Article Text

Abstract
Introduction Here, we provide a feasible, well-designed protocol of a randomised controlled trial for the assessment of the effects of a home-based multidisciplinary intervention on the severity of skin adverse drug reactions and health-related indicators in patients with non-small cell lung cancer (NSCLC) under epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) therapy.
Methods and analysis The study will be a two-group, parallel randomised controlled trial conducted at patients’ homes by a multidisciplinary team in Zhengzhou in Henan Province, China. Patients with NSCLC who received EGFR-TKI therapy and experienced adverse skin reactions will be randomised and receive either ordinary care or home-based multidisciplinary interventions. The intervention will be divided into an intensive stage (6 weeks) and a maintenance stage (6 weeks) with baseline and follow-up assessment. Interventions in the intensive stage will include general interventions such as health education, follow-up, behaviour guide and social support and targeted interventions such as skill training, coping with adverse drug reaction and problem-solving. The measures that will be carried out in maintenance stage are continuous interventions consisted of an intensive intervention. The multidisciplinary team will be responsible for managing skin adverse drug reactions as required at patients’ homes. Data collection and analysis will be performed by researchers at baseline, the end of the sixth week of intervention and the third month after the intervention. The primary outcome is the degree of skin adverse drug reactions, while the secondary outcomes, for example, self-management ability, quality of life, outpatient visits and health economics indicators, will also be presented.
Ethics and dissemination This study was reviewed and approved by the Ethics Committee of Zhengzhou University (No. ZZUIRB-2020-97). Findings will be available to patients, clinicians, nurses, pharmacists, community medical staff, funders and health policymakers through peer-reviewed publications, social media and patient support groups.
Trial registration number Chinese Clinical Trials Registry (ChiCTR2000040643).
- CLINICAL PHARMACOLOGY
- COMPLEMENTARY MEDICINE
- DERMATOLOGY
- ONCOLOGY
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is a randomised controlled trial to evaluate the efficacy of home-based multidisciplinary interventions.
This study compares home-based multidisciplinary approaches with usual continuous care in managing skin adverse drug reactions in epidermal growth factor receptor tyrosine kinase inhibitor-treated patients with lung cancer.
This is a single-centre study, thus, the findings cannot be directly generalised to other treatment settings. Second, potential bias will exist because blinding interventionists will not be possible.
The long-term effects of the intervention are not to be tracked.
Introduction
Lung cancer is one of the leading causes of cancer-related death, accounting for a quarter of total cancer deaths. Globally, there were 2.22 million new lung cancer cases and 1.55 million lung cancer-related deaths in 2019, while the corresponding data reached 787 000 and 631 000 in China in 2015.1 2 Among various types of lung cancers, non-small cell lung cancer (NSCLC) represents 85% of the total cases in China.3 4 Significantly, 75% of patients with NSCLC were in advanced stages when they were diagnosed, with a 5-year survival rate of approximately 15%.5 As a result, NSCLC-related theranostics and clinical care have gained great attention in recent years.
The rapid development in molecular biology has enabled the identification of molecular targets of particular cancer cells, thus providing a framework for targeted anticancer therapies.6 7 Several studies have shown that targeted therapies could improve the overall survival, progression-free survival and response rate of patients with cancer, and contribute to better tolerance and quality of life (QoL).8 9 Among various types of targeted therapies, epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) have been particularly emphasised for NSCLC treatment. As suggested by the National Comprehensive Cancer Network guidelines, EGFR-TKIs could be used as the standard first-line treatment for patients with EGFR mutation-positive NSCLC,10 which represent more than 50% of patients with NSCLC in the Asia-Pacific region.11 Partly because of its oral administration, EGFR-TKIs have gained increasing popularity in recent years.12
Although the incidence of lethal adverse reactions to targeted therapy is lower than that of chemotherapy, due to the prolonged treatment time, an up to 80% adverse reaction incidence has been reported.13 Skin adverse drug reactions (ADRs) are the most common ADRs for EGFR-TKI therapy, represented by acneiform eruptions (even papule pustular rash), pruritus, dryness of skin, periungual inflammation (paronychia and nail loss), hair changes and hypersensitivity.12 As recorded by a recent investigation, approximately 80% of patients who received EGFR-TKI treatment showed skin ADRs within 3 months.14 15
Severe skin ADRs can harm patients both physically and psychologically. For example, the symptoms caused by skin ADRs could disturb patients’ sleep and detrimentally affect their self-esteem, resulting in various social participation disorders.16–19 Even worse, it was reported that the medication adherence of patients receiving EGFR-TKI-based targeted therapy was poor; approximately 32% of patients with NSCLC under EGFR-TKI treatment quit treatment due to skin toxicity reactions, which compromised the treatment effects.20 21
Overall, it is imperative to minimise severe skin ADRs of targeted cancer therapy for improved anticancer management. The primary purpose of ADR control is to avoid patients from unnecessary reduction or discontinuation of treatments. Several clinical interventions, including both pharmacological and non-pharmacological interventions, have been identified as effective ADR management approaches for targeted cancer therapy. Non-pharmacological strategies such as health education, monitoring, evaluation, recording, follow-up of ADRs and risk management were likely to generate positive outcomes because of the improvement in patients’ perception and self-management.22 23 Brunot et al implemented a nurse-led education project to manage ADRs of targeted treatment. The results showed that patients who received health education could correctly identify ADRs in time, reducing the reduction or withdrawal of targeted treatment caused by ADRs. However, it was also found that with this method, the occurrence and severity of ADRs were not decreased.24 As a result, the effect of this nurse-led education intervention in improving patients’ ADRs is unsatisfactory. Zhao et al25 developed a nurse-led drug management strategy to improve the QoL of patients with advanced renal cancer under targeted therapy. The intervention involved medication compliance management, follow-up management, and psychological and nutritional treatment. The results showed that this intervention could improve the self-management of skin ADRs and effectively reduce the severity of ADRs.20 However, the long-term benefits of this intervention were limited; in some cases, the compliance of the intervention was poor.
There are remarkable differences in skin ADRs among different patients, in terms of physical/psychological status and compliance of cooperation26; thus, it is necessary to provide not only comprehensive but also personalised interventions. To this end, a multidisciplinary skin management team consisting of medical staff of different professional backgrounds is needed. Indeed, compared with nurse-led interventions, a multidisciplinary intervention can provide comprehensive treatment, consultation and high-quality care for patients through complementary knowledge and skills, which ensure the rationality and scientificity of the intervention.27
To our knowledge, this study is the first home-based multidisciplinary intervention designed for skin ADR management, focusing mainly on self-management, QoL and outpatient visits of patients with cancer under targeted EGFR-TKI therapy. A home-based intervention can not only meet the psychosocial needs of patients, importantly, it allows continuous intervention which can promote patients’ recovery and reduce the rehospitalisation rate and cost. Besides, a home-based intervention enables to provide the management of healthcare providers and to promote the self-management of discharged patients at the same time, which ensure the continuity and professionalism of healthcare services.
Methods
Aims
This study aims to determine whether a home-based multidisciplinary intervention for patients with NSCLC undergoing targeted EGFR-TKI therapy could (1) improve skin ADRs and health-related indicators compared with patients receiving ordinary care; and (2) reduce outpatient visits and improve health economics.
Design
A prospective 12-week single-centre randomised controlled study will be conducted by a multidisciplinary team (MDT). It will be a two-group, parallel randomised controlled trial (RCT) with a pretest and follow-up. Patients with NSCLC who received EGFR-TKI therapy and experienced adverse skin reactions will be randomised to receive either ordinary care or home-based multidisciplinary interventions. The intervention will be divided into an intensive stage for 6 weeks and a maintenance stage for 6 weeks with a pretest and follow-up. The participants in the intervention group will receive home-based multidisciplinary comprehensive measures and usual care, while the control group will receive only usual cancer care under the guideline of ADR management of targeted therapy. This protocol complied with the Standard Protocol Items: Recommendations for Interventional Trials guidelines, which are recommended for clinical trials.
Participants and setting
Patients with NSCLC undergoing EGFR-TKI treatment will be recruited from a comprehensive hospital in Henan, China. Convenience sampling will be used. The inclusion criteria will include the following: (1) the pathological diagnosis was NSCLC; (2) patients with EGFR-positive advanced NSCLC; (3) patients had been on EGFR-TKI (including erlotinib, gefitinib, ektinib, afatinib, dactinib, ositinib, ametinib) treatment for at least 4 weeks; (4) patients received EGFR-TKI-targeted anticancer therapy at home; (5) patients with skin ADRs (skin ADRs were identified based on the coexistence of the adverse symptoms upon EGFR-TKI treatment, in other words, the symptoms of skin ADRs appeared with the application of EGFR-TKI treatment and decreased or disappeared when EGFR-TKI treatment was reduced or stopped); (6) patients’ cognitive function is normal, and the patient could communicate normally; (7) the residences are within 20 km from the hospital and (8) informed consent of patients. The exclusion criteria will be as follows: (1) the patients are unaware of their disease conditions; (2) patients with poor physical function with difficulty completing the research; (3) skin ADRs caused by other reasons; (4) unable to complete the questionnaire independently or with the assistance of investigators; (5) patients involved in other skin adverse reaction management studies.
This study will be conducted at patients’ homes by an MDT from a comprehensive hospital in Henan, China. The hospital is affiliated with a medical university with the largest cancer centre in Henan Province. It receives approximately 100 new patients with NSCLC with targeted EGFR-TKI therapy every year, and currently, most of the patients have access to home services.
Sample size
The sample size was calculated by G power software, which required certain criteria, such as effect size, power and significance level.28 The effect size (0.67) of a study that examined the effectiveness of a multidisciplinary intervention on medication adherence among American patients with heart failure was used.29 The sample size was calculated to be 100 in total with 50 in one group, with an effect size of 0.67, a significance level of 0.05 and a power of 0.8. To account for a rounded-up attrition rate of 10% in the study,30 the total sample size was determined to be 56 in one group.
Recruitment
Participants will be recruited through face-to-face conversations by nurses before discharge or by telephone follow-up after discharge. Eligible participants will be given a paper or electronic participant information list that consists of a brief description of the study and consent form. Participants who are interested in participating in the study will return the signed consent form to the researcher directly or through the internet. After signing the consent form, participants will be randomly divided into the indicated groups.
MDT members will be made aware of the study by email by the director of the study, and information sessions will be held to explain staff roles in detail. The director will guide and supervise all team members to follow recruitment criteria and participate in the evaluation of the recruitment phase. Managing the design and recruitment components of the study in this way will increase the enthusiasm and cooperation of participants. The study flow chart is shown in figure 1 (the flow chart of study process of participants in the RCT).
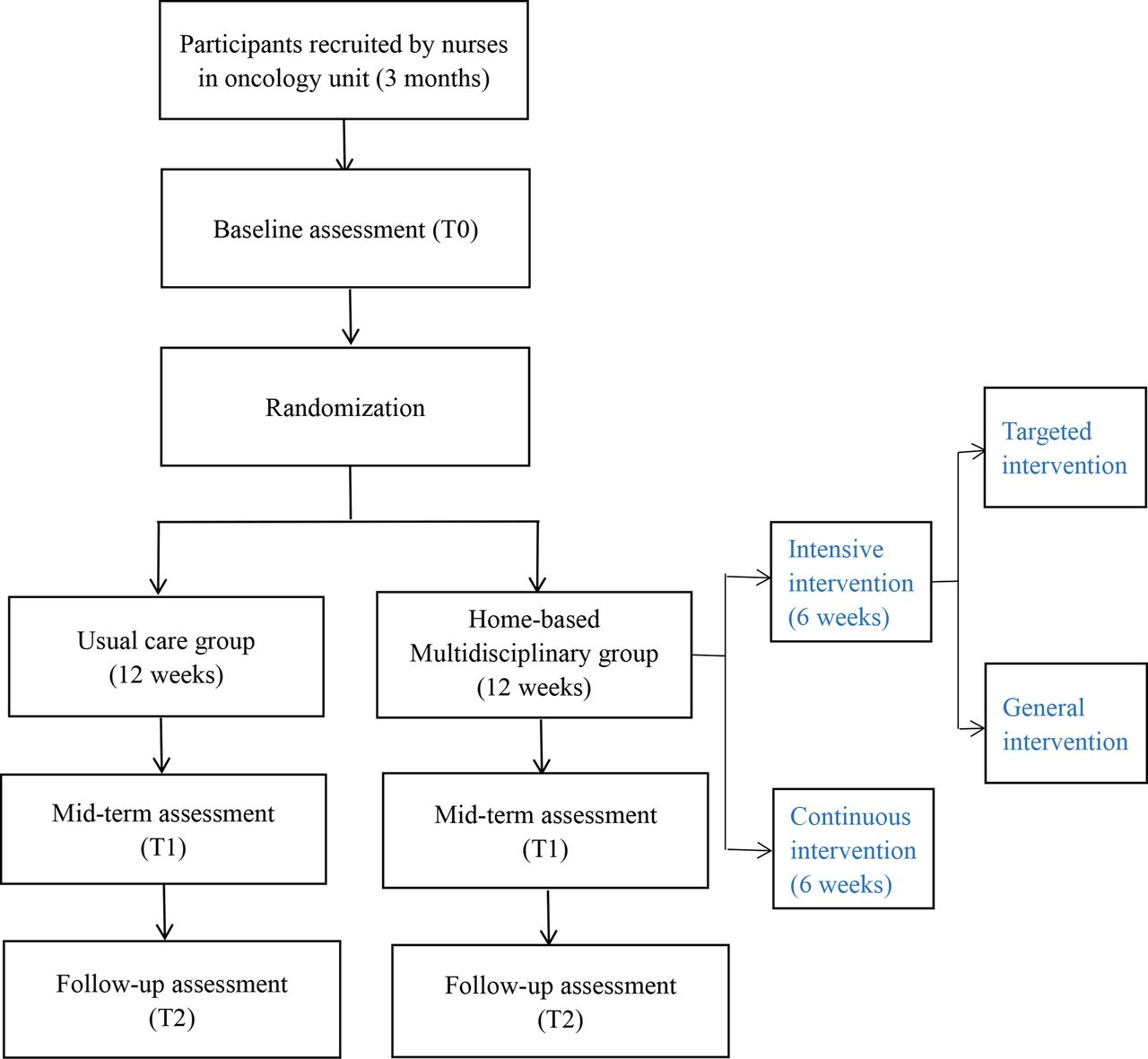
The flow chart of study process of participants in the RCT. T0: before the intervention; T1: 6 weeks after the intervention; T2: 3 months after the intervention. RCT, randomised controlled trial.
Randomisation
During the 3-month recruitment period, we aim to recruit 112 participants who meet the inclusion criteria. Participants will be randomised to either the intervention group or to the usual care group, and they will receive identifiers according to the order of inclusion. We will apply the random number table to divide 112 participants into two groups at a ratio of 1:1. Starting from the number in the second row and the fourth column of the random number table, we draw numbers from left to right, read 112 double-digit random numbers and sort them by number. If the extracted random numbers are the same, they will be sorted according to the sequence, and the first number will be set as small. The participants with numbers 01–56 will be in the control group, and those with numbers 57–112 will be assigned to the intervention group. The randomisation procedure will be performed by an independent statistician who does not know the study details. Only the statistician knows the random sequence that will be concealed to other researchers of this study.
Allocation concealment
Allocation concealment will be obtained using opaque and sealed envelopes. The statistician will complete the allocation assignments that are prepared before the trial and unknown to the rest of the research team.
Intervention
The intervention protocol was designed according to the practice guidelines and expert consensus on skin symptom management, targeted therapy for NSCLC and ADR management of targeted therapy for patients with cancer. Meanwhile, we followed the Health Education Prescription for Lung Cancer and the Experts’ Consensus on Multidisciplinary Care of Lung Cancer. In addition, we considered some influencing factors, such as cognition, nutrition, psychological status, self-management, health behaviour and social support, as the intervention points. Relevant concomitant care and interventions are prohibited during the trial.
Before preparing the protocol, we analysed all available literature about interventions on ADRs of anticancer therapy and concluded that, for optimal results, the most appropriate intervention period should be 6 weeks; at the same time, the compliance of intervention could be guaranteed. Considering the sustainability of the effect of the intervention, we will add a 6-week continuous intervention. Due to home-based interventions, participants are more likely to accept longer-term interventions.
Home-based multidisciplinary intervention team
Medical team: this team is composed of experts from several departments, including two oncologists, one dermatologist, one traditional Chinese medicine (TCM) doctor and one pharmacist. One nutritionist and one psychologist are also involved.
Nursing team: the nursing team is divided into professional and subprofessional teams. The members of the professional team are composed of three oncology nurses, one of whom has a master’s degree, and one head nurse of the oncology department acts as the team leader. The nurses in the subprofessional group include a nutrition specialist nurse and a follow-up nurse.
Team leader: the team leader is the head nurse of the oncology department who is responsible for organising the specific work of the MDT and monitoring the implementation of the intervention. The head nurse has intensive experience in organising, coordinating, communicating and dealing with difficulties and is familiar with the team culture and clinical decision-making procedures.
Team initiator: an authoritative expert in lung cancer clinical practice with certain skills in administrative organisation and coordination. The team initiator in this study is the director of the oncology department.
Coordinator: the coordinator is the nurse with a graduate degree in the oncology department who is responsible for arranging multidisciplinary meetings and tracking the implementation progress of each member. Moreover, the coordinator will assist the team leader in coordinating and communicating.
Roles and qualifications: all members involved in multidisciplinary intervention have both academic competence and clinical experience, and they can solve problems and make decisions independently. Roles are as follows: oncologist, oncology nurse specialist, dermatologist, TCM doctor, pharmacist, nutritionist, psychologist, instructor and research designer.
Team training
The training programme was drafted by the researchers according to the Chinese Skin ADRs Management Practice Guidelines and Experts’ Consensus of Anticancer Therapy. After fully considering the opinions of experts from various disciplines, the training courses were compiled. The dermatologists will learn first and then train other team members. The courses mainly included guideline interpretation, the effect and self-management of targeted drugs and skin ADR management, nutritional assessment and management, psychological assessment and communication skills. Additionally, members will also receive training, including shared decision-making training, teach-back methods and effective communication. At the same time, members need to master skills such as (1) how to confirm patients’ understanding of basic information and how to share and understand patients’ preferences during treatment; (2) how to cultivate the ADR management ability of patients and caregivers; (3) how to prepare and construct cases and protocols before MDT meetings.
The training will be conducted in the form of lectures, interactive seminars, case discussions, clinical practice and scenario simulation. Simulation training will be performed by retrospectively analysing the data of five patients with NSCLC treated with targeted EGFR-TKI therapy. The contents of simulation training include medication selection, communication, nutritional status assessment and dietary guidance, individualised psychological evaluation and intervention, and telephone follow-up. At the same time, team members will discuss the standard of home visits and emergency coping. The training will be carried out in the meeting room of the oncology department for 2 months, once a week, approximately 2 hours each time. After the training, the assessment will be conducted in the form of case analysis and scenario simulation and will be commented on by dermatologists.
Implementation of multidisciplinary intervention
The core elements of MDT are listed as follows:
Develop plans: multidisciplinary members formulate team management strategies, work plans (objectives, budget, job assignment, completion time limit) and performance standards, including the responsibility of each member, rules and regulations of meetings, supervision and assessment.
Resources and environment: (1) providing infrastructure including multidisciplinary meeting rooms, transportation, necessary technology and equipment; (2) administrative support including developing supportive policies and guidelines; (3) organisational support including financial support, human resource allocation and subsidies for MDT members; (4) coordinating time conflicts to ensure a fixed time to deal with MDT work without extra workload.
Patient centred: (1) considering patients’ comorbidity and disease progression; (2) encouraging patients to participate in skin ADR management; (3) incorporating patients’ views and preferences; (4) increasing discussions between patients and MDT members; and (5) satisfying patients’ psychosocial needs.
Team leadership: (1) encouraging open communication and discussion to ensure equal participation; (2) considering opinions from all disciplines to resolve differences; (3) assigning team members to chair the MDT meeting in turn; (4) tracking, supervising and summarising teamwork and problem-solving; and (5) providing feedback.
Ensuring team attendance and enthusiasm: (1) emphasising cooperation and maintaining a good atmosphere; (2) proposing incentive policies such as providing opportunities for personal development and promotion for MDT members; (3) emphasising nurses’ voice and (4) teleconferencing.
MDT meeting: (1) preparation stage: the coordinator and oncologists will prepare the MDT outpatient meeting room for 1~2 hours each time once a week, and the coordinator will prepare the meeting place and time and inform all participants; (2) discussion: determining the meeting objectives, displaying the patient’s cases and then discussing the problems to be solved, the progress of intervention and solving different opinions; (3) decision-making: the final draft of the management plan formed after discussion should include exact opinions and executable measures; (4) tracking: tracking, monitoring and evaluating the progress of the intervention to revise the protocol and patients’ follow-up; (5) feedback: increasing online discussion between patients and MDT members to get feedback from patients and their families; (6) summary and improvement: all members will participate to discuss and summarise the effectiveness, problems and deficiencies of intervention, and propose improvement suggestions.
The intervention is divided into two stages: intensive intervention (6 weeks) containing general intervention and targeted intervention and continuous intervention (6 weeks). The protocols adopt different strategies such as health education, follow-up, symptom management, behaviour guidance, nutritional treatment, psychological counselling, providing social support and encouraging communication.
General intervention
All participants in the intervention group received usual care. Based on usual care, the researchers will introduce the main contents of the intervention and provide the intervention instruction manual to the participants. A nurse of MDT establishes an electronic file for each participant and builds a WeChat group (online interactive platform) including all participants and MDT members. One week after discharge from the hospital, the MDT visits patients’ homes to make a preliminary assessment and develops initial goals and plans.
In the second week, dermatologists and nurses will teach participants to cope with skin ADRs by providing specific measures such as skin protection and medication. Oncologists and pharmacists adjust patients’ medication strategies when necessary, and the nurse is responsible for arranging the referral of participants in time. The next week, oncologists, dermatologists, pharmacists, TCM doctors and nurses will carry out health education to improve patients’ cognition, beliefs and behaviour. Health education is carried out through written manuals, videos, pictures and live courses on the Tencent learning platform. After education, an online test will be conducted to check if the participants have understood. In addition to education, a nurse guides participants and their families to use an electronic record table to monitor skin ADRs continuously and dynamically. These records will be sent to nurses through WeChat; at the same time, the MDT will discuss and solve problems asked by participants through the WeChat interactive platform. Subsequently, the nurses will organise an online meeting to communicate and to share experiences among patients to improve participants’ motivation to manage skin ADRs. At this stage, available social resources and assistance information are provided to participants. In the fourth week, intensive health education programmes are held by dermatologists and nurses to consolidate the knowledge and skills of participants in skin ADR management. Participants are tested by the teach-back method. In the following 2 weeks, behaviour guides, effective communication and problem-solving were developed by the MDT to overcome difficulties. During the whole process, oncologists and nurses inform participants to contact the team immediately when emergency conditions occur. Nurses and psychologists are concerned about participants’ psychological status, and participants are encouraged to express their expectations and emotions and receive psychological counselling. The telephone follow-up will be conducted by a nurse once a week, and the nurse will evaluate and record patients’ medication situation and skin ADRs. For the participants who have problems, the nurse will help them or inform other team members to visit home if necessary. Except for the telephone follow-up and home visit, outpatient follow-up will be implemented 1 month after targeted EGFR-TKI therapy and every 3 months later.
Targeted intervention
Targeted interventions are carried out focusing on the evaluation, prevention, controlling of severe skin ADRs and skin management behaviour promotion. Individualised health education, psychological guidance and behavioural guidance are implemented based on personal characteristics. In this process, we adopt one-on-one communication and targeted problem-solving. The predictors of severe skin ADRs, such as old age, malnutrition, comorbidity and combined medication, will be evaluated. In the first week, skin prevention measures and protection measures are designed by dermatologists and TCM; for example, a honeysuckle decoction wet compress is used to prevent rash and avoid extreme temperature, pressure and friction to prevent hand-foot syndrome. Then, coping with severe skin ADRs is based on the mechanism of ADRs (skin treatment using antibiotics and corticosteroids), different symptoms (topical preparations to relieve symptoms and individualised drug adjustment) and influencing factors (nutrition management, reducing self-perceived burden, improving self-efficacy and improving medication literacy). In the third week, according to the patients’ different education levels, learning abilities and progress, the nurse will carry out hierarchical health education. The next week, the MDT will take measures to promote adherence to skin management behaviour (emphasising the importance of skin ADR management on medication compliance and treatment effects and helping participants perceive the benefits of skin ADR management). In the last 2 weeks, professional psychological guidance and treatment are given as needed to decrease stress and to improve self-esteem. One-on-one communication and targeted problem-solving are conducted during this period.
Continuous intervention
Continuous intervention is designed to consolidate the intensive intervention. Unresolved issues and unfinished tasks during intensive intervention are completed at this stage. More one-on-one communication and individualised guidance will be given.
The conceptual framework of this study is developed based on Omaha System Theory, Symptom Management Theory and MDT Driven Care Framework. The framework of practice includes three major components: Problem Classification Scheme (PCS), Intervention Scheme (IS) and Problem Rating Scale for Outcomes (PRSO) (see figure 2). The PCS involves problems in four fields: environment, psychosocial, physiological and health-related behaviours. The human and environmental factors included in the Symptom Management Theory correspond to the contents of the environment and psychosocial fields. Meanwhile, the health and disease factors and the symptom experience showed in Symptom Management Theory correspond to the contents of the physiological fields. The IS provides the intervention direction for the study. Because this study is a multidisciplinary intervention, the contents and strategies of intervention should be constructed according to the input factors and management process contained in the MDT Driven Care Framework. Finally, we select appropriate indicators in output outcomes in MDT Driven Care Framework to form PRSO to evaluate the effect of the intervention.

Conceptual frameworks for the home-based multidisciplinary intervention. ADR, adverse drug reaction; MDT, multidisciplinary team.
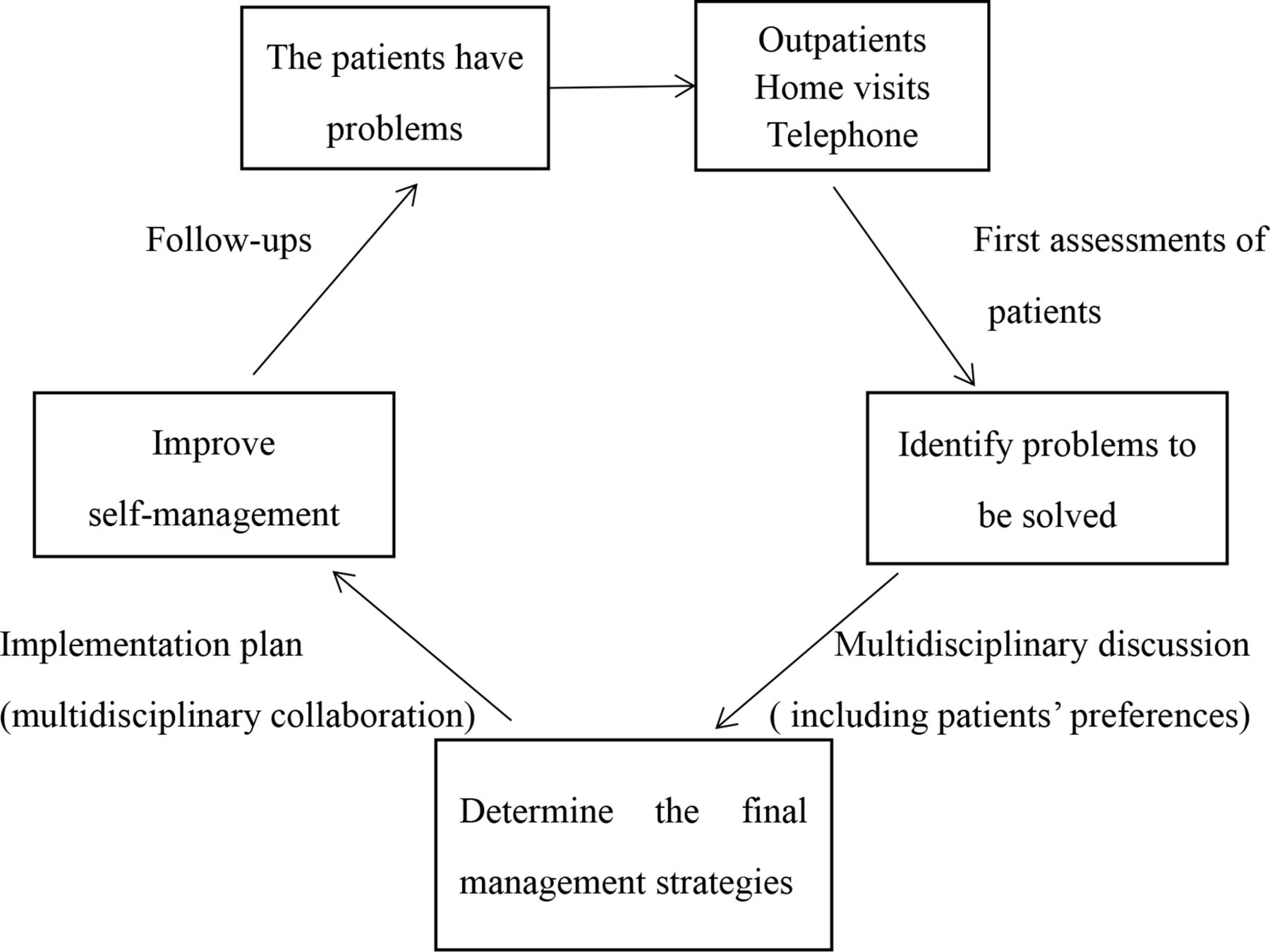
The flow chart of MDT intervention is shown in figure 3 (the flow chart of multidisciplinary intervention). The intervention will be carried out through various forms (telephone intervention, outpatient intervention, home intervention and tele-intervention), including an intensive intervention for 6 weeks, twice a week, 1–1.5 hours each time, and a continuous intervention for 6 weeks, once every 2 weeks, 1–1.5 hours each time.

{kind=link}
{kind=link}
{kind=link}
The flow chart of multidisciplinary intervention.
Adherence to the intervention
Adherence will be guaranteed by distributing intervention manuals, introducing the intervention in detail, and improving the accessibility of skin ADR management and standardised follow-up. Adherence will be measured by evaluating attendance of any form of intervention, reviewing the completion of tasks and the realisation of phased goals. In addition, whether the patients participate in the discussion and feedback is regarded as the performance of intervention compliance. Protocol non-adherence will be defined as follows: (1) failure to complete the assigned task for more than three times; (2) do not actively communicate and interact for more than 1 month; (3) failure to attend the course or group discussion more than twice on time; (4) failure to follow up more than three times; (5) no skin ADR monitoring record.
Criteria for discontinuing or modifying allocated interventions
We will discontinue the study when participants request to withdraw the study or participants’ disease worsening. We will modify intervention strategies which participants feel boring to adhere to or difficult to complete. Meanwhile, during the intervention, we will revise the intervention measures constantly according to participants’ advice or the implementation of intervention.
Intervention fidelity
The intervention fidelity will be assessed by an independent nurse who is blinded to the study using a standardised fidelity checklist.31 The fidelity checklist is composed of adherence (18 items) and competence (14 items) subscales. All items are coded ‘yes’ or ‘no’, with a comments section. The first three items on the adherence subscale reflect the basic requirements of the group and intervention. For example, receiving information and details of the intervention, this item was designed to determine knowledge gain related to the intervention to see how patients explain the outline of the intervention. Items 4–17 on the adherence subscale reflect the content of the intervention including patients’ discussion of the effectiveness of the intervention. Code ratings of competence subscales are defined from 1 (ability rarely or never acquired) to 3 (ability consistently acquired), which reflect how patients cope with skin ADRs and patients’ abilities to complete each stage of intervention.
Control group
The control group will be given continuous usual care. A continuous care group will be established to provide suitable continuous services according to patients’ disease progression and skin ADRs. Similarly, health files for patients and the WeChat group were built for consultation and follow-up. Before discharge, doctors and nurses emphasise the purpose and significance of skin ADR management and explain skin ADR prevention measures, skin symptom management and precautions, and skin ADR management manuals, including the treatment of various skin symptoms and skin protection measures, are distributed. During the patients’ stay at home, all measures will be conducted by WeChat and telephone. The pharmacist provides information on targeted EGFR-TKI therapy and strategies to cope with emergency conditions. Nurses will assist in skin assessment and help participants develop skin ADR management plans and conduct telephone follow-up every 2 weeks to track participants’ conditions, including EGFR-TKI use, skin ADR management, diet and exercise, and psychological and nutritional status. The follow-up nurse answers questions, solves problems, provides guidance and contacts other medical staff to give professional guidance and support according to the patients’ needs. In addition, health education is implemented by issuing an electronic education manual and online courses once a month and participating in lectures held by the hospital based on individualised needs. Outpatient follow-up will be arranged if necessary to evaluate the curative effect and skin ADRs.
Patient and public involvement
Patients first involved in the research when we design the intervention strategies. The researchers reviewed the electronic medical records of patients to identify potential participants, then, face-to-face conversations and telephone interviews were conducted to collect opinions and preference of patients about intervention. Several questions (for example: can you tell us specifically how you feel about skin ADRs?) were discussed to explore patients’ priorities and experience; meanwhile, patients were invited to attend multidisciplinary meeting to share decisions and participate in the development of their own management plans. After formulating the intervention plan, we need to conduct a pilot study to evaluate the intervention burden and the time spent of patients in participating in the study. According to the feedback of patients, we will modify the intervention strategies. If patients get benefits from the study, they will recommend the methods and drugs used for managing skin ADRs as well as the contact information of the MDT to other patients through WeChat patient group.
Outcomes and measurements
Primary outcome
The degree of skin ADR
The degree of skin ADR will be measured by the Common Terminology Criteria for Adverse Events version 5.0 (CTCAE 5.0). The standard classification of skin ADRs in the latest edition of the skin and subcutaneous tissue part of CTCAE 5.0 has been widely used in clinical practice and involves various ADRs of the skin.32 CTCAE 5.0 described the specific definition, performance and nature of each skin ADR and divided ADRs into five grades according to the scope of occurrence, symptoms and impact on life (whether the ADR is life-threatening), and gave the judgement criteria. According to the occurrence and the degree of ADR, skin ADRs were rated on a scale from 0 to 6 (0 indicated no skin ADR, and 5 indicated the highest severity of skin ADR). According to the impact of ADR on life and daily activities, ≤2 points was defined as non-severe ADR, >2 points as severe, for nail changes and hair loss, and >1 point as severe. In cases when the patients had multiple skin ADRs during targeted EGFR-TKI therapy, only the most serious ADRs were scored.
Secondary outcomes
Self-management ability
Self-management ability will be evaluated by the Cancer Patient Self-management Evaluation Scale developed by Cheng et al in 2017.33 The scale included six dimensions: daily life management (11 items), symptom management (7 items), emotion management (9 items), communication with medical staff (4 items), information management (3 items) and self-management efficacy (10 items). Likert 5-level scoring ranged from ‘no’ (1 point) to ‘always’ (5 points). The higher the score, the better the self-management ability of patients.
Quality of life
The Functional Assessment of Cancer Therapy-Epidermal Growth Factor Receptor Inhibitor 18 will be used to investigate QoL.34 The scale was divided into three dimensions (physiological status, social and family status, and functional status) to investigate the QoL of patients in the last 7 days. According to the impact on QoL, a 5-point Likert scale ranging from ‘no impact’ (0 points) to ‘a lot impact’ (4 points) was used. The forward items were scored 0~4 points, and the reverse items were scored 4~0 points. The total score was obtained by summing the scores of each item. The total score range was 0~72. The higher the score, the better the QoL.
Outpatient visits
Times of outpatient visits due to skin ADRs from the beginning of the intervention to the third month after the intensive intervention.
Health economics
The total cost of skin ADR management, including the cost of drugs, outpatient follow-up, hospitalisation, etc, from the beginning of the intervention to the third month after the intensive intervention.
Data collection
The data will be collected by two trained research assistants. All groups will receive a baseline face-to-face measurement using questionnaires. Post-intervention measurements will also be collected at 7 weeks of the intervention and 3 months after intensive intervention through an electronic questionnaire collection platform. All participants will receive WeChat reminders to complete the questionnaires. Participants will receive 10 renminbi (RMB) as a reward for completing each investigation during data collection. Participants who accomplish the study in both groups will also be given an extra 20 RMB. Informed consent will be obtained from eligible patients who agreed to participate in the study. Patients’ general information, skin ADRs, self-management ability and QoL will be measured at baseline (T0), the seventh week of intervention (T1) and the third month after the intensive intervention (T2). Outpatient visits and health economics will only be evaluated in the third month after the intensive intervention. Patient sociodemographic data, clinical characteristics and medication conditions will be obtained from patients’ electronic medical records.
Statistical analysis
IBM SPSS statistics V.21.0 software will be used for statistical analysis. Means and SDs will be used to describe continuous data, and frequencies and percentages will be used to describe categorical data. Differences between two groups for categorical data will be analysed with analysis of variance (ANOVA) and the Χ2 test. For continuous data conforming to a normal distribution, the t-test will examine the differences between groups at the same time points, and repeated ANOVA will be used to examine differences within group comparisons at different times. Repeated ANOVA will also be used to evaluate the trend of the index of each group at three time points and to explore the time effect, group effect and interaction of intervention. For non-normal continuous data, the Kruskal-Wallis test will be used to examine differences between groups at each time point. The reliability of the scales will be assessed by Cronbach’s α coefficient. An intention-to-treat (ITT) analysis will be used. All statistical tests used are two tailed, and p values of <0.05 are considered statistically significant.
Processing missing data
We assume that the missing data are random and independent of the constituent elements of the study. If the proportion of missing data is large and the missing data appear randomly, the mean values of the characteristics will be used to fill in the missing value. For the indicators with a small proportion of missing data, the multiple interpolation method will be used to fill the vacancy value.
Data management and confidentiality
The personal information and clinical data of all study participants are confidential. Participants will be numbered, and these numbers will be used to identify and assess participants. The participant’s identity information will be used only during the follow-up. A nurse specially assigned for safekeeping will establish the participant’s electronic information file, which will be saved in encrypted form. Only this nurse has access rights and she/he needs to insert the authorised USB with the password. These measures ensure the security of stored data.
Sensitivity analysis
Participants will be divided into two groups according to concurrent therapies such as radiotherapy, chemotherapy and immunotherapy: participants only receive targeted EGFR-TKI therapy, and participants receive concurrent therapies. Stratified analysis and sensitivity analysis will be conducted in the two groups by ITT to compare the results and explain the differences.
Data monitoring and administration
The study will be monitored by the Data Monitoring Committee (DMC) which includes two independent researchers (a participant representative and another one from the investigator team). The DMC will be responsible for monitoring scientificity, rationality, patients’ safety, recruitment and adherence of the protocol, and data quality control. The committee will meet at least 3 months per time or at any time when necessary during the study for routine review of safety data and trial progression. During the study, patients who experience any discomfort or identified with previously non-existent physical or psychological problems will also be informed and recommended to be referred to professional departments. The DMC should report its findings to the Trial Steering Committee (TSC). The TSC is an independent committee consisting of relevant experienced clinicians and researchers to ensure the study is conforming to requirements as registered. The DMC and TSC will audit trial conduct every 3 months and have access to all interim results and make the final decision to terminate the trial. The auditing process will be independent from investigators and the sponsor. No serious harm is expected as a result of the trial. However, if harm does occur, the participant will be referred to a relevant department in hospital.
Trial funding and organisation
The trial was funded by the China Postdoctoral Science Foundation in 2018 (2018M630839) and the National Natural Science Foundation of China (no. 81773175). The trial is sponsored by the College of Nursing and Health of Zhengzhou University, Henan University of Economics and Law and the First Affiliated Hospital of Zhengzhou University. This trial was registered with ClinicalTrials.gov (ChiCTR2000040643) on 12 May 2020.
Trial status
This trial was registered in the Chinese Clinical Trials Registry on 12 May 2020 with registration number ChiCTR2000040643. The trial started recruiting using protocol version 1.0 (dated May 2020) and is due to close in December 2021. The protocol was amended to version 2.0 in May 2021 after expert consultation according to the comments proposed. First, we supplemented and refined the inclusion and exclusion criteria of patients, which is more conducive to selecting more appropriate participants to relieve bias. Then, we supplemented some contents of the intervention such as health education assessment, patient group discussion and the intervention measures based on symptoms, mechanism and influencing factors formulated. Additionally, we adjusted the time of home visit, outpatient follow-up and telephone follow-up. Moreover, we further clarified the work content of each member of the MDT and how they coordinate. Last, we deleted some secondary outcomes for the following reasons: some indicators had been included in the measurement of other indicators, for example, self-management ability includes self-management efficiency, so we deleted these duplicate indicators; there are also some indicators we deleted that are more affected by cancer disease and treatment, while the intervention in this study has less impact on them such as body function, cancer metastasis and recurrence, and also, these indicators need to be tracked for a longer time. Both amendments were reviewed and approved by the sponsor and the Ethics Committee. Protocol amendments are disseminated to relevant parties by Zhengzhou University. The subjects will be recruited from January to September 2020, and the intervention will be implemented from November 2021 to May 2022. Data collection will be performed between May 2022 and August 2022, from baseline, the end of the sixth week of intervention and the third month after the intervention. Data analysis will be performed from September to December 2022. Preliminary findings are expected in March 2023.
Ethics and dissemination
This study was reviewed and approved by the Ethics Committee of our university, and permission was granted by the managers of the hospital. For participants recruited, the information list issued will state the study details clearly, and written informed consent (see online supplemental file 1) will be obtained from each of them. The results of the study will be published in peer-reviewed publications and will be presented at relevant national and international conferences. This study will provide reference and guide for healthcare professionals in designing home-based multidisciplinary interventions and ADR management of targeted therapy or other anticancer therapies. We will cooperate with the research team and patients to write a research report to disseminate research results to the patient groups, clinical staff and other research teams.
Supplemental material
Discussion
Skin ADRs are related to the prognosis and QoL of patients undergoing targeted EGFR-TKI therapy and negatively affect patients’ mental state and adherence to treatment. Severe skin ADRs can even cause patients to lose hope for treatment, resulting in discontinuation.35 At present, the Society of Oncology of Europe and America have successively issued a series of practical guidelines for skin ADR management in patients with cancer. These guidelines recommended personalised skin management and proposed preventive treatments for skin ADRs 1, 6 and 8 weeks after using targeted therapy.36 37 In 2019, the China Anti-Cancer Association constructed a practical guideline for skin ADR management adapted to Chinese culture. This provides a basis for further research on non-pharmacological interventions for skin ADRs caused by chemotherapy and targeted therapy in the future.
Studies conducted on the ADRs of targeted therapy are rare. Although some existing interventions were designed to improve ADRs, the research findings were inconsistent. A few interventions achieved satisfactory effects on reducing the incidence and severity of ADRs (reference), while some studies did not change the status of ADRs (reference). Moreover, previous studies lacked a theoretical guide, the compliance of these interventions was not high and the continuous effects were poor. Several studies have demonstrated the advantages of multidisciplinary interventions on ADR management.38–40 Previous studies indicated that a multidisciplinary intervention could ensure better anticancer treatment effects with minimal ADRs and least treatment interruption,41 and patients have better compliance with multidisciplinary management.42 The European Union Health Services Review Committee issued a guideline recommending that ‘a multidisciplinary approach’ to cancer care is needed to make the best decisions on treatment, symptom management and support for patients with cancer.27 However, few studies have focused on the application of multidisciplinary interventions for skin ADRs caused by targeted therapy. Therefore, it is important to explore an effective multidisciplinary intervention for patients with cancer with skin ADRs undergoing targeted EGFR-TKI therapy. Hence, the overall objective of this study is to design a protocol to explore the effectiveness of the multidisciplinary intervention in alleviating the severity of skin ADRs.
The research adopts a rigorous design that is guided by an appropriate theory. The study randomly divides participants into different groups, and participants’ baseline characteristics will be evaluated to report any significant differences. The validity and reliability of the instruments we used have been examined, which also affirm a rigorous study design.
Limitations
The study has some limitations. First, this is a single-centre study, and participants will be recruited from a single hospital, which compromises the generalisability of the findings. Second, blinding of interventionists will not be possible. Potential bias will exist during the assessment process due to being aware of participants’ group allocations. However, these researchers will not be involved in data collection and analysis. Last, the long-term effect of the intervention, the prognosis and the curative effect of participants are not tracked. Therefore, a multicentre prospective study with long-term follow-up will be needed.
Relevance to clinical practice
Despite the high prevalence of skin ADRs in patients with cancer undergoing targeted EGFR-TKI therapy, there is no effective intervention study to control skin ADRs. The results of the study will be of great significance to clinical practice.1 The experience gained from this study will guide the skin ADR management of patients with cancer receiving targeted therapy. The intervention will contribute to preventing severe skin ADRs and alleviating the severity of skin ADRs in patients with cancer during targeted therapy.2 This study provides an evidence-based home-based multidisciplinary intervention and assesses the feasibility and efficiency of the intervention. Then, we can recommend the application of the multidisciplinary intervention in the management of ADRs in patients with cancer, especially for patients with oral anticancer drugs at home.3 The intervention programme is also promising to improve the QoL and prognosis of patients with cancer undergoing targeted therapy.
Ethics statements
Patient consent for publication
Acknowledgments
We thank the First Affiliated Hospital of Zhengzhou University for their assistance and support. We thank the oncologists and nurses of hospital who help us to build trust relationship with patients. We thank each member of the multidisciplinary team. We thank the graduates from the college of nursing and health of Zhengzhou University. We thank professors from School of Statistics, Henan University of Economics and Law and Murdoch University for their support. We appreciate all participants for their generous participation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
RD and HY are joint first authors.
Contributors TW and CC were responsible for the quality control of the study as well as the communication with the hospital, also they contributed to the preparation of this manuscript and will contribute to the ongoing supervision of the study. RD and HY conceived the study design, contributed to the methodology and this manuscript and trained the research assistant. MAG, HZ and HY assisted with the study design and contributed to this manuscript. HY re-edited the language of the whole text to make the article more readable. LM contributed to data analysis and solving statistical problems.
Funding This work was supported by the China Postdoctoral Science Foundation in 2018 (2018M630839) and the National Natural Science Foundation of China (no. 81773175).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.