Article Text

Abstract
Introduction Starting dialysis not only has a major impact on the life of patients but also on their informal caregivers. Previous research shows greater burden and lower quality of life among caregivers of dialysis patients compared with the general population. Unfortunately, the evidence on the course of both positive and negative experience in caregivers of incident dialysis patients is scarce. Furthermore, well-designed, prospective, multicentre studies comparing caregiving of home dialysis patients with in-centre dialysis patients are lacking. This paper proposes a protocol to assess the trajectory of experiences (both positive and negative) and quality of life of caregivers of home dialysis patients compared with caregivers of in-centre dialysis patients.
Methods and analysis This paper presents a protocol for a prospective, observational, multicentre cohort study which extends the ongoing Dutch nOcturnal and hoME dialysis Study To Improve Clinical Outcomes (DOMESTICO). This study will include at least 200 adult caregivers of patients who start dialysis therapy and have been included in the DOMESTICO study. Positive experiences of the caregivers will be the primary outcome parameter of this study, and negative experiences and health-related quality of life the secondary outcome parameters. Required support will be investigated as an exploratory finding. Outcome parameters will be assessed at baseline, and at 6 and 12 months after start of dialysis using validated questionnaires.
Ethics and dissemination Ethical approval for this study has been obtained from the Medical Research Ethics Committee of the Amsterdam University Medical Centre. The results of this study will be disseminated by publication in a peer-reviewed journal and through presentations at conferences and seminars.
- Dialysis
- End stage renal failure
- MENTAL HEALTH
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study examines and compares both burden and positive experiences among caregivers of home dialysis versus caregivers of in-centre dialysis patients.
The intended sample size of this is study is large compared with other studies involving caregiver experience of dialysis patients.
The inclusion of caregivers for this study is linked to the inclusion of patients in a nationwide, prospective, observational cohort study comparing clinical outcomes of home dialysis to in-centre dialysis.
As for any study using self-administrated questionnaires, non-responding could lead to incomplete results.
Introduction
Dialysis is a form of kidney function replacement therapy for patients with end-stage kidney disease (ESKD). It can be performed in a dialysis centre (ie, in-centre haemodialysis (HD)) or at home (ie, peritoneal dialysis (PD) or home HD). The mortality rate among dialysis patients is high: patients starting on dialysis have a median 5-year survival rate of only 45%.1 Observational studies comparing in-centre HD with home dialysis show comparable survival between groups.2–4 As many patients experience dialysis as a heavy burden resulting in impaired health-related quality of life (HRQoL), focus is shifting in recent years from survival towards HRQoL as the main outcome parameter. Home dialysis could result in better HRQoL because it offers more flexibility and independence. Available evidence regarding the effects of home dialysis on HRQoL compared with in-centre HD is however limited.5 Therefore, the Dutch nOcturnal and hoME dialysis Study To Improve Clinical Outcomes (DOMESTICO) was initiated. DOMESTICO is a nationwide study in incident dialysis patients aiming to compare HRQoL, clinical outcomes and cost-effectiveness of home dialysis with in-centre HD.6 Patients have been included from December 2017 onwards.
ESKD, the need to start dialysis, and the choice for a home-based treatment or a centre-based treatment does not only have an effect on patients, but also on their social environment, in particular on informal caregivers like spouses and adult children providing care to the patient. Informal caregivers are people, often family and friends, who provide care, typically unpaid, to someone with whom they have a personal relationship.7 8 In the Dutch population over 18, one out of three persons provides informal care. Of these informal caregivers, 1 out of 10 feels overburdened, in particular those who provide long-lasting intensive care.9 Signs of overburdening can be increased sick leave from work, reduced social life and health issues.10 This could lead to reduced QoL of the informal caregiver, but also of the patient.11 Moreover, it could result in PD technique failure/drop-out.12 On the other hand, caregiving can also entail positive experiences such as feelings of personal growth, joy and sense of accomplishment.13–18 In particular, residential caregivers report both high caregiver burden and positive experiences.13 19
The burden of care and QoL among caregivers of dialysis patients were recently described in a systematic review.20 It appeared that the burden of life experienced by caregivers and QoL were worse than in the general population. Depression was less common compared with the dialysis patients for whom the caregivers cared for and similar or slightly greater compared with the general population. Furthermore, the impact on caregivers while caregiving for in-centre HD patients seemed comparable to that for PD patients. However, most studies in this systematic review had a cross-sectional design, included a small number of caregivers, and had a high risk of bias. Moreover, these studies did not assess the association with patient outcomes.
It is likely that caregivers of dialysis patients also have positive experiences. However, studies investigating this are scarce. In a convenience sample of 89 caregivers of HD patients, responding to an online survey, caregivers who viewed their role positively experienced lesser degrees of burden than caregivers with a negative role perception.21 A qualitative study found that caregivers experienced personal growth that contributed to their ability to cope with the burden of caregiving.22 No studies have been conducted comparing positive experiences of caregivers of home dialysis patients and caregivers of patients treated with in-centre HD.
In order to properly inform patients with ESKD and their caregivers about the start of dialysis therapy and the choice of dialysis modality, it is important to discuss also what the caregiver can expect after the start of dialysis. Such information is also essential for reaching true shared decision-making. However, available evidence regarding the course of caregiving experiences after start of dialysis is limited. Therefore, large and well-designed, prospective, multicentre studies with sufficient follow-up are needed. The aim of this study is to assess the trajectory of the experiences (both positive and negative) and HRQoL of caregivers of patients who start home dialysis, and compare these to experiences and HRQoL of caregivers of patients who start in-centre HD. We hypothesise that (coresidential) caregivers of home dialysis patients experience more positive experiences, but also more negative experiences, and still have better HRQoL, compared with caregivers of in-centre HD patients.
Methods
Study objectives
The main objective of this study is to assess the experiences (both positive and negative) and HRQoL of caregivers of patients who start dialysis at home compared with the experiences and HRQoL of caregivers of patients who start in-centre HD. The assessments will be performed at baseline and 6 and 12 months after starting dialysis.
Moreover, we will make an inventory of the required support for caregivers in order to develop an online caregiver module. This module will be an extension of the Kidney Guide, which is a decision aid developed by the Dutch Kidney Patients Association.23
Study design
We will conduct a prospective, observational, multicentre cohort study which will be an extension of the ongoing DOMESTICO study. DOMESTICO is a nationwide study in incident dialysis patients, investigating the effects of home dialysis on HRQoL in relation to clinical outcome and costs, in comparison to in-centre HD.6 Dialysis patients are included from 54 Dutch dialysis centres (covering 98% of Dutch centres) and 4 Belgian centres. At present, 27 of participating Dutch centres and 1 Belgian centre have agreed to also recruit informal caregivers into this extension study.
Study participants
Participants are eligible for this study when they care for a partner, family member, friend or loved one with ESKD who is starting dialysis therapy and is included in the DOMESTICO study. The participant has to be 18 years or older. Caregivers are requested to provide written informed consent. If the patient has multiple informal caregivers, only the caregiver that is the most responsible person for looking after the patient during the course of the disease is included, generally a spouse or adult child.
Study enrolment
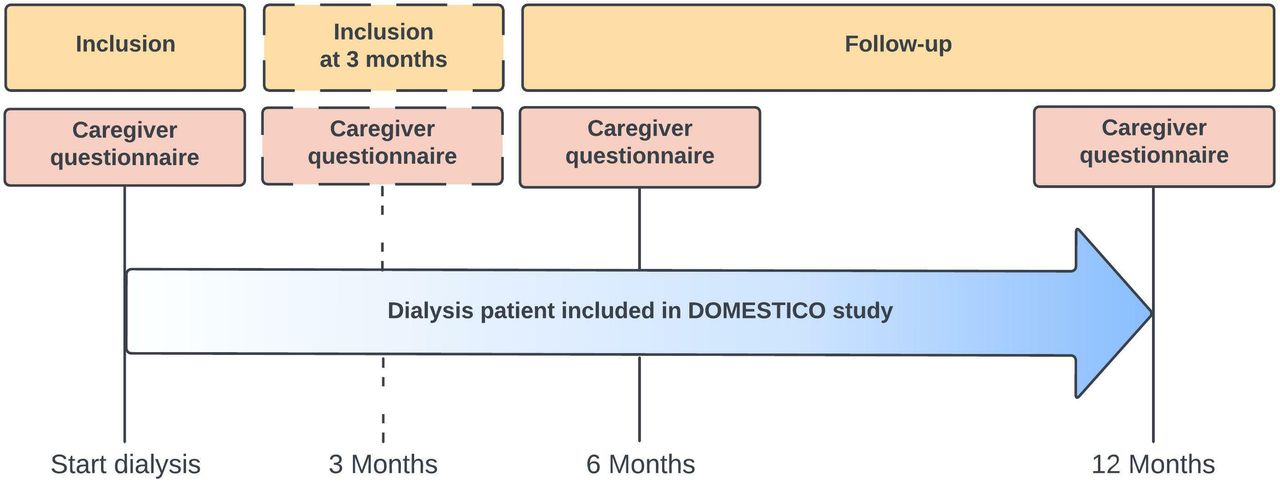
Caregivers are included in the period within 4 weeks before to 4 weeks after start of dialysis of the person they are caring for. If caregivers are missed for inclusion within this timeframe (eg, due to acute start of dialysis of the patient), there is a second opportunity for inclusion at 3 months (±2 weeks) after start of dialysis. Start of dialysis is defined as the first PD session performed at (a nursing) home (excluding PD-training) or, in case of in-centre HD, the first HD session performed in a centre (excluding continuous kidney replacement therapy).6 See figure 1 for a schematic overview of the study design.

{kind=link}
Schematic overview of the prospective, multicentre cohort study on experiences and health-related quality of life of caregivers of dialysis patients in the DOMESTICO study. Timeline shows the inclusion period for caregivers 4 weeks before start dialysis till 4 weeks after start dialysis, a second inclusion possibility at 3 months after start dialysis (±2 weeks) and the follow-up period until 12 months after start dialysis. Questionnaires are filled in by the caregivers at baseline, 6 months and 12 months. DOMESTICO, Dutch nOcturnal and hoME dialysis Study To Improve Clinical Outcomes.
Caregiver experiences and their HRQoL will be assessed by five different validated questionnaires (see table 1 and online supplemental Appendix 1). All questionnaires are available in Dutch and English, and are self-administered. Participants are asked to fill in the questionnaires after inclusion, and at 6 and 12 months after start dialysis. If participants have difficulties completing the questionnaires, they can reach out to the local investigator or the main research assistant for help. Early study termination occurs if the patient or caregiver withdraws from the study or if the patient stops dialysis treatment due to recovery of kidney function, kidney transplantation, the wish to stop dialysis or death.
Supplemental material
Overview of study endpoints
Primary endpoint
The primary endpoint is the positive experiences of the caregiver of a given patient at 12 months after start of dialysis of this patient, measured by the Positive Experiences Scale (PES) (table 1).
The PES is a Dutch 8-item validated questionnaire, which includes statements regarding joy, satisfaction, being appreciated, closeness, happiness, learning new activities and meeting new people. Caregivers score their positive experiences on a three-point Likert scale: agree (0), neutral (1) and disagree (2). Scores can range from 0 to 16. A higher sum score means fewer positive experiences. Sum scores can be divided into four categories: 0–4 points means ‘positive’, 5–8 points means ‘fairly positive’, 9–12 points means ‘somewhat positive’ and 13 point or more means ‘not positive’.19 24
Secondary endpoints
Secondary endpoints are negative experiences and HRQoL of the caregiver 12 months after start dialysis (table 1). Negative experiences of the caregiver will be measured by two questionnaires: the EDIZ+ (‘Ervaren Druk door Informele Zorg’ or Experienced Pressure by Informal Care) and the CES-D (Centre for Epidemiologic Studies Depression Scale).
The EDIZ+ is a Dutch 15-item validated questionnaire which assesses caregiver burden. Caregivers report their level of burden on a three-point Likert scale. For every statement, scores are dichotomised into burden (agree=1) and into no burden (neutral or disagree=0). Scores can range from 0 to 15. Sum scores can be divided into four categories; 0 points indicates no burden, 1–3 points indicates mild burden, 4–8 points indicates moderate burden and ≥9 points indicates overburdening.25
The CES-D investigates whether the caregiver might have a depression. It is a 20-item validated questionnaire, exploring the frequency of different types of depressive symptoms on a four-point Likert scale; rarely/never (0), sometimes (1), regularly (2) and mostly/always (3). Scores can range from 0 to 60. A CES-D score of ≥16 points is considered as a possible case of depression.26
HRQoL of the caregiver will be determined with the 12-item Short Form (SF-12) and the EuroQoL-5D-5L (EQ5D-5L). The SF-12 consists of eight domains: physical functioning, role-physical, bodily pain, general health, vitality, social function, role emotional and mental health. These domains are summarised in the Physical Component Summary (PCS) score and the Mental Component Summary (MCS) score. A healthy individual scores 50 points on a scale of 0–100, with an SD of 10 points. Higher scores of the PCS and MCS reflect better HRQoL.27
The EQ5D-5L assesses the HRQoL on the following five domains: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each domain is scored on a 5-point Likert scale, ranging from ‘no problems’ to ‘extreme problems’. The EQ5D-5L also asks a score on the current health status of the caregiver, ranging from 0 (‘worst imaginable health state’) to 100 (‘best imaginable health state’).28 29
Exploratory endpoints
In addition to the primary and secondary endpoints, required support will be investigated as an exploratory endpoint. Required support will be inventoried by a questionnaire investigating in which domains caregivers would like extra support, such as material support, psychological support, financial support, education or additional home care service.
Data collection
All study endpoints will be assessed at baseline, and at 6 and 12 months after start of dialysis. At baseline, additional demographical and personal data will be collected: gender, age, ethnical background, marital status, relation to the patient, living situation, education level, employment status, involvement in dialysis modality choice, duration, frequency and intensity of care, travelling time, involvement in assisting with home dialysis, involvement of professional caregivers and other informal caregivers, and impact on working, spare time and hobbies.
Data will be captured in case report forms using CASTOR Electronic Data Capture System. CASTOR is a cloud-based clinical data management platform. The database is developed by the DOMESTICO study group and follows the principles of Good Clinical Practice (ie, it has an audit trail, direct validation of inserted data and authorisation per form and user).30 Data will be linked to the DOMESTICO database which is hosted by Nefrovisie, the Dutch Quality Institute for Nephrology. The database will be archived for future research during a minimum of 15 years after completion of this study.
Statistical analysis
All statistical analyses will be conducted using statistical software such as SPSS (Version 28, IBM Corp. Released 2021) and Stata (Release 17, StataCorp. 2021). Baseline characteristics of the participants will be presented as mean±SD, median with IQR or as number with percentages. Differences in baseline characteristics between caregivers of home dialysis patients and caregivers of in-centre HD patients will be assessed using unpaired t-test, Mann-Whitney U test or χ2 test, where appropriate. In the analysis of the primary and quantitative secondary endpoints, caregivers of home dialysis patients will be compared with caregivers of in-centre HD patients using longitudinal linear regression, with adjustment for possible confounders. Possible confounders determined a priori are gender, age, ethnical background, marital status, relation to the patient, living situation, education level, employment status and involvement in dialysis modality choice. The p-value, effect size and 95% CIs will be reported. To deal with missing data, multiple imputation techniques will be used to impute the missing values where appropriate. The exploratory endpoint will be presented using descriptive techniques.
Sample size calculation
As studies investigating positive experiences of caregivers of dialysis are scarce and no data at all on within-caregiver correlations over time, it is not possible to provide a valid sample size calculation for the primary endpoint. In addition, Gilbertson et al recently performed a systematic review to investigate the burden of caring for dialysis patients. The authors identified 61 studies. Of these studies, 52 studies (85%) had a cross-sectional design and 58 studies (95%) enrolled less than 200 participants. Most studies (85%) had a high risk of bias due to frequent methodological flaws in sample representativeness, poor comparability between respondents and non-respondents, and poor-quality statistics.20 Therefore, we aim to include at least 200 caregivers, of which 100 caregivers of patients who start home dialysis. The results of this study might provide a basis for further studies that can subsequently estimate a proper sample size for the outcome that seems to be the most interesting.
Patient and public involvement
Patient and public involvement has occurred throughout the project with the help of the Dutch Kidney Patients Association (NVN). The NVN is actively involved in all work packages of the DOMESTICO project as member of the steering committee and as member of several project groups. The NVN is also involved in the present study. They contributed to the design of the study protocol. Study progress and study results will be discussed and shared with the NVN and spread via their website, their journal (Wisselwerking) and at national conferences for kidney patients and their caregivers. Furthermore, the results will be used to further develop a caregiver module as an extension of the decision aid the Kidney Guide (Nierwijzer.nl) of the NVN.23
Discussion
Patients with ESKD experience numerous symptoms and have a poor HRQoL. Starting dialysis impacts their HRQoL further, affecting their daily lives. It is important to realise that dialysis treatment does not only have a significant impact on daily life of patients, but also on that of their informal caregivers. In this study, we will assess the experiences (both positive and negative) and HRQoL of caregivers of patients who start dialysis at home compared with experiences and HRQoL of caregivers of patients who start in-centre HD. This nationwide cohort study, which is an extension of the ongoing DOMESTICO study, will include at least 200 caregivers. Caregivers will be followed prospectively until 12 months after start of dialysis. Their positive and negative experiences as well as their HRQoL will be assessed by using validated questionnaires.
In addition to its nationwide and prospective design and its large sample size, this study has some other unique features. While most studies focus on caregiver burden, this study focuses on the positive aspects of being an informal caregiver by choosing positive experiences as primary endpoint. We hypothesise that caregivers of home dialysis patients experience more positive experiences compared with caregivers of patients starting in-centre HD.
Of course, this study will also investigate the burden of being caregiver of a dialysis patient, enabling us to support them. Especially, the exploratory endpoints aim to identify the domains for which caregivers want more support. Therefore, this study will be conducted in close collaboration with the medical social workers of the participating centres. Medical social workers have specific expertise to help and support kidney patients and their families. They play an important role in providing information about the different treatment options and during the trajectory after starting dialysis.31 They can teach patients and caregivers how to cope with their disease and the comprehensive dialysis treatment. Their involvement in this study will allow them to have more in-depth conversations about the needs of caregivers.
Finally, inclusion of caregivers is linked to inclusion of patients in the prospective DOMESTICO study investigating the effects of home dialysis on HRQoL, clinical outcomes and costs in comparison with in-centre HD. The DOMESTICO study will include more than 1600 dialysis patients. HRQoL, the primary outcome parameter, is determined with the SF-12 and the Dialysis Symptom Index. These questionnaires were carefully selected as PROMs in Dutch nephrology care by the NVN, the Dutch Federation for Nephrology, and the department of Epidemiology of the Leiden University Medical Center.32 33 Furthermore, data regarding several clinical outcome parameters are collected, such as hospitalisation, technique failure and medication use. Combining the extensive data collection in the DOMESTICO study with this caregiver study will enable us to assess bidirectional associations between caregiver experience and patient outcomes in future studies.
In conclusion, several initiatives in many countries have been launched in recent years to overcome potential barriers for starting dialysis at home. In the Netherlands, a Taskforce Home Dialysis and the DOMESTICO project were initiated. Starting home dialysis does not only have an effect on patients, but also on their social environment, in particular on informal caregivers. More knowledge about caregiver experiences could provide better information to patients and caregivers regarding consequences of different dialysis modalities and start of dialysis therapy. Subsequently, adequate information will enhance the process of shared-decision-making. Finally, it can contribute to the development of intervention strategies to timely identify and reduce caregiver burden. This will improve HRQoL of both dialysis patients and their caregivers.
Ethics and dissemination
The DOMESTICO study is conducted according to the principles of the Declaration of Helsinki and in accordance with Medical Research Involving Human Subjects Act (WMO). Ethical approval for this extension was obtained from the Medical Research Ethics Committee of the Amsterdam University Medical Center (NL63277.029.17).
The results of this study will be published in a peer-reviewed journal and will be presented at relevant meetings, conferences and seminars. Collaborations with investigators interested in caregiver experience of dialysis patients are welcomed.
Ethics statements
Patient consent for publication
Acknowledgments
Admiraal de Ruyter Hospital, Goes (N Vrielink); Alrijne Hospital, Leiderdorp/Alphen (GBW Pronk, JEM Arkenbout); Amphia Hospital, Breda (S van der Muren, N Kats, N de Wit); Antonius Hospital, Nieuwegein (EM Veldhuizen); Canisius-Wilhelmina Hospital, Nijmegen (R Leenders, L Smits, A Verstegen); Catharina Hospital, Eindhoven (E Ponse); Deventer Hospital, Deventer (MJ de Ruiter, A Maalderink-Kornegoor); Dialysis Center Beverwijk, Beverwijk (C van den Berge); Dialysis Center Tergooi, Hilversum (E van Steensel); Diapriva Dialysis Center, Amsterdam (DA Ventura da Silva, M Jellema); Elkerliek Hospital, Helmond (M Frankx); Flevoziekenhuis, Almere (A Boonstra); Gelre Hospitals, Apeldoorn/Zutphen (J Mulderij); Groene Hart Hospital, Gouda (W de Ruijter); Haga Hospital, The Hague (LHM van Vliet); Isala Hospital, Zwolle (J van der Horst); Laurentius Hospital, Roermond (F Unal, K Bex); Maasstad Hospital, Rotterdam (B Hoekstra); Maxima Medical Center, Veldhoven (TJFM Vogels); Noordwest Ziekenhuisgroep, Alkmaar (M Grubben, I Hulsebosch); OLVG Oost, Amsterdam (PS Dubbelman, RM Smulders); OLVG West, Amsterdam (L Zwiers, EM Wisse); Radboudumc, Nijmegen (G van den Bosch); Reinier de Graaf Group, Delft (PFC Groeneweg-Peeters, MMAG Troost, EAJ Paauwe); Rijnstate Hospital, Arnhem (F Stortelder, R Krake, I Vogel); Saxenburgh Group, Hardenberg (N Janssen); Slingeland Hospital, Doetinchem (H Rouwhorst); UMC Utrecht, Utrecht (E Verweij, R Zekhuis, I Faber); VieCuri Medical Center, Venlo (N van Daal, H Vestjens); Amsterdam UMC, Amsterdam (DA Ventura da Silva, M Jellema); Bernhoven Hospital, Uden (A Sanders); ZorgSaam Zorggroep Zeeuws Vlaanderen, Terneuzen (M Geelhoedt); Jessa Hospital, Hasselt, Belgium (C van Hees, M Smets).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SV, NAG, TJFMV, JAJB, BVG, BCvJ and AA designed the protocol of the present study. SV, TSvL, ED, AJR, TJFMV, WCSK, BCvJ and AA are all involved in the conductance of the study. SV and TSvL contributed equally to this paper. All authors critically edited the manuscript and approved the final version.
Funding The extension of the DOMESTICO study is supported by a grant of the Dutch Kidney Foundation (Grant no: 21OM+003).
Disclaimer The sponsor had no role in the design and conduct of the study and no role in writing or in the decision to publish this paper.
Competing interests The DOMESTICO study is supported by grants of ZonMw, Fresenius Medical Care, Baxter Healthcare, Dirinco, Cablon Medical, AstraZeneca, Eurocept Homecare, Novartis, Vifor Pharma, and Bayer. AA has received speaker honoraria from Baxter Healthcare, Fresenius Medical Care, Cablon Medical and AstraZeneca. All other authors declare no conflict of interest.
Patient and public involvement Patients and the public were involved in the design and in the dissemination plans of this research with the help of the Dutch Kidney Patients Association (NVN). See the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.