Article Text

Abstract
Objectives To examine the prevalence and the associated factors of burnout among both healthcare workers (HCWs) and the general working population, which has not yet been unknown, using large-scale, nationwide data.
Design Cross-sectional internet-based study.
Setting Nationwide internet survey conducted between 8 and 26 February 2021 in Japan.
Participants Workers aged 20–64 years. We classified the workers as HCWs and the general working population.
Exposures Demographic characteristics (age, sex and marital status), socioeconomic status (education, employment and income), health-related, work-related and industry-related factors (smoking, alcohol use, physical and psychiatric comorbidities, working hours, types of healthcare professionals, experience on the COVID-19 frontline and working industries).
Main outcome measures Burnout defined as a score of ≥3 points on the Mini-Z Single-Item Burnout Scale.
Results Of the included 12 650 workers, 1087 were HCWs. After inverse probability weighting on data from the 2016 Comprehensive Survey of Living Conditions, burnout in HCWs and the general working population was 33.5% (95% CI 29.2% to 38.0%) and 31.0% (95% CI 29.7% to 32.4%), respectively. In the weighted multivariable modified Poisson regression models, working 60 hours or more was associated with burnout in all workers (HCWs: prevalence ratio (PR) 2.52, 95% CI 1.68 to 3.76; general population: PR 1.26, 95% CI 1.07 to 1.48). Widowed/separated compared with married was associated with burnout only among HCWs (PR 1.69, 95% CI 1.16 to 2.47), whereas presence of physical or psychiatric comorbidities was associated with burnout among the general working population (PR 1.14, 95% CI 1.03 to 1.28; and PR 1.65, 95% CI 1.45 to 1.87, respectively).
Conclusions Burnout was prevalent in both HCWs and the general working population in Japan. Both common and specific risk factors were observed. Our findings highlight the need for the general workplace policy and targeted interventions for burnout prevention.
- mental health
- occupational & industrial medicine
- public health
Data availability statement
No data are available. The data used in this study are not available in a public repository because they contain personally identifiable or potentially sensitive participant information. Based on the regulations for ethical guidelines in Japan, the Institutional Review Board of the Osaka International Cancer Institute has imposed restrictions on the dissemination of the data collected in this study. All data inquiries will be channelled through TT (tabuchitak@gmail.com) to Osaka Cancer Institute Institutional Ethics Committee.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Using homogenous large-scale survey data in Japan, this study revealed the burnout and associated factors among healthcare workers and the general working population, all of which were underexamined.
This study only evaluates the burnout symptoms measured by Mini-Z Single-Item Burnout Scale.
There may be concerns about the differences between respondents from the internet survey and the general public in Japan.
There may also be concerns about temporal or geographical external validity.
Introduction
The COVID-19 pandemic, which originated in December 2019, has become a global health crisis. As of 11 April 2022, more than 497 million confirmed cases and 6.1 million deaths had been attributed to COVID-19 according to WHO.1 Besides high rates of infection and mortality, the COVID-19 pandemic has impacted healthcare systems, causing shortage of health resources and overwhelming demands of acute care.2 The pandemic has necessitated major lifestyle changes, such as universal mask wearing, social distancing and home confinement, for maintaining healthcare systems.3 The sociocultural changes and economic difficulties caused by the prolongation of the pandemic have led to various psychological problems, such as fear, anxiety and burnout, in general populations over the long term.4
Burnout, characterised by emotional exhaustion, depersonalisation and personal accomplishment, is one of the most relevant psychological issues among workers because it has serious physical, psychological and occupational consequences.5 Burnout was a common phenomenon even before the COVID-19 pandemic, as a study from the Netherlands reported that 3%–7% of all workers in various industries experienced burnout.5 During the pandemic, burnout has been particularly prevalent among healthcare workers (HCWs), because they have struggled with patient care in under-resourced healthcare systems.6 Additionally, among the general working population, workers have been exposed to substantial COVID-19-related stress emerging from workplace factors, such as missing or insufficient workplace policy and inadequate protective equipment supply.7 In fact, some studies have reported on burnout among non-HCWs during the pandemic, such as hotel employees.8 Although assumptions have been made regarding different occupations’ relative risks for burnout during the pandemic, such speculations have been based on comparisons across heterogeneous studies.9 10 Differences in study populations, settings or trends in the number of newly diagnosed COVID-19 cases have made it difficult for policymakers to ascertain the full extent of burnout. Thus, there is a need for large-scale, nationwide studies incorporating sufficiently large representative samples including HCWs and non-HCWs and examine the rates of burnout during the COVID-19 pandemic. However, to our knowledge, such evidence has been rather scarce.
Therefore, we aimed to clarify the prevalence of burnout among HCWs and the general working population separately during the COVID-19 pandemic, using Japanese large-scale internet survey data with various occupational disciplines. Furthermore, we focused on exploring the factors associated with burnout in these populations, which is crucial to identify individuals who are more susceptible to burnout. We hypothesised that those factors vary in each working population. Hence, we examined such factors among HCWs and the general working population separately.
Methods
Study design and survey participants
We conducted a cross-sectional study using data from a large-scale internet survey called the Japan ‘COVID-19 and Society’ Internet Survey (JACSIS). The JACSIS is a longitudinal study project comprising a series of biannual internet surveys since August 2020. As of 1 January 2022, three survey waves had been conducted; in this study, we used data from the second wave (n=26 000). Participants of the JACSIS in the first wave were recruited from a survey panel provided by a Japanese internet research agency (Rakuten Insight, Tokyo, Japan) that has approximately 2.3 million panellists and their socioeconomic status information. Participants in the first wave were recruited from among 224 389 panellists aged 15–79 years, who were randomly sampled from the total panellists. We conducted the enrolment for the first wave between 25 August and 30 September 2020 until the targeted number of respondents (n=28 000) was reached. When enrolling the participants, the agency stratified the participants by sex, age and prefecture (covering all 47 prefectures in Japan) and matched them on the distribution of the general Japanese population in 2019. The respondents of the second wave of the JACSIS were enrolled between 8 and 26 February 2021. The period was in the middle of the third wave of the COVID-19 pandemic, from 1 November 2021 to 31 March 2021.11 12 During the enrolment, the average daily numbers of SARS-CoV-2 infections and deaths due to COVID-19 were 1267 and 74, respectively; and the vaccine coverage was less than 1%.11 12 In each survey, we collect different information about the COVID-19 pandemic. Because we obtained burnout-related variables only in the second survey wave, we used the data in this study. For enrolment of the second wave participants, we primarily recruited those who had participated in the first wave; 81.6% (22 840/28 000) of the respondents from the first wave participated in the second wave. To achieve the targeted response number in the second wave (n=26 000), we additionally recruited 3160 participants from randomly sampled panellists as described above.
The online questionnaire was designed such that respondents had to answer each question before they could proceed to the next, ensuring that no missing data were generated.
Inclusion and exclusion criteria
Of the 26 000 respondents in the second wave, we included respondents who had not chosen any of the following options to report their employment status: ‘student’, ‘retired’, ‘househusband/housewife’, ‘unemployed’. Further, respondents aged 20–64 years were included according to the definition of a working-age population in the literature.13 We excluded respondents with straight-lining responses, that is, if they chose the same response option to answer all questions in a set of questions. In addition to these exclusion criteria, we performed an attention check using the following instruction: ‘Please choose the answer second from the bottom.’ Respondents who selected responses other than the second answer from the bottom were excluded.
Definition of types of industry
In each wave of the JACSIS, respondents have been asked to report their working industry. Based on our questionnaire and the International Standard Industrial Classification of All Economic Activities,14 we classified the respondents’ working industry into the following 16 types: agriculture, forestry, fishing, mining; utilities; construction; manufacturing; wholesale trade; retail trade; transportation, warehousing; information services; finance, insurance; real estate, rental, leasing; education services; healthcare; social assistance; accommodation, food services; other services; and public administration. Subsequently, we identified HCWs working in the field of social assistance, such as public health nurses.15 To identify this population, we asked respondents classified as working on social assistance whether they were HCWs, and based on their responses, we reclassified them as HCWs.
Exposure variables
Exposure variables of interest were demographic characteristics, socioeconomic status, health-related status and work-related factors. The demographics included age group (20–29, 30–39, 40–49, 50–59, 60–64 years), sex (male, female) and marital status (unmarried, married, widowed/separated).16 The socioeconomic status included educational attainment (high school educated or lower, college educated or higher),17 employment status (employer, self-employed, regular employee, non-regular employee)18 and equivalent household income calculated by dividing the household income by the square root of household size (categorised by the tertiles of equivalent household income (low, –JPY2.49 million (Japanese yen); intermediate, JPY2.5–JPY4.29 million; high, JPY4.3– million; unknown/declined to answer)).19 Health-related status included smoking status (never, past, current),20 alcohol use (never, past, current)20 and presence of physical and psychiatric comorbidities. Physical comorbidities of interest included those at high risk of severe COVID-19, death and delay in disease care due to the pandemic (hypertension, diabetes, asthma, chronic obstructive pulmonary disease, stroke, ischaemic heart disease and cancer).21–24 Psychiatric comorbidities were depression and other psychiatric disorder,25 based on questionnaire responses (online supplemental method S1). Working hours per week (–39, 40–59 and 60–) were included as a work-related factor.19 26 Furthermore, industry-specific variables were assessed. In HCWs, we included types of healthcare professionals (doctor, nurse, pharmacist, others),6 and the experience of working on COVID-19 frontline (yes, no).27 Experience of working on frontline was defined as close contact with patients positive for COVID-19, such as providing care, examining tests and operating, based on the questionnaire. In the general working population, we included working industries (15 industries except healthcare) as an industry-specific variable. The questionnaires and response options are developed for this survey and shown in online supplemental method S1.
Supplemental material
Outcome variable
The outcome of interest was the prevalence of burnout among HCWs and the general working population. We used the Mini-Z Single-Item Burnout Scale (MZSIB), which is a burnout screening tool.28 A score of 3 or higher on the MZSIB was defined as burnout.28 MZSIB has been established crosswalks from the Maslach Burnout Inventory (MBI), which is a gold standard in burnout assessment; its reliability and validity in Japanese have been confirmed.28 29 Although MZSIB has been developed for physicians, it enquires about non-specific, self-reported stress and burnout symptoms and has been used with other healthcare professionals and non-HCWs, such as librarians.30 We obtained permission to use the Japanese version of MZSIB from the translators before the survey. The questionnaires and response options are shown in online supplemental method S1.
Statistical analyses
First, baseline characteristics of HCWs and the general working population were noted. Second, we estimated the distribution of MZSIB scores and the prevalence of burnout in each industry. Lastly, using modified Poisson regression analysis, we estimated the prevalence ratios (PRs) and CIs to identify the associated factors of burnout. Because a previous study reported that burnout among HCWs during the COVID-19 pandemic was approximately 30%, we assumed that burnout was not rare among the respondents of this study.6 31 Therefore, we applied not logistic regression models but modified Poisson models for reliable and valid estimations.32 To approach the estimates of the Japanese general population from the JACSIS respondents, we used an inverse probability weighting (IPW) method using propensity scores.33 Details of sampling weights are shown in online supplemental method S2. We adjusted for the differences between the internet survey respondents and the general public in Japan.
All CIs and p values were based on the robust variance estimator to account for IPW. Statistical significance was set at p<0.05. All analyses were performed using STATA V.16.1 (StataCorp, College Station, Texas, USA) and SPSS V.19.0 (IBM).
Patient and public involvement
This study involved neither patients nor the public about the research question. This study did not invite any patients to comment on the study design, interpretation of the results, or the readability or accuracy of this document.
Results
Characteristics of respondents
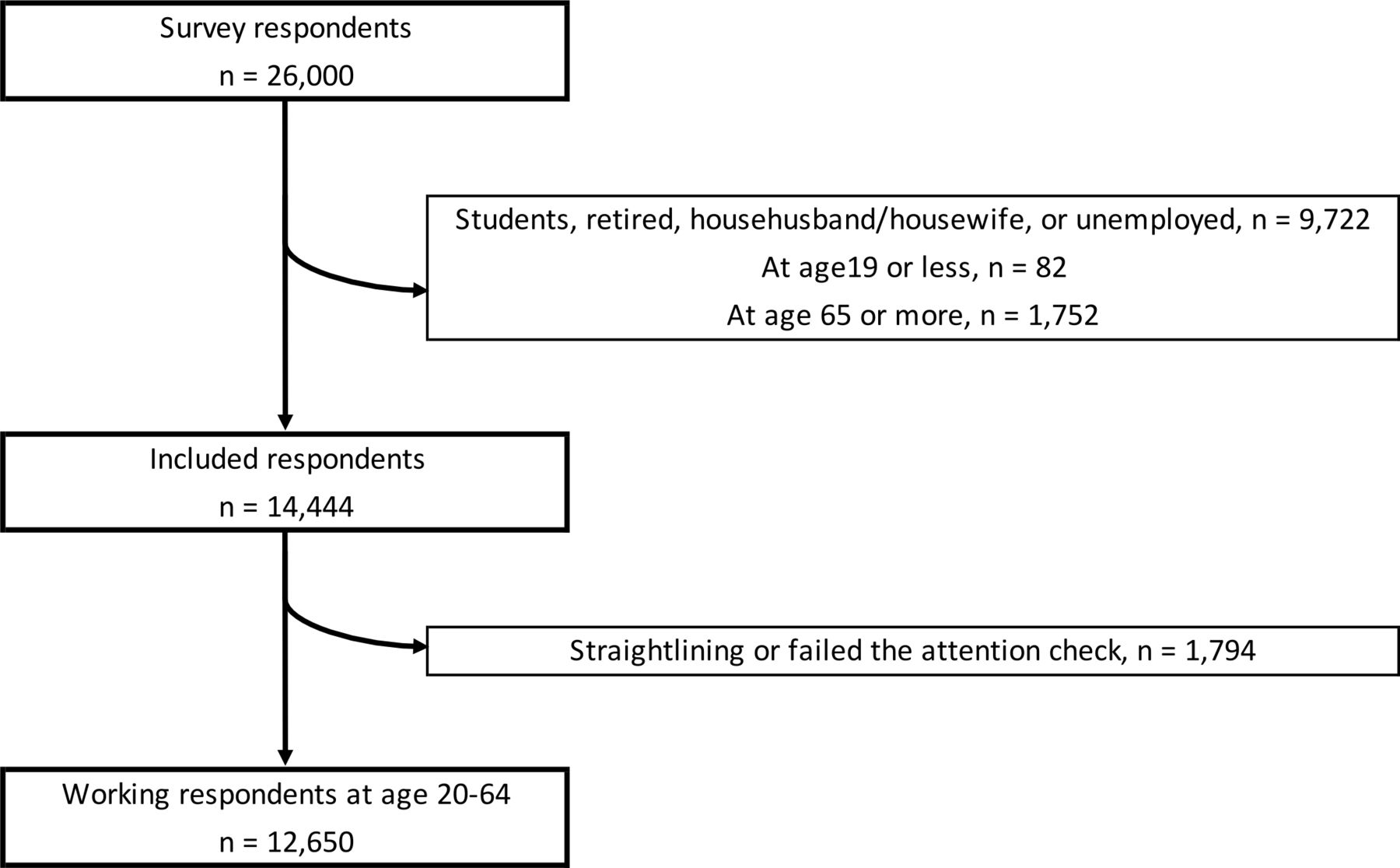
Of the 14 444 workers, we excluded 1794 who met the exclusion criteria (figure 1). Of the included 12 650 workers, 1087 (8.6%) were HCWs. Overall, 39.6% were female, 29.8% were in the 40–49 years age group, 63.9% were married, 46.7% had college or higher education and 58.6% were regular employees (table 1). Compared with the general working population, HCWs were likely to be female, young, regular employees, with higher education and higher income levels. Moreover, HCWs were less likely to be smoking, using alcohol, having physical or psychiatric comorbidities and working 60 hours/week or more (table 1).
Baseline characteristics of respondents

Flow diagram of this study.
Among HCWs, 9.2% were working on the COVID-19 frontline and 23.9% were nurses, whereas in the general working population, 22.0% were working on manufacturing (online supplemental table S1).
Prevalence of burnout
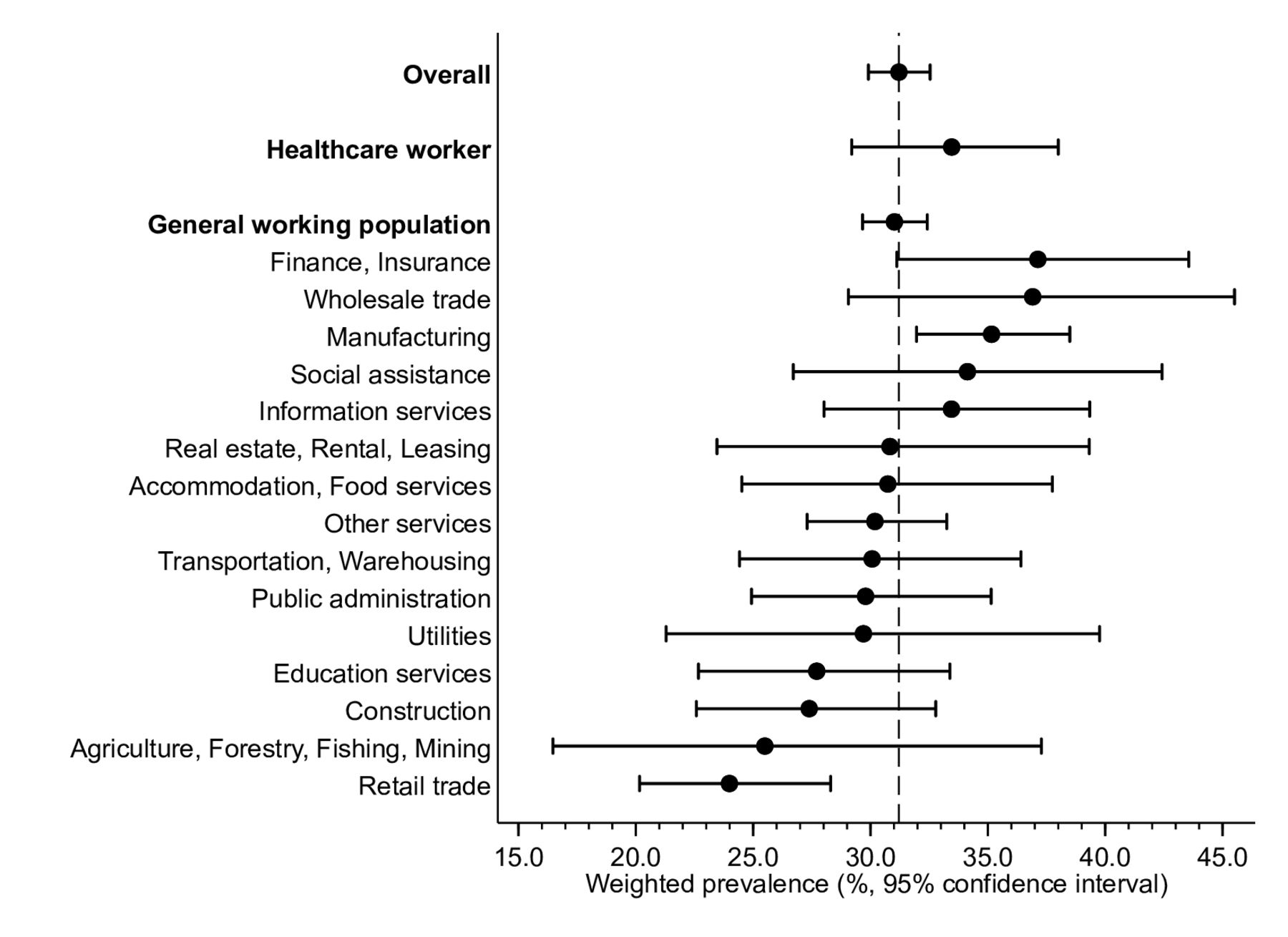
Burnout was prevalent in 31.2% of the overall sample, with 33.5% and 31.0% among HCWs and the general working population, respectively (figure 2, online supplemental table S2). Among the general working population, ‘finance, insurance’ and ‘wholesale trade’ industries had high proportions of workers with burnout (37.1% and 36.9%, respectively), whereas ‘retail trade’ and ‘agriculture, forestry, fishing, mining’ showed low proportions of workers with burnout (24.0% and 25.5%, respectively).

{kind=link}
{kind=link}
Weighted prevalence of burnout in healthcare workers and the general working population.
Distribution of MZSIB scores
When focusing on each score of MZSIB, the distributions among HCWs and the general working population were similarly right skewed (online supplemental figure S1).
Factors associated with burnout among HCWs and the general working population
The multivariable model showed that among HCWs, being widowed/separated was associated with burnout (PR 1.69, 95% CI 1.16 to 2.46; p=0.01). In contrast, among the general working population, presence of physical or psychiatric comorbidities (PR 1.14, 95% CI 1.03 to 1.28; p=0.01; and PR 1.65, 95% CI 1.45 to 1.87; p<0.001, respectively) was associated with burnout (table 2).
Results from multivariable modified Poisson regression analysis
A significant association between working 60 hours or more per week and burnout was observed in both HCWs and the general working population (PR 2.52, 95% CI 1.69 to 3.76; p<0.001; and PR 1.26, 95% CI 1.07 to 1.48; p=0.01, respectively).
Discussion
Using a large-scale internet survey that included more than 12 000 workers in Japan, we clarified the prevalence of burnout and its associated factors among HCWs and the general working population. The prevalence of burnout among HCWs and the general working population was approximately 33.5% and 31.2%, respectively. In the general working population, the prevalence of burnout varied according to industry; burnout was observed in more than 35.0% of the workers in ‘finance, insurance’, ‘wholesale trade’ and ‘manufacturing’, whereas it was seen among less than 27.5% of those in ‘construction’ and ‘agriculture, forestry, fishing, mining’. We identified both common and specific associated factors of burnout among HCWs and the general population. For example, long working hours, which is a known indicator of burnout,19 were associated with burnout in both HCWs and the general working population; however, for marital status, an association with burnout was observed in HCWs but not in the general working population. In contrast, individual comorbidities, a statistically significant indicator of burnout in the general working population, were not associated with burnout in HCWs. Our findings imply that there may be differences in the aetiology of burnout between HCWs and the general working population, thus highlighting the importance of targeted and tailored intervention for burnout prevention.
There are several potential mechanisms that may explain our results. First, burnout in the general working population was similarly observed as among HCWs. As noted above, general workers as well as HCWs have struggled with insufficient protective equipment against COVID-19.7 In addition to COVID-19-related stressors in the working environment, economic downturn impacted workers’ income.34 Such socioeconomic changes may account for the high prevalence of burnout in the general population. Second, among the general working population, the high prevalence of burnout in the ‘finance, insurance’, ‘wholesale trade’ and ‘manufacturing’ industries was noteworthy. This may be explained by the impact of the pandemic on the economy. Due to the COVID-19 pandemic and subsequent shutdowns worldwide, financial markets have been exposed to substantial stress and volatility.35 Workers in financial industries, such as bankers, had to fulfil their duties even during the pandemic to keep the economy afloat.36 Such difficulties may negatively impact them. Moreover, the financial distress from the pandemic has negatively affected households, communities and small businesses, such as manufacturing and wholesale.35 Individuals working in these industries have also faced difficulties in maintaining a steady flow of required services due to the economic downturn.37 The occupational stress caused by the pandemic may render workers in these industries vulnerable to burnout.
In terms of the risk factors, we can also speculate some common and specific mechanistic explanations for HCWs and the general working population. A study showed that HCWs have not sufficiently coped with occupational stress, such as hopelessness, sadness or frustration during the COVID-19 pandemic.38 Furthermore, poor work-life integration (WLI), characterised by conflicts of career and personal responsibilities, is responsible for burnout,39 and may have become evident during the pandemic among HCWs. Factors associated with burnout identified in this study, such as being single and working long hours, are risk factors for both job stress and poor WLI,38 39 and might have strongly contributed to burnout during the pandemic. Of the general working population, individual health concerns may have strongly influenced the occurrence of burnout. Worker’s physical and mental health concerns are known predictors of burnout.40 As the COVID-19 pandemic has impacted healthcare systems, and delays in doctor consultation have been widely reported,41 workers with comorbidities may have experienced increased worry about their health conditions and consultation delay, leading to fear of COVID-19 and subsequent burnout.
Evidence focused on differences in the prevalence and associated factors across the occupational industries during the COVID-19 pandemic is scarce. Before the pandemic, Shanafelt et al explored the prevalence of burnout among physicians and other workers in the USA.9 In their study, physicians had a higher likelihood of burnout than general employees (37.9% vs 27.8%). Additionally, they found that longer working hours and higher educational attainment were associated with higher risk of burnout.9 After the pandemic, numerous studies reported the prevalence of burnout. Ghahramani et al conducted a systematic review and meta-analysis of burnout among HCWs during the pandemic and reported that the pooled prevalence of burnout was as high as 52%, highlighting the heavy burden of burnout for policymakers.27 Particularly, the meta-analysis highlighted that job types (eg, physicians, nurses and other HCWs), country-level income and frontline exposure to patients with COVID-19 were crucial predictors of high prevalence of burnout. In Japan, Matsuo et al conducted a survey study that investigated burnout and its associated factors among 312 HCWs in a Japanese single hospital between 6 and 19 April 20206; the prevalence of burnout was approximately 31.4%, and notably, high prevalence of burnout was observed in HCWs other than physicians. Another study by Kuriyama et al examined the prevalence and associated factors among 214 Japanese physicians via an internet survey between 2 and 16 March 2021.42 In their study, the proportion of burnout among physicians was approximately 34.4%, and marital status (eg, being without a partner) was associated with burnout. Although these studies provide crucial information, all analyses were based on either data collected before the pandemic or heterogeneous data collected during the pandemic. Hence, evidence based on homogeneous, large-scale data during the COVID-19 pandemic was limited. To the best of our knowledge, this is the first study that examined the prevalence of burnout across job industries including both HCWs and non-HCWs, and explored the factors associated with burnout in HCWs and the general working population separately, using large-scale, nationally representative data.
Our study has limitations. First, because this study was internet based, all respondents may not be workers from Japan. Furthermore, we did not obtain each respondent’s nationality. However, to minimise the differences, we used IPW, which is commonly used in internet-based studies.43 Second, we did not include individual work-related factors, which are important to document burnout, such as resilience or work engagement.44 45 Although these factors are crucial components of organisational strategies to reduce burnout, our study focused on overall prevalence of burnout and its associated factors in Japan and included a wide range of socioeconomic and health-related factors, which are essential in the context of policymaking from current evidence. Third, we defined the outcome using MZSIB and we did not use the MBI, which is the most commonly used to diagnose burnout.5 46 Thus, we could neither evaluate other components of burnout (eg, emotional exhaustion, depersonalisation and personal accomplishment)5 nor confirm the diagnosis of burnout. However, the primary objective of our research was to clarify the prevalence of burnout across HCWs and the general working population, and MZSIB is a reliable and valid measure of screening burnout in our study setting.29 Fourth, our results are based on the situation as of February 2021 and may not have temporal and geographical external validity. To ensure generalisability, studies conducted in other time periods of the pandemic in Japan or abroad are warranted. Fifth, this study did not obtain some unmeasured but important candidate predictors for burnout, such as night shift.47 48 This study did not investigate the pandemic-specific occupational factors, such as personal protective equipment in the workplace.7 Such potential predictors should be also examined in future studies. Sixth, due to the limited sample size, we could not conduct subgroup analyses for evaluating heterogeneity for each occupation. Further large-scale studies that incorporate enough individuals of each occupation are still warranted.
In conclusion, this nationwide internet-based study found that more than 30% of HCWs and the general population experienced burnout during the COVID-19 pandemic. However, the prevalence of burnout varied across working industries; burnout was observed in more than 35.0% of workers in ‘finance, insurance’, ‘wholesale trade’ and ‘manufacturing’, compared with less than 27.5% of the workers in ‘construction’ and ‘agriculture, forestry, fishing, mining’. Although long working hours was a common associated factor, marital status in HCWs and comorbidities in the general workers were specific risk factors. Given our results, targeted intervention for HCWs and the general working population, in addition to general workplace policy for long working hours, is warranted to prevent burnout in workers.
Data availability statement
No data are available. The data used in this study are not available in a public repository because they contain personally identifiable or potentially sensitive participant information. Based on the regulations for ethical guidelines in Japan, the Institutional Review Board of the Osaka International Cancer Institute has imposed restrictions on the dissemination of the data collected in this study. All data inquiries will be channelled through TT (tabuchitak@gmail.com) to Osaka Cancer Institute Institutional Ethics Committee.
Ethics statements
Patient consent for publication
Ethics approval
Participants responded to the web-based questionnaires if they agreed to provide web-based informed consent and intended to participate in this survey. A credit point known as ‘Epoints’, which could be used for internet shopping and cash conversion, was provided to the participants as an incentive. All procedures were conducted in accordance with the ethical standards of the Declaration of Helsinki, 1975, as revised in 2013. This study was approved by the Institutional Review Board of Osaka International Cancer Institute (No 20084). We followed the STROBE guideline for cross-sectional study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @TYoshioka0318, @TakahiroTabuchi
TM and TY contributed equally.
Contributors TM, TY, RO, KN and TT contributed to the conceptualisation of this study. TY, RO and TT collected the data. TY, TM, RO and TT developed the plan for analysis. TM and TY analysed the data and wrote the original manuscript. RO, KN and TT reviewed, interpreted, critically appraised and revised the original manuscript. TM, TY, RO, KN and TT reviewed the final version of the manuscript and approved its submission. TM and TY take responsibility for the content of the manuscript, including the data and analysis. TY accepts full responsibility for overall contents of this study as guarantor, has access to the data, and controlled the decision to publish.
Funding The JACSIS study was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI grants (grant numbers: 17H03589, 19K10671, 19K10446, 18H03107, 18H03062, 19H03860), the JSPS Grant-in-Aid for Young Scientists (grant number: 19K19439), the Research Support Program to Apply the Wisdom of the University to tackle COVID-19 Related Emergency Problems, University of Tsukuba and Health Labour Sciences Research Grant (grant numbers: 19FA1005, 19FG2001, 19FA1012) and the Japan Agency for Medical Research and Development (AMED; grant number: 2033648). The authors acknowledge the National Institute of Public Health for the support of article publishing charge.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.