventions26 27 conducted in the US showed overall improvement to well-being and performance during both day and night shifts. Twenty minute midday naps in day shifts were associated with improvements in cognitive functioning and attentional failures in first year interns,26 while 40 minute naps during night shifts showed improvement to reaction times, mood, sleepiness and driving performance in emergency department (ED) staff.27 However, no significant changes were seen in memory and simulations of intravenous tasks.
Studies investigating yoga and mindfulness offered the 1-hour sessions within work hours.28–31 These studies (two before/after28 29 and two RCTs30 31) found overall positive improvements to well-being and performance measures such as burnout, anxiety, depression, stress, blood pressure, sleep, professional fulfilment, interpersonal disengagement, resilience and mindfulness. However, no changes were seen in heart rate,29 subjective sleep scores,28 sleep disturbances and affect.31 The US study in faculty physicians31 found that positive findings of reduced burnout, stress, anxiety and depression, and increased professional fulfilment, were not sustained at a 2-month follow-up; while another in US obstetric trainees29 found an overall increase in participants’ weight following the implementation of a yoga programme.
To reduce the common musculoskeletal difficulties associated with prolonged surgery, the effect of microbreaks (breaks of approximately 5 minutes or less) was tested in surgeons in Canada, USA and Germany, using parallel RCTs,34 randomised crossover trials32 33 and before/after study design.35
Results were predominantly positive. Five-minute microbreaks every 30 minutes saw improvements to musculoskeletal strain, cortisol, attention, concentration, doctors’ responses to stressful intraoperative events, intraoperative and postoperative impairment by fatigue and stress—without prolonging the duration of a given surgery nor affecting patient outcomes.33 34 However, doctors’ approval of this type of scheme depended on their preferred way of working.34 Studies also tested microbreaks of a shorter duration (20 second pauses every 20 minutes and 1.5–2 minute breaks every 20–40 minutes), and despite the shorter break time, showed predominantly positive effects.32 35 Twenty-second microbreaks showed improvements to physical discomfort, muscular fatigue and accuracy,32 while breaks of 1.5–2 minutes showed improvement to musculoskeletal pain, physical performance and, for some surgeons, mental performance, with no or minimal effect on surgery duration, difficulty, complexity, distractions, work flow or mental/physical demands.35 Additionally, the majority of surgeons expressed a desire to incorporate this type of shorter micropause into their regular routine.35
Other microbreak interventions included a Canadian study delivering microfood breaks (six small meals) throughout the work day36; and (in France) 5 minute mindfulness meditations prior to breaking bad news to patients.37 Microfood breaks were found to have positive effects on speed and accuracy, blood glucose levels, fluid intake, urine output and caloric intake though no significant reduction in hypoglycaemic nutrition-related symptoms.36 Five minute mindfulness meditations had a positive effect on performance during a simulated bad news consultation; however, it had no significant effect on doctors’ stress, confidence or self-perceived or patient-perceived empathy.37
Quantitative study findings: survey and cohort studies
Cross-sectional surveys investigated various topic areas and used a variety of measures to investigate the impact of break taking. A survey of radiologists in Saudi Arabia found that infrequent break taking was predictive of digital eye strain,38 while in the UK,39 doctors reported lack of breaks as the most common barrier to healthy eating. Two studies (in Egypt and Germany)40 41 found that fewer breaks correlated with, or were predictors of, higher stress levels, whereas a survey of physicians in private practice42 found that break taking negatively correlated with work-home conflict and indirectly correlated with emotional exhaustion. However, a small survey of 46 Tunisian anaesthetists of varying grades43 found no association between break-taking behaviours and levels of burnout. The survey of German doctors41 also found that while shorter break duration was a predictor of work-related accidents, it was not a predictor of motor vehicle accident rates.
Additionally, one cross-national survey44 showed break duration negatively correlated with doctors’ work stress in Sweden but not in Germany.
Cohort studies were prospective and retrospective in design and reported on a variety of measures. One prospective cohort study in Belgium ED physicians45 found that greater use of fatigue reduction strategies (break activities) were associated with faster reaction times but not with levels of burnout. A UK study in trainees46 found that the lack of breaks during shifts was associated with greater negative affect (worry, tiredness, impatience, frustration, etc) and less positive affect (competence, enjoyment, happiness, etc). A retrospective cohort study using secondary analysis of electronic records in the US47 found that doctors were more likely to inappropriately prescribe opioids before than after a break, while another in Switzerland48 showed that report errors (as a surrogate marker of fatigue) reduced after breaks, though this postbreak effect waned as the week progressed.
Qualitative findings: qualitative appraisals of break interventions
Two studies qualitatively appraised interventions. One49 used individual interviews to follow-up the aforementioned Canadian microfood break study36 and found that lack of time, access to break areas and lack of food choices were barriers to adequate nutrition, which in turn impacted doctors’ emotional and physical symptoms, their ability to work and their interactions with colleagues and patients. However, the intervention created greater awareness of nutrition in the workplace and prompted some doctors to change their habits and eat more regularly.
Another small (n=5) qualitative study of an intervention50 used a survey to appraise a weekly 1-hour intrawork exercise session in Canadian rheumatology fellows. Participants reported that work was a barrier to their desired exercise regime and felt that the programme was an effective use of time and resources. The majority found that the programme increased their confidence, and following the programme, the majority were continuing to exercise more regularly.
Qualitative findings: other
Other qualitative studies used focus groups and individual interviews with doctors, and thematically analysed discussions about various break-related topics with a well-being or performance component.51–54
One (UK) focus group study investigated themes regarding breaks as a potential strategy to improve general practitioner (GP) well-being.51 GPs described breaks as a valuable, desirable opportunity to remove oneself from the workplace that is a feasible well-being improvement strategy, though shorter coffee breaks were deemed more feasible than lunch breaks.
Another focus group study53 investigated US ED doctors’ thoughts about the function of breaks. Themes included doctors’ need for breaks for cognitive and emotional functioning, however, when breaks were taken for the benefit of patients or productivity this was more acceptable than if they were taken for self-care alone. Doctors expressed the view that breaks had the potential to hinder work (though this had never personally been experienced) and that taking them required flexibility and attuned organisational skills. Additionally, any culture change around doctors’ break taking was thought to require ‘buy-in’ from colleagues and other staff.
A UK focus group study52 investigated the impact of Working Time Regulations on the experience of fatigue. Themes included fatigue being a threat to doctors’ performance (eg, efficiency and skills) and that this worsened with hunger or discomfort caused by missed breaks. Participants expressed that fatigue was still experienced despite the implementation of regulations, that rest areas were increasingly being reduced, and that senior staff seemed to lack awareness of trainee entitlements to rest.
Finally, an interview study54 with doctors who were also new mothers found that while they valued the ability to breastfeed, this was dependent on their ability to take breaks to express milk.
Mixed-method findings
The only included mixed-method study55 investigated the phenomenon of sharing ignorance and hiding ignorance. The qualitative component of the study (individual interviews) identified breaks as an opportunity to share and hide ignorance, while the quantitative survey showed that breaks significantly facilitated sharing, but not hiding, ignorance.
Quality assessment
The methodological quality of included studies was rather low (see tables 1–5). The risk of bias in randomised studies ranged from ‘some concerns’ to ‘high’ (see table 1), while in quasi-experimental studies ranged from ‘moderate’ to ‘critical’ (see table 2), with most studies being at ‘critical’ risk of bias. This was predominantly due to inherent confounding, a lack of comparator or control groups, the use of subjective criteria and a lack of blinding to intervention status. No randomised or quasi-experimental studies had prepublished their protocols and/or analysis intentions.
Risk of bias in randomised crossover/controlled studies (Cochrane ROB-2)
Risk of bias in quasi-experimental studies (ROBINS)
Risk of bias in observational cohort study (JBI)
Risk of bias in cross-sectional studies (JBI)
Risk of bias in qualitative studies (JBI)
Using the relevant JBI checklist, observational studies (see table 3) met 62% to 100% of applicable criteria; however, many of the questions posed by the checklists were not applicable due to the design of these studies (two were retrospective) and a lack of control or comparison groups.
Cross-sectional designs (see table 4) met 50%–100% of the relevant JBI criteria. In the absence of a standardised, objective measure of break taking, it is not surprising that only two of seven (28.6%) studies41 44 used standard, valid, objective criteria for measurement of break-taking. In these studies, break duration was measured in minutes where other studies dichotomously asked whether participants took breaks at work (‘yes’ or ‘no’) or used a non-validated Likert-type scale dividing break frequency or duration into categories. Additionally, these were the only cross-sectional studies that reported appropriate methods to deal with confounding, despite most studies identifying potential confounders.
Qualitative studies (see table 5) met between 50% and 90% of the JBI checklist criteria. Only two of the seven (28.6%) qualitative studies49 51 reported the cultural or theoretical position of the researcher, and one study53 acknowledged the researcher’s potential influence on the data.
Discussion
The breadth of break-related topics shows that efforts are being made to investigate break effectiveness in doctors. Overall, the existing literature suggests a positive effect of break taking on a range of well-being and performance outcomes. However, comparison of data is hindered by a lack of consensus about which break-related topics and research questions should be prioritised, how these should be researched and measured, and what defines a break, alongside heterogeneity in the type of study design.
Only two included studies investigated the effectiveness of standard 30 minute breaks,24 25 which requires particular attention as it is likely the most common type of break taken by doctors at work. Similarly, only two studies investigated the effect of naps, another common topic of discussion for performance and well-being, particularly for nights and long shifts.
It is unclear whether the content or duration of breaks is more important than the ability to take one. There were mixed findings for standard 30 minute uninterrupted breaks, though this is likely due to a lack of studies on the topic. Naps, microbreaks and yoga and mindfulness interventions showed improvement to well-being and/or performance outcomes. However, outcome measures were dissimilar across studies, preventing valid comparison of break interventions and durations.
Overall, the quality of studies on break effectiveness was rated as suboptimal. While sample sizes for survey and cohort studies were moderate, small samples were used in intervention studies and RCTs. Additionally, existing experimental (and non-experimental) studies carry a moderate to severe risk of bias due to inherent confounding, a lack of blinding or control groups. This is problematic as experimental designs would provide the best approximation of break effectiveness and causality. While the feasibility of blinded experiments in break-taking research is low and unlikely, there is scope to reduce confounding and introduce more RCTs in this area.
Qualitative research provides some nuanced understanding of break phenomena; however, existing qualitative literature does not tend to locate researchers culturally, theoretically and philosophically, nor does it acknowledge the potential influence of the researcher on findings.
As a construct, intrawork breaks lack an agreed definition and a standardised means of measurement. There appears to be no consensus on what delineates a break (temporally, contextually or behaviourally) or how to measure it reliably and validly. Indeed the use of validated instruments for measures of well-being or performance was low overall. This lack of agreement further prevents comparisons of data and conclusions about the effectiveness of breaks.
As (to our knowledge) this is the first systematic review of break taking in doctors, we did not place any limits on study design. While this provides a comprehensive review of existing empirical evidence, this review also highlights the substantial variability in types of intervention implemented and measures of outcome used, resulting in a marked heterogeneity of data which make further quantitative synthesis potentially misleading.
Given the heterogeneity in design, quality, research questions and outcomes of existing studies, it is not possible to conclude with certainty whether intrawork breaks improve well-being and performance in doctors, though the existing evidence suggests a positive trend. This positive effect aligns with existing research in industrial contexts,18 despite contextual differences between industry and healthcare settings.
To properly understand the effectiveness of breaks for doctors and justify financial and organisational investment in break facilitation, agreement among policymakers, regulators and research bodies regarding the research priorities would allow the evidence base to be developed quickly and effectively. From the results of this systematic review, such priorities could include: agreed international standardised definitions of intrawork breaks, development of outcome measures of well-being for doctors56 and consensus on the most robust methodologies to test the effectiveness of intrawork break interventions in real-world situations. There is clearly a need for valid and reliable outcome measures that do not conflate well-being with the absence of distress,57 across a range of potential performance outcome measurements as well as ways of measuring impact on patient care.58
The COVID-19 pandemic has highlighted the importance of ensuring workforce well-being, but the evidence of what works best for whom in terms of intrawork breaks remains uncertain.
Data availability statement
Data supporting this study will be openly available from the University of Southampton public, open access repository following thesis submission in July 2023, as the work forms part of a PhD. Supplemental material. This content has been supplied by the authors. It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Ethics statements
Patient consent for publication
Ethics approval
As a systematic review of the literature, no ethical approval was required.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @drjmas
Contributors AON: designed the study, collected, analysed and interpreted the data and wrote the first draft of the article. She led on the response to reviewers. JS guarantor, overseeing study design, data collection and analysis, edited and approved the final version of the article. DSB: funding acquisition, contributed to design of the study and data analysis, and approved the final version of the article. SC contributed to design of the study and data analysis and approved the final version of the article. All authors contributed to, and agreed the revisions following review.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.