Article Text

Abstract
Background and aims Endoscopic submucosal dissection (ESD) remains an investigational issue for early gastric cancer (EGC) with expanded indications owing to the risk of lymph node metastasis. In this study, we aimed to evaluate the clinical outcomes and safety of ESD versus surgical resection (SR) for EGC with expanded indications.
Methods The systematic review selected studies from PubMed, Embase, Cochrane and Web of Science databases from 2010 to 2020, and compared survival and clinical safety data of ESD with those of surgical resection for EGC with expanded indications. The fixed-effects or random-effects model was used to calculate the differences between the two groups. To assess the validity of the eligible studies, risk of bias was measured using the Newcastle–Ottawa Quality Assessment Scale.
Results Nine retrospective studies were used to calculate the differences in survival and clinical safety data between the two groups for EGC with expanded indications. Differences were not significant between the groups in terms of age, sex, tumour size, tumour histology or lesion morphology. Regarding tumour site, tumours located in the L area (the lower third of the stomach) were more likely to be found in the ESD group. With regard to metachronous and synchronous carcinomas, there was a significant difference favouring SR treatment (metachronous: OR=0.12, 95% CI=0.05 to 0.25, p<0.00001; synchronous: OR=0.11, 95% CI=0.02 to 0.46, p=0.003). Adverse event data were identified in six studies showing a significant difference favouring ESD treatment (ESD vs SR, OR=0.49, 95% CI=0.34 to 0.72. p=0.002). Additionally, six studies evaluating 5-year overall survival showed no significant differences between the two groups (HR=1.22, 95% CI=0.66 to 2.25, p=0.53). With regard to 5-year disease-free survival, patients with expanded indication EGC undergoing SR showed better survival (ESD vs SR, HR=3.29, 95% CI=1.60 to 6.76, p=0.001).
Conclusion ESD provided favourable results for patients with EGC with expanded indications regarding clinical outcomes and safety in retrospective studies. Further, to detect synchronous or metachronous lesions, endoscopic surveillance should be performed following ESD. However, the included studies were observational, some did not have adequate adjustment for confounding factors and their results lacked generalisability due to their origin. Thus, further related randomised controlled trials are urgently encouraged.
PROSPERO registration number CRD42021251068.
- Endoscopy
- Gastrointestinal tumours
- Gastrointestinal tumours
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The meta-analysis combined data across the included studies to calculate the difference between endoscopic submucosal dissection and surgical resection treatment for patients with early gastric cancer with expanded indications.
The systematic review of the PubMed, Embase, Cochrane and Web of Science databases was performed for studies from 2010 to 2020 comparing survival data and clinical safety.
The Newcastle–Ottawa Quality Assessment Scale and Scottish Intercollegiate Guidelines Network checklist were used to measure the risk of bias in cohort studies.
The HR and its SE were estimated using the method described by Tierney et al.
As the retrospective nature of the selected studies presented selection biases, the present study has some limitations when compared with studies of randomised trials.
Introduction
Despite improvements in surgical procedures and therapeutic strategies, gastric cancer remains one of the most common cancer-related causes of death worldwide.1 2 Radical gastrectomy is considered the optimal choice for locally advanced resectable gastric cancer3; however, while this procedure can obtain adequate resection margins and lymph node dissection, it poses significant perioperative complications and may impair long-term gastrointestinal function and quality of life. Early gastric cancer (EGC), defined as an invasive cancer involving the mucosa or submucosa irrespective of the nodal status,4 may be treated by endoscopic resection, which offers the advantages of minimal invasiveness, low cost, good patient tolerance and high quality of life following the procedure.5 6 In fact, endoscopic resection has been accepted as the standard treatment for patients with EGC and a negligible risk of metastatic lymph nodes in eastern countries.7 According to the 2010 Japanese Gastric Cancer Treatment Guidelines, the absolute indication for EGC is strictly limited to mucosal lesions with a differentiated histopathological type and without ulceration or lymphatic-vascular invasion, and a size smaller than 2.0 cm.8–10 Additionally, owing to the development of endoscopic devices and techniques, endoscopic submucosal dissection (ESD) can achieve en bloc and complete resection, offering a reduction in postoperative residual lesions and local recurrence. The expanded indications include: (1) differentiated mucosal cancer without ulceration, irrespective of tumour size (>20mm); (2) differentiated mucosal cancer with ulceration and diameter ≤30 mm; (3) differentiated submucosal penetrative cancer with depth <500 µm (SM1) and diameter ≤30 mm; and (4) undifferentiated mucosal cancer without ulceration and diameter ≤20 mm.8 In prior cohort studies, the long-term favourable outcomes of ESD for EGC in patients meeting the expanded indication criteria when compared with those meeting the absolute indication have been demonstrated.11 According to the 2010 Japanese Gastric Cancer Treatment Guidelines, ESD is regarded as the investigational treatment for EGC lesions that meet the expanded indication criteria.12 Several studies have suggested that lymph node metastasis occurs after curative ESD in EGC meeting the expanded indication criteria.13–16 However, the Japanese treatment guidelines were revised in 2018 (Japanese Gastric Cancer Association: Japanese gastric cancer treatment guidelines 2018 (5th edition) Gastric Cancer 2021, 24:1–21). According to these guidelines, a differentiated-type adenocarcinoma without ulcerative findings (UL0) in which the depth of invasion is clinically diagnosed as T1a and the diameter is >2 cm, and a differentiated-type adenocarcinoma with ulcerative findings (UL1) in which the depth of invasion is clinically diagnosed as T1a and the diameter is ≤3 cm, are classified as absolute and not expansive indications, based on the results of the JCOG0607 trial.7 In addition, an undifferentiated-type adenocarcinoma without ulcerative findings (UL0) in which the depth of invasion is clinically diagnosed as T1a and the diameter is ≤2 cm will also be classified as an absolute indication based on the results of the JCOG1009/1010 trial.17 However, the JCOG0607 and JCOG1009/1010 trials were designed as non-randomised single-arm confirmatory trials, not both-arm studies, without comparisons between ESD and gastrectomy for expanded indication gastric cancer. Thus, the validity of the expanded indications for endoscopic submucosal versus gastrectomy resection remains controversial. Therefore, this study aimed to evaluate the outcomes and clinical safety of ESD versus surgical resection for EGC with expanded indications.
Methods
This meta-analysis was reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations18 (PRISMA 2020 checklist) and the Assessing the Methodological Quality of Systematic Reviews Guidelines. Additionally, this research was registered in PROSPERO (CRD42021251068).
Eligibility criteria
We included studies that involved a comparison of ESD and surgical resection (SR) for EGC with expanded indications: (1) differentiated mucosal cancer without ulceration, irrespective of tumour size(>20mm); (2) differentiated mucosal cancer with ulceration and diameter ≤30 mm; (3) differentiated submucosal penetrative cancer with depth <500 µm (SM1) and diameter ≤30 mm; and (4) undifferentiated mucosal cancer without ulceration and diameter ≤20 mm. The included studies explicitly reported data on at least one of the following outcomes: en bloc resection, complete resection, metachronous cancer, synchronous cancer, procedure-related adverse events, or short-term and long-term prognoses. Additionally, we included only studies that were clinical randomised or non-randomised controlled trials or observational studies of adequate quality. Duplicate publications, secondary literature, conference papers, abstracts, letters, editorials, expert opinions, case reports and studies that lacked clinical endpoint data were excluded.
Literature search
As the 2010 Japanese Gastric Cancer Treatment Guidelines stated that ESD was regarded as the investigational treatment for EGC lesions that meet the expanded indication criteria, the systematic review of the PubMed, Embase, Cochrane and Web of Science databases was performed for studies from 2010 to 2020 comparing survival data and clinical safety of ESD versus SR for EGC with expanded indications. The search strategy combined the National Institute of Health Medical Subject Heading Index terms and free text regarding “endoscopic submucosal dissection,” “gastric cancer” and “surgery” (online supplemental file 1—search strategy). The reference lists of the included articles were then searched to identify additional relevant studies.
Supplemental material
Data extraction
Two reviewers were blinded to independently extract the following standard information from each included article: study characteristics (first author, year of publication, country and sample size), participant characteristics (age, tumour size, depth of invasion, location, tumour morphology, tumour histology, absolute indication or expanded indication), intervention (ESD vs surgery resection or gastrectomy plus lymphadenectomy) and outcome data (en bloc resection, complete resection, procedure-related adverse events and survival data). We reviewed the text, tables and figures to identify relevant items, and extracted the data. In cases of disagreement between the two reviewers, an additional reviewer re-evaluated the relevant studies and the group reached a consensus.
To assess the validity of eligible studies, the Newcastle–Ottawa Quality Assessment Scale and Scottish Intercollegiate Guidelines Network checklist were used to measure the risk of bias for cohort studies.19 The GRADE (Grade of Recommendations Assessment, Developmentand Evaluation) tool (GRADEpro) was then used to assess the quality of the evidence provided by the pooled results, with evidence graded as very low, low, moderate or high.
Outcomes
Complete resection was defined as resection of a tumour without histological evidence of tumour cell involvement on the lateral and vertical resection margins; en bloc resection referred to the resection of a tumour in one piece without a visible residual tumour. If patients received no curative resection, they underwent additional surgery (ESD or gastrectomy plus lymphadenectomy) or follow-up. Additionally, synchronous gastric cancer was regarded as a new cancer at a previously uninvolved site in the remnant stomach occurring within 1 year of treatment, and metachronous gastric cancer occurred more than 1 year after treatment. Procedure-related adverse events included bleeding, ileus, intra-abdominal abscess, anastomotic site leakage, etc.
Statistical analysis
RevMan V.5.3 software for Windows (Cochrane, London, UK) was used to analyse data extracted from the included literature. ORs with 95% CIs were used to estimate and analyse dichotomous variables, and continuous variables were analysed using the weighted mean difference with 95% CI. Considering that both disease-free survival (DFS) and overall survival (OS) are time-to-event outcomes, the HR between the two survival distributions was used as a summary statistic. In each trial, HR and its SE were estimated using the method previously described by Tierney et al.20 Assuming homogeneity of individuals, HR estimates of individual studies were incorporated into an overall HR using a fixed-effects model. If significant heterogeneity was observed, a random-effects model was used. Heterogeneity across studies was assessed using χ2 and I2, and was calculated if the I2 value was >50%. We investigated sources of heterogeneity by subgroup hypotheses: type of study design (propensity score matching (PSM) group vs non-PSM group). Funnel plots were used to investigate publication bias. All statistical tests were two sided, and statistical significance was set at p<0.05.
Patient and public involvement
This study did not include patient or public involvement as it focused on statistical methods for the meta-analyses of studies. All analyses were performed based on data that had been previously published in the literature.
Results
Studies and patients
Nine retrospective studies were included (figure 1, table 1 and PRISMA flow chart),21–29 with 2479 cases, of which 995 (40.1%) were in the ESD group. Assessment of quality according to the Newcastle–Ottawa Scale showed that the included studies with seven scores or more were considered acceptable or high-quality studies. Baseline patient characteristics are presented in table 2, and the key covariates selected to match the ESD and SR groups in the PSM design studies are listed in table 3. A summary table of the GRADE evidence profile was established based on the evaluation of the risk of bias, inconsistency, indirectness, imprecision and other considerations, and is shown in table 4. There were no significant differences between the groups in terms of age, sex, tumour size, tumour histology or lesion morphology. In terms of the tumour site, tumours located in the L area (the -lower third of the stomach) were more likely to be found in the ESD group (p=0.02).
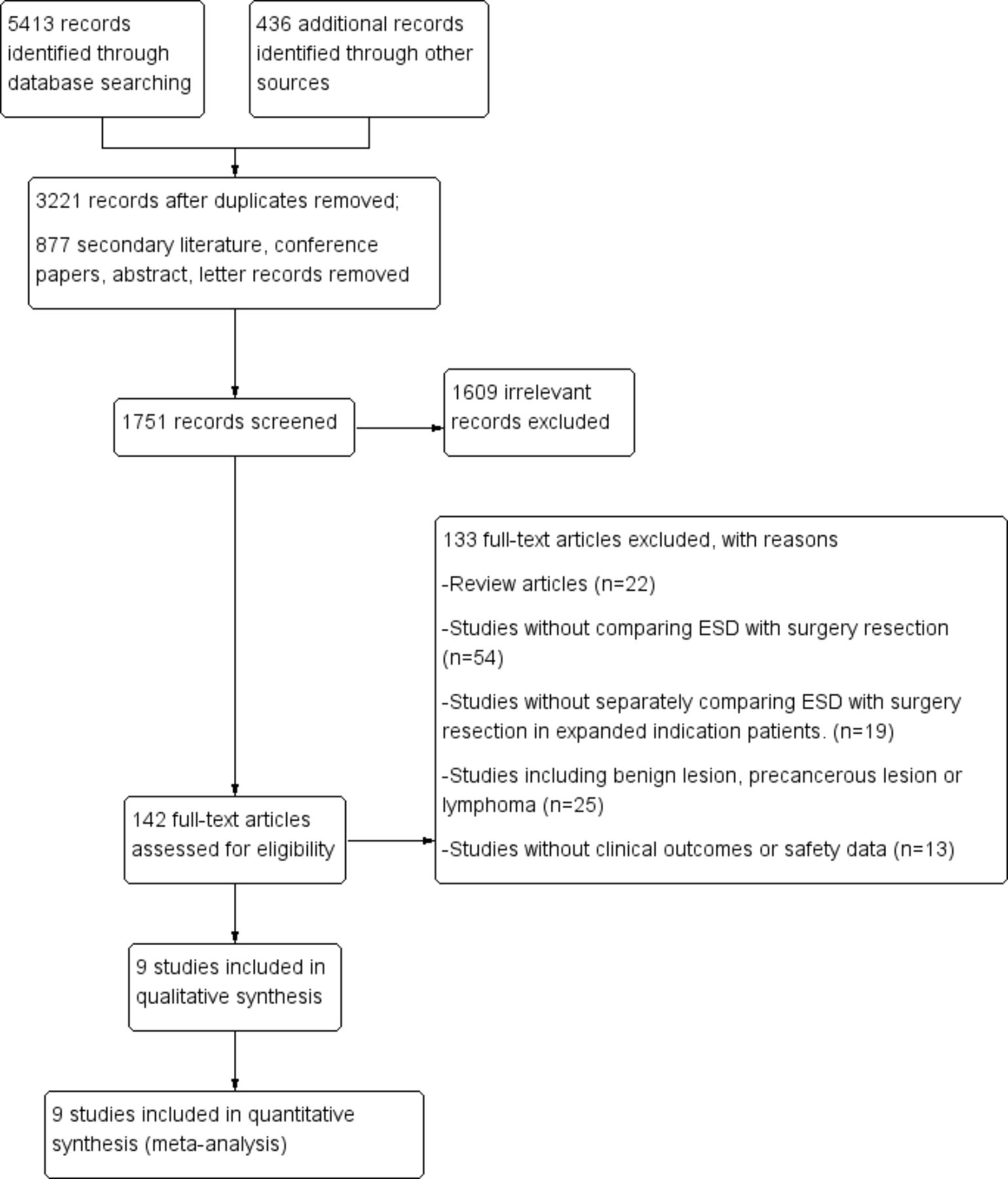
Flow chart illustrating the study selection process. Finally, a total of nine studies were included to calculate differences of survival data and clinical safety between the two groups for EGC with expanded indication. EGC, early gastric cancer; ESD, endoscopic submucosal dissection.
Summary of included studies in the meta-analysis
Outcomes of meta-analysis of baseline characteristics of the included studies
The key covariates to match ESD group and SR group of PSM design study
GRADE evidence profile
Short-term outcomes (synchronous or metachronous gastric cancer) and safety
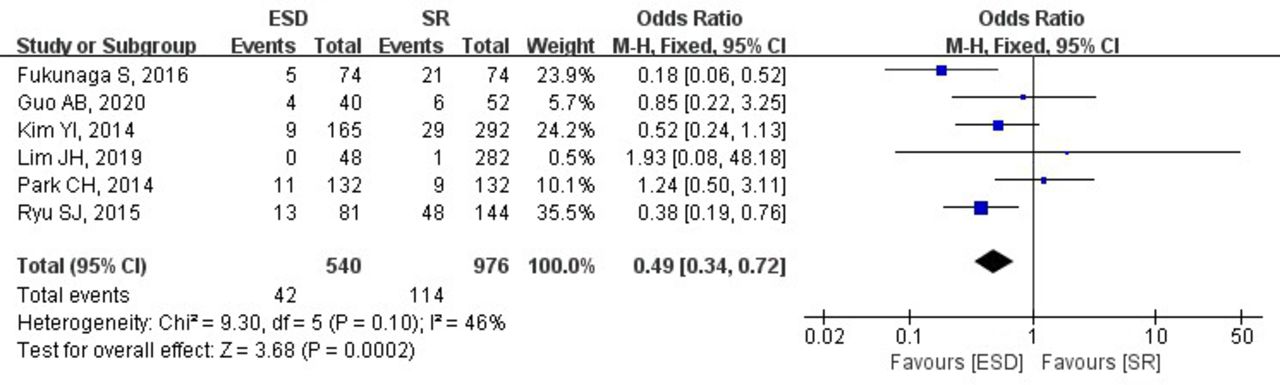
With regard to metachronous gastric cancer, relevant data were identified in eight studies (2148 patients, figure 2), and synchronous data were observed in four (978 patients, figure 3). Pooling the data from the included studies that assessed metachronous and synchronous carcinoma showed a significant difference favouring SR treatment (metachronous: OR=0.12, 95% CI=0.05 to 0.25, p<0.00001; synchronous: OR=0.11, 95% CI=0.02 to 0.46, p=0.003). There was no statistical heterogeneity between the studies (metachronous: I2=0, p=0.46; synchronous: I2=0, p=0.66). Adverse event data were identified in six studies (1516 patients) with no statistical heterogeneity (I2=46%, p=0.10). The included studies showed a significant difference favouring ESD treatment for expanded indication EGC with fewer procedure-related adverse events (ESD vs SR, OR=0.49, 95% CI=0.34 to 0.72. p=0.002, figure 4).

Forest plot of metachronous gastric cancer. ESD, endoscopic submucosal dissection; SR, surgical resection.
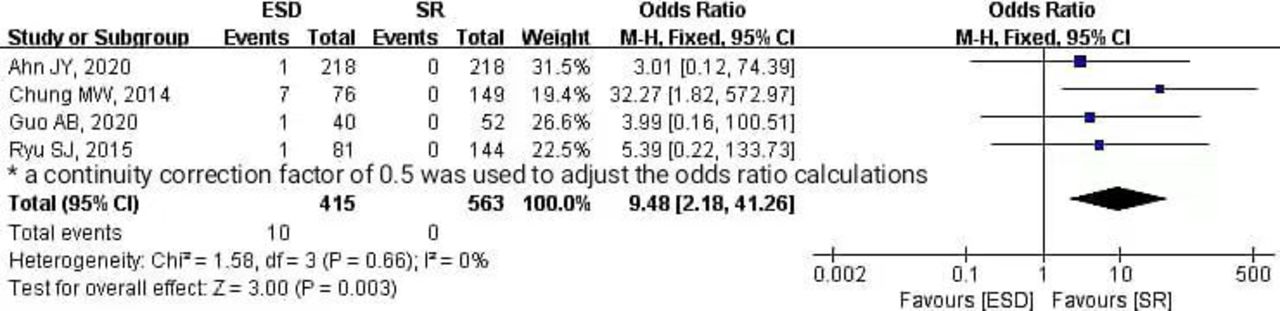
Forest plot of synchronous gastric cancer. ESD, endoscopic submucosal dissection; SR, surgical resection.

Forest plot of adverse events. ESD, endoscopic submucosal dissection; SR, surgical resection.
Long-term outcomes
Six studies evaluated the 5-year OS in 1727 patients and showed no significant difference between the two groups (HR=1.22, 95% CI=0.66 to 2.25, p=0.53, figure 5A), and the heterogeneity between studies was not significant (I2=46%, p=0.53). Similarly, in subgroup analysis, no significant difference associated with 5-year OS was detected between the two groups (PSM: HR=1.22, 95% CI=0.65 to 2.30, p=0.54; non-PSM: HR=1.19, 95% CI=0.09 to 15.75, p=0.90, figure 5B). However, with regard to 5-year DFS, which was analysed in four studies with 1084 cases, patients undergoing SR showed better survival than those undergoing ESD for expanded indication EGC (ESD vs SR, HR=3.29, 95% CI=1.60 to 6.76, p=0.001), and there was no statistical heterogeneity (I2=46%, p=0.71, figure 6A). Subgroup analysis (PSM and non-PSM groups) also showed a significant difference favouring SR treatment (ESD vs SR, PSM: HR=2.85, 95% CI=1.16 to 6.96, p=0.02; non-PSM: HR=4.30, 95% CI=1.27 to 14.54, p=0.02, figure 6B) with negligible heterogeneity (PSM: I2=8%, p=0.30; non-PSM: I2=0, p=0.94).

Forest plot of 5-year overall survival, the overall analysis (A) and subgroup analysis (B) of survival data. ESD, endoscopic submucosal dissection; PSM, propensity score matching; SR, surgical resection.

Forest plot of 5-year disease-free survival, the overall analysis (A) and subgroup analysis (B) of survival data. ESD, endoscopic submucosal dissection; PSM, propensity score matching; SR, surgical resection.
Sensitivity analysis and publication bias
Excluding one study at each time point from the included studies, sensitivity analysis associated with metachronous data, synchronous data and survival data showed the robustness of the pooled effect estimates. Additionally, the funnel plot showed that publication bias was not evident for metachronous gastric cancer (figure 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot of studies that were compared for metachronous gastric cancer shows no evidence of publication bias.
Discussion
The meta-analysis in this study combined data from across the included studies to calculate the difference between ESD and SR treatment with regard to survival data and clinical safety for EGC with expanded indications in a single study, presently representing the largest number of cases associated with comparisons of ESD and SR. It demonstrated that although the short-term outcome of metachronous or synchronous gastric cancer occurrence was more favourable in the SR group, ESD was associated with fewer procedure-related adverse events, embodying the advantages of minimal invasiveness, good patient tolerance and high quality of life after surgery while retaining the function of the gastrointestinal tract. Even if gastrectomy plus lymphadenectomy (SR group) was superior to ESD in terms of 5-year DFS for EGC with expanded indications, the long-term outcome of 5-year OS associated with ESD treatment was similar to that of SR treatment. ESD provided favourable results for EGC with expanded indications in terms of clinical outcome and safety; however, to detect synchronous or metachronous lesions, endoscopic surveillance should be performed following ESD. However, the studies included were observational. Further, some did not have adequate adjustment for confounding factors, and the results lacked generalisability due to the origin of the studies. Therefore, randomised controlled trials in the near future are recommended.
Endoscopic submucosal resection was once considered a treatment option for EGC with absolute indications. Regarding expanded indications, ESD was regarded as the investigational treatment for EGC with a negligible risk of lymph node metastasis. However, several studies reported comparisons of survival data between the absolute and expanded indications for EGC treated with ESD and demonstrated that no statistical difference was detected. It was concluded that ESD may be an alternative treatment for EGC with no or negligible risk of lymph node metastasis meeting the expanded indication.30 No high-quality randomised controlled trials have been conducted to investigate whether gastrectomy plus lymphadenectomy (SR) is superior to ESD in terms of clinical outcome and safety.31 Fukunaga et al and Lim et al (both PSM retrospective studies) showed SR to have a more favourable 5-year OS than ESD for EGC with expanded indications.25 28 In contrast, the remaining studies have deemed no significant differences between the two groups. Finally, in this study, pooling the data of the included studies that assessed long-term outcomes showed no significant differences favouring SR treatment. However, with regard to 5-year DFS, patients undergoing SR had better survival than those undergoing ESD with expanded indication. The less favourable prognosis of ESD may result from more synchronous or metachronous gastric cancer following ESD treatment in the remnant stomach. Synchronous or metachronous gastric cancer was a critical concern as to whether it was actually rational to receive ESD treatment instead of SR treatment for EGC meeting the absolute indication.32–35 It is proposed that the expanded criteria are based on surgical specimen evaluation; however,
surgeons typically choose treatment modalities with limited information, such as histopathology of biopsy specimens and gross endoscopic finding.9 26 In some cases, histological discrepancies between endoscopic and endoscopic resection specimens may exist,36 and it is possible that some stomach intraepithelial neoplasia or precancerous lesions that could develop into synchronous or metachronous lesions are easily neglected by endoscopic gross findings or histopathology of biopsy specimens. Second, ESD treatment preserved the whole stomach, so the incidence of synchronous or metachronous lesions was higher than that of the SR method. Previous studies have suggested that additional surgery should be offered to patients with synchronous or metachronous lesions or who underwent non-curative endoscopic resection.37 38 Intensive and persistent endoscopic surveillance should be performed after ESD to detect synchronous or metachronous lesions. Perhaps, owing to the detection of synchronous or metachronous lesions and additional surgery, ESD treatment has a non-inferior prognosis of 5-year OS for EGC with expanded indications.
ESD is considered a minimally invasive procedure with the merits of low cost, good patient tolerance and high quality of life after surgery; however, few studies have directly compared the clinical safety of ESD with that of surgery for EGC meeting the expanded indications. This meta-analysis suggested that the ESD method was superior to SR treatment with fewer procedure-related adverse events and lower mortality.23–26 28 29 Most included studies were PSM retrospective studies that increased the level of evidence in a single retrospective cohort study.
The present study had some limitations. First, compared with randomised trials, the retrospective nature of the selected studies presented selection biases. More specifically, observational studies lack generalisability because of their origin, and treatment selection for endoscopic resection or surgery was not based on randomisation. To minimise selection bias, some studies were designed as PSM studies, but hidden biases remained because of unmeasured confounders. The key covariates to match the ESD and SR groups in the PSM design study differed, which also led to selection biases. Second, publication bias refers to the problematic tendency of researchers to report positive or good results, resulting in a misleading bias across the overall published literature.39 Publication bias of metachronous lesions was measured using funnel plots. However, for the survival data, analysis of funnel plots was unnecessary because of the small number of included studies. Third, the Newcastle–Ottawa Scale used to assess the quality and bias in cross-sectional and longitudinal studies has a number of limitations, such as the low agreement between two independent reviewers in applying the scale, particularly where authors have not been adequately trained in the methodology. Finally, the quantification of heterogeneity is regarded as one component of a rough estimation of variability across studies, but the observed degree of inconsistency may have clinical implications.
In conclusion, ESD provides favourable results for EGC with expanded indications in terms of clinical outcome and safety in retrospective studies, while to detect synchronous or metachronous lesions, endoscopic surveillance should be performed following ESD. However, as observational studies lack generalisability because of their origin, prospective randomised controlled studies should be conducted to verify the clinical outcome and safety for EGC treated with ESD with expanded indications.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study did not include patient or public involvement as it focused on statistical methods for the meta-analyses of studies. Ethics Committee(s) exempted this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors XX conceived the study. XX, GZ, NG and ZZ developed the study design. GZ, ZZ and NG screened the literature and performed the data extraction. NG and ZZ performed the statistical analysis. NG was responsible for the overall content as the guarantor. XX wrote the first and successive drafts of the manuscript. XX, GZ, NG and ZZ interpreted the data, critically revised the manuscript for important intellectual content and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.