Article Text

Abstract
Objective We aimed to increase the understanding of the scaling of de-implementation strategies by identifying the determinants of the process and developing a determinant framework.
Design and methods This study has a mixed-methods design. First, we performed an integrative review to build a literature-based framework describing the determinants of the scaling of healthcare innovations and interventions. PubMed and EMBASE were searched for relevant studies from 1995 to December 2020. We systematically extracted the determinants of the scaling of interventions and developed a literature-based framework. Subsequently, this framework was discussed in four focus groups with national and international de-implementation experts. The literature-based framework was complemented by the findings of the focus group meetings and adapted for the scaling of de-implementation strategies.
Results The literature search resulted in 42 articles that discussed the determinants of the scaling of innovations and interventions. No articles described determinants specifically for de-implementation strategies. During the focus groups, all participants agreed on the relevance of the extracted determinants for the scaling of de-implementation strategies. The experts emphasised that while the determinants are relevant for various countries, the implications differ due to different contexts, cultures and histories. The analyses of the focus groups resulted in additional topics and determinants, namely, medical training, professional networks, interests of stakeholders, clinical guidelines and patients’ perspectives. The results of the focus group meetings were combined with the literature framework, which together formed the supporting the scaling of de-implementation strategies (SPREAD) framework. The SPREAD framework includes determinants from four domains: (1) scaling plan, (2) external context, (3) de-implementation strategy and (4) adopters.
Conclusions The SPREAD framework describes the determinants of the scaling of de-implementation strategies. These determinants are potential targets for various parties to facilitate the scaling of de-implementation strategies. Future research should validate these determinants of the scaling of de-implementation strategies.
- quality in health care
- change management
- health services administration & management
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
A mixed-methods approach was used to develop the framework, namely, a systematic analysis of recent literature and a subsequent critical review of de-implementation experts.
All participating experts have prior experience with the de-implementation of low-value care and a wide range of backgrounds, professions and nationalities.
The identified determinants are not empirically validated for the scaling of de-implementation strategies in this study.
Introduction
Low-value care (LVC) is either care that is not beneficial for patients or care for which the value does not offset the risk or cost given the available alternatives.1 LVC causes preventable adverse events for patients and wastes limited resources.2–4 It has been estimated that 10%–25% of healthcare spending in the USA is related to LVC.5 6 Prevalence estimations of inappropriate diagnostic testing range from 0.09% to 97.5%, indicating that the prevalence, along with the costs, highly depends on the type of care.7 Nevertheless, LVC is a pressing matter in healthcare systems and limits the capacity to provide high-value care.
LVC can be reduced through targeted strategies, also called de-implementation strategies.8 9 For example, the number of opioid prescriptions has been reduced by providing comparative feedback with persuading messaging and action planning, and the use of an electronic patient education tool has reduced the number of inappropriate upper gastrointestinal endoscopies by 61%.10 11 In another study, the number of laboratory tests was reduced by 11% in four hospitals through a combination of strategies, namely, appointing role models, data feedback, education for healthcare professionals, intensified supervision of residents and changes in the order system, among others.12 There are many more effective de-implementation strategies; a recent overview reported that 196 out of 319 strategies (61%) significantly reduced the number of inappropriate drug prescriptions, while another review showed that 11 out of 16 strategies (69%) significantly reduced the number of low-value medical tests.13 14
To substantially increase the impact of such de-implementation strategies, the effective strategies should be scaled to other organisations and healthcare providers.15 However, this rarely occurs spontaneously, and little is known about this process.16 17 This makes the scaling of these strategies challenging.
A commonly used theory is Rogers’ theory of diffusion of innovations, which is also applied in healthcare settings.18–21 Any idea, practice or object that is perceived as new can be considered an innovation.18 The theory describes the spread of innovations from innovators through early adopters, the early majority, the late majority and laggards. Factors affecting the diffusion of innovations are categorised into three main domains: perceptions of innovation, characteristics of potential adopters and contextual factors.18
It is unknown whether the determinants of scaling innovations also apply to the scaling of de-implementation strategies. The de-implementation of LVC can be considered innovative, as it aims to bring about change. However, de-implementation strategies are not equivalent to innovations. An innovation acts on a different level than a de-implementation strategy. A healthcare innovation is an (evidence-based) intervention or care practice, while an implementation strategy is the method that enhances the adoption and implementation of the intervention.22 The strategy aims to change the behaviour of healthcare professionals and/or patients. Therefore, on one hand, scaling a de-implementation strategy is seen as spreading a method that aims to reduce LVC to other organisations and healthcare professionals. On the other hand, scaling a healthcare innovation is seen as spreading a care practice, such as an additional diagnostic test or new treatment option.
In addition, healthcare innovations provide new possibilities, while de-implementation aims to discontinue the provision of a care practice.1 18 23 Consequently, de-implementation is complicated by psychological biases. People unconsciously tend to favour information that confirms their beliefs.24 This confirmation bias applies especially to de-implementation, since the process requires clinicians to abandon clinical practices they previously thought to be evidence based.24 25 The abandonment of care, even care with no additional value for the patient, could also be experienced as a loss. Therefore, loss aversion, that is, the tendency to avoid loss, affects de-implementation as well.8 In addition to these psychological aspects, there are also different barriers to de-implementation.26 For example, providing LVC can be lucrative for healthcare providers and organisations due to current financial models, such as fee-for-service payments.27 28 These differences between implementation and de-implementation result in a different focus regarding strategies.29 30
To enhance the de-implementation of LVC, several frameworks and models have been published.17 31–34 The main focus of these frameworks is either the process of de-implementation or the de-implementation strategy itself.31 35 36 However, scaling a de-implementation strategy from one organisation to another differs from the de-implementation process in one particular setting. In de-implementation, healthcare professionals identify LVC practices and target those they think are of importance. In scaling an effective strategy, the target is already fixed. Therefore, first, other individuals need to be convinced of the importance of targeting a particular LVC. In addition, they need to be convinced that the de-implementation strategy will also be effective in their organisation and that it is worth investing valuable time in doing so.18
The literature on the scaling of de-implementation strategies is very limited. One framework describes this process as the last phase in de-implementation, yet it remains unclear which factors influence the scaling of de-implementation strategies and how these factors can be targeted.17 However, there is substantial experience available in regard to scaling healthcare innovations. Therefore, we aim to use this knowledge to develop a determinant framework for the scaling of de-implementation strategies.37
Method
Study design
This study has a mixed-methods design. We performed an integrative review38 because this method allowed us to systematically extract determinants from the literature. We defined determinants as influencing factors for scaling, including both barriers and facilitators.37 First, we searched the literature for determinants of the scaling of de-implementation strategies. As these were not found, we also searched for the determinants of the scaling of healthcare innovations and interventions. We used the determinants of the scaling of healthcare innovations and interventions to build a literature-based framework. Subsequently, this framework was discussed in focus groups with de-implementation experts. The experts reviewed and adapted the framework for de-implementation strategies.
Literature-based framework
Literature search
We developed a search strategy for PubMed and EMBASE in collaboration with a medical information specialist (AT). The full strategy is described in online supplemental file 1. The search was conducted in PubMed and EMBASE for relevant literature published between January 1995 and December 2020.
Supplemental material
Data screening and extraction
After duplicate articles were removed, two authors (among RBK, DVK or DK) independently screened the titles and abstracts of the remaining articles for relevance. Articles on the scaling of innovations or interventions in healthcare in countries that are members of the Organisation for Economic Co-operation and Development (OECD) were included. We excluded conference abstracts, commentaries, articles describing quality improvement in a specific organisation, articles that were not available in English and articles that were published before 1995.
The full text of the remaining articles was screened for eligibility by one author (DVK or DK). After this screening, we noticed that determinants were rarely studied empirically. Therefore, we searched for determinants in all parts of the included articles, including the introduction and discussion. Relevant text passages were selected for further analysis if they contained information about factors or processes that influence scale-up. To reach a consensus about relevant passages, three authors (RBK, DVK and DK) independently highlighted the text passages that they considered relevant in the same five articles. Differences were discussed, and a consensus was reached among the authors. Subsequently, one author (DVK or DK) extracted the relevant fragments from the remaining included articles.
Data analysis
Qualitative analysis was performed in ATLAS.ti. One author (DK) performed conceptual labelling inductively by coding the determinants of the scaling process. A codebook was developed and continuously adapted during coding. Determinants were not coded if the definition was not clear or the association with the scaling process was not stated or demonstrated. All coded determinants were subsequently checked by another author (RBK or SAvD). In a group meeting, three authors (DK, RBK and SAvD) identified domains and subdomains, which were iteratively evaluated in two group meetings with all authors (DK, RBK, SAvD, PPTJ, GPW). None of the articles mentioned determinants of the scaling of de-implementation strategies; consequently, the literature-based framework solely discussed the determinants of the scaling of innovations and interventions.
Focus groups
We aimed to convert our literature-based framework into a determinant framework for the scaling of de-implementation strategies. Therefore, we organised online focus groups with de-implementation experts who reviewed and complemented our framework. The completed Consolidated Criteria for Reporting Qualitative Research can be found in online supplemental file 2.
Supplemental material
Participants and study procedure
Participants were purposively sampled based on their expertise in the de-implementation of LVC, their interest in the scaling of de-implementation strategies and their country of residence. Expertise was defined as having past experience in advisory capacities concerning the de-implementation of LVC or direct involvement in de-implementation projects. Eighteen participants were invited by email to take part in a digital focus group, of which 16 accepted the invitation. Two experts rejected the invitation, but both suggested another expert with a similar background who was willing to participate. In preparation for the focus group, the participants were asked to review the literature-based framework, answer questions about the relevance of the current determinants of de-implementation strategies and add any potentially missing determinants. The preparation documents can be found in online supplemental file 3. During the focus groups, the experts discussed the relevance of the identified domains and subdomains of de-implementation strategies and whether the literature-based framework lacked determinants of the scaling of de-implementation strategies. The topic guide can be found in online supplemental file 4. Data saturation was reached after four focus groups. The focus groups were conducted by DK and either RBK or SAvD.
Supplemental material
Supplemental material
Data analysis
The audio recordings were transcribed and analysed in Atlas.ti. The codebook constructed for the literature-based framework was used as the basis for the coding. The initial coding was performed by DK and checked by either RBK or SAvD. Differences were discussed in a consensus meeting with three authors (DK, RBK, SAvD), who also discussed the adaptation of the previously identified domains and subdomains. The new domains and subdomains were evaluated in group meetings with all authors (DK, RBK, SAvD, PPTJ, GPW) until a consensus was reached.
Patient and public involvement
There was no direct patient or public involvement in this study.
Results
The literature search identified a total of 2903 articles. After duplicate removal, the titles and abstracts of 1898 articles were screened. We selected 131 articles for full-text screening, of which 86 articles met our eligibility criteria. After a thorough screening of the full texts, text passages about scaling were found in 62 articles. Determinants could be identified in the passages extracted from 42 of these articles. This process is outlined in a flow diagram in figure 1. None of the articles discussed determinants of the scaling of de-implementation strategies. The determinants were categorised into four domains: scaling plan, external context, intervention and adopters. The literature-based framework is shown in online supplemental file 3.

Flow diagram.
Study characteristics
A description of the articles that discussed determinants of the scaling of innovations is provided in online supplemental file 5. Twenty-seven studies collected empirical data. These studies were conducted in the UK, the USA, Canada, Australia, Israel or the Netherlands. Furthermore, determinants were found in nine perspectives and six literature reviews. The contribution of each article to the domains and subdomains is shown in table 1.
Supplemental material
Contribution to the subdomains of the literature-based framework per article
Focus groups
Seventeen experts participated in digital focus groups held in April and May 2021. The characteristics of the participants are shown in table 2. All experts agreed that the determinants in the literature-based framework were also relevant for the scaling of de-implementation strategies. They provided nuances and examples of the determinants and added new topics to the framework, such as patients’ perspectives, consequences of medical training and the importance of an alternative to the targeted LVC. Furthermore, they pointed out differences between innovations and de-implementation strategies and their consequences for scaling. The experts in the international focus group emphasised that while the determinants apply to various countries, the content and implications differ due to different contexts, cultures and histories. The results of the focus groups are summarised in online supplemental file 6.
Supplemental material
Characteristics of the participating experts
Cluster of domains
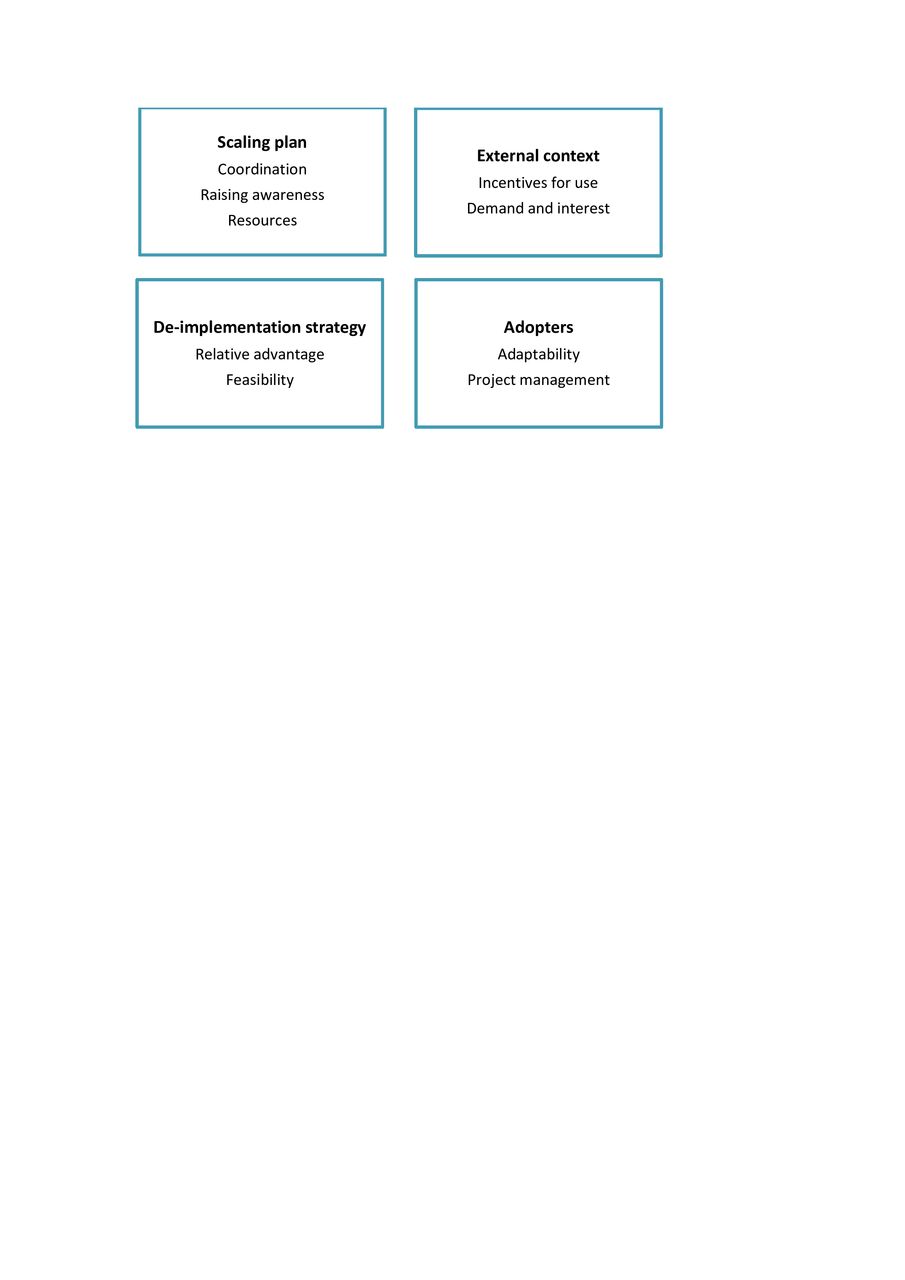
The results of the focus groups were combined with the literature-based framework. This process resulted in the supporting the scaling of de-implementation strategies (SPREAD) framework. The determinants were classified into four domains: scaling plan, external context, de-implementation strategy and adopters. The four domains and their subdomains are shown in figure 2 and table 3. A detailed description is provided below.
Domains, subdomains and determinants of the scaling of de-implementation strategies
{kind=link}
{kind=link}
Domains and subdomains.
Scaling plan
Coordination
The scaling of a de-implementation strategy requires a responsible team. While this team could consist of policymakers, health insurers and healthcare professionals, patients and patient organisations could also lead the scaling process. The scaling team preferably partners with stakeholders and potential adopters of the strategy. Stakeholders differ per strategy; they include members from multiple disciplines and can be regional or national organisations. Stakeholders are not only the targets of a de-implementation strategy but also the ones who are indirectly affected by such a strategy. For example, an audit and feedback strategy requires an organisation that provides data and a receiving healthcare professional. Other stakeholders are the ones who are affected if the strategy is effective at reducing LVC, for example, patients, health insurers and the government. Therefore, patients and patient organisations are often important stakeholders that are valuable for scaling. A partnership with stakeholders should include a shared responsibility to increase the level of commitment. Moreover, scaling is facilitated by partnerships with organisations that have either a large end-user reach or powerful, active members in the target setting. Partnerships ideally start in an early stage, for example, in the developmental stage of the strategy or when the strategy is prepared for scaling. In addition to organising partnerships, the scaling team should also provide support to adopters to make de-implementation as simple as possible. The support can include implementation training, technology support with benchmark data and creating a learning community. Such communities can exchange experiences, knowledge and insights about the strategy and its implementation.
Raising awareness
Potential adopters, including healthcare professionals and patients, must be made aware of the de-implementation strategy. These adopters can be reached through media channels and networks. Media campaigns not only spread information quickly but also shorten the time between awareness and use. Social and professional networks can also be addressed to raise awareness. Therefore, it is important to make use of the networks of the scaling team, the engaged stakeholders and the strategy enthusiasts (opinion leaders). Moreover, peer-to-peer learning is more effective than innovators’ own promotion of their innovations. This underlines the importance of opinion leaders in organisations other than the place of origin. Opinion leaders are persons within an organisation or field who have earned respect by having high levels of competence. They have a strong amount of influence on individual attitudes toward strategies, which can be used to promote the scaling of the de-implementation strategy. In raising awareness, carefully framing of the de-implementation strategy is important since de-implementation can easily be interpreted as a cost-saving measure.
Resources
Resources are crucial for the scaling of de-implementation strategies. Financial resources are needed to execute the scaling plan, and the scaling team should have skilled members. These members should have required knowledge of the external context, including the relevant regulations. With this knowledge, financial and organisational barriers and facilitators can be addressed more effectively. In addition to financial and human resources, sufficient time is needed since scaling occurs slowly.
External context
Incentives for use
Incentives for use are drivers of the use of de-implementation strategies, in addition to advantages of the strategy; they include a reduction of LVC and improved patient outcomes. They can act on all levels: individual, organisational and national. Examples of incentives are financial consequences, employment opportunities, regulatory arrangements, clinical guidelines, accreditation and scientific opportunities. Incentives for de-implementation are often lacking, while the provision of LVC is stimulated by, for example, current payment systems. De-implementation could therefore result in a financial disadvantage in some cases, which is a barrier to scaling. Therefore, incentives to reduce the amount of LVC and incentives for the use of de-implementation strategies should be added, while incentives for the use of LVC should be removed. Whether politicians and policymakers create or remove incentives is influenced by multiple factors. For example, the economic and political climate can drive the strategic priorities of politicians and influence budget choices.
Demands and interest
Scaling is facilitated by a demand for the de-implementation strategy. A demand can start with an urge for less LVC from within society. This urge could stimulate organisations to look for ways to reduce the amount of LVC and could result in a demand for an effective de-implementation strategy. However, there are often conflicting demands in the case of de-implementation; there may be a simultaneous demand to keep providing LVC. This demand can come from all stakeholders, including patients, healthcare professionals, healthcare organisations, and the technology and pharmaceutical industry. All these stakeholders have their own interests, which may influence the demand for the provision of LVC. Additionally, even the availability of LVC can be a source of demand. Demands and interests are influenced by the perceptions of stakeholders. For example, hospitals could be interested in presenting themselves as providers of high-quality care. The common perception of high-quality care is more and innovative care, which could be perceived as contrary to reducing LVC. The perceptions of patients also influence their demands. For example, patients could feel like they have the right to receive care, even if it is of low value, because they pay insurance fees. Therefore, reducing LVC could be perceived as a loss to patients.
De-implementation strategies
Relative advantage
An effective de-implementation strategy leads to a reduction in the amount of LVC provided. The advantage of de-implementation strategies is therefore a reduction in the level of LVC, which indirectly improves patient outcomes. The relative advantage of the de-implementation strategy is the perceived advantage of the reduction of the targeted LVC compared with the current situation. De-implementation is facilitated if the targeted LVC is replaced with an alternative because healthcare professionals prefer to offer patients something more than a wait-and-see approach. Additionally, alternative care should be appealing and should not require more time and effort than the original plan for care. The advantages of de-implementation strategies can be further increased by limiting the risk of failing and decreasing the required investments to conduct the strategies, such as costs and workload. Furthermore, the gains of the strategy should be relevant to patients, adopters and adopting organisations. Examples of relevant gains for patients are an improved quality of life, better clinical outcomes, decreased burdens and favourable social outcomes, such as reassurance. Additional outcomes for healthcare professionals and organisations are higher-quality performance and reduced costs or increased profits. In the case of partnerships, it helps if these parties also benefit from the strategy. The effects of the strategy must be substantiated by evidence about improved outcomes. Evidence is frequently challenged in the case of de-implementation, even when guidelines state that the targeted care is of low value. Therefore, it is important that there is strong supporting evidence.
Feasibility
The feasibility of a de-implementation strategy is determined by its compatibility, adaptability, observability, trialability and complexity. The goal of the strategy should be compatible with the existing values, beliefs, past experiences and needs of potential adopters. Moreover, the influencing factors of providing LVC differ between hospitals and settings. Therefore, the local assessment of barriers and facilitators is essential, and strategies should be adapted according to these findings to fit the local needs and conditions. Adaptability provides the opportunity to modify the overall strategy to fit these local barriers and facilitators; therefore, it is also an important feature. Feasibility is also increased if the effects of the strategy are easy to observe and monitor because insights into the progression of the strategy motivate adopters to continue, and unforeseen effects can be identified and acted upon. Trialability, that is, the ability to test a strategy on a small scale, lowers the initial investment and allows adaptors to experiment with the strategy. Finally, the implementation of the strategy should be simple. A complex strategy can be simplified by implementing it in a stepwise manner.
Adopter or adopting organisation
Adaptability
Adaptability is defined as an adopter’s or adopting organisation’s capacity to change. It depends on the governance regarding change, the available resources and the adaptors’ openness to change. The organisation’s governance could stimulate de-implementation through rapid decision-making and flexibility. Furthermore, de-implementation requires sufficient financial, technical and human resources from the adopting organisations and the time of individual adopters. Openness to change includes the perceived need for change, and it is associated with several adopter characteristics. Influencing characteristics are, for example, the adopter’s age and attitude toward the de-implementation strategy, including his or her trust, confidence, optimism, commitment and support regarding the proposed change. Moreover, the ease of de-implementation depends on past experiences with a particular LVC and how it was promoted during medical training. The belief of the advantage of a particular procedure will be greater if the professional was trained by someone who was confident about its advantage. Consequently, the de-implementation of that procedure will be more difficult. On the organisational level, openness to change depends on the relative balance of the opponents and supporters of the change. This can be influenced by engagement strategies within the organisation. Collaborations between stakeholders at various levels within an organisation can help gain broad support for a de-implementation strategy.
Project management
Strategies must be embedded into organisations. This requires an accountable team composed of team members who have the authority to de-implement within their organisation. De-implementation is facilitated by a plan and strong team leadership. Similar to the scaling plan, partnering with local end-users in early stages helps make strategies compatible with the current way of working. In addition to healthcare professionals, patients are often also end-users of de-implementation strategies. Involving patients is crucial to overcome their resistance to de-implementation. Furthermore, clinical champions who are enthusiasts of the strategy and are willing to promote and support it within their organisations should be selected. After implementation, continuous monitoring, evaluation and adaptation of the de-implementation strategy are recommended. Monitoring the impact and frequent evaluations of the strategy can both increase and sustain its gains. Providing feedback to users motivates the use of the strategy and sustains a positive perception.
Discussion
The SPREAD framework provides an overview of determinants that could be targeted to facilitate the scaling of a de-implementation strategy. These determinants are classified into four domains: scaling plan, external context, de-implementation strategy and adopters. First, scaling plans need to be coordinated by a team. This team should organise partnerships, support adopters, raise awareness among potential adopters and gather resources. The external context preferably includes incentives for the use of a de-implementation strategy, whereas incentives for providing LVC should be removed. The use of de-implementation strategies is also stimulated by the demand for and interest in de-implementation or a specific strategy. Furthermore, the use of a de-implementation strategy ideally leads to advantages over the current situation, and its implementation should be feasible. Last, whether adopters adopt a de-implementation strategy also depends on their adaptability and local project management. Experts have emphasised that while the determinants are country independent, they have implications that vary with context, culture and history.
Comparison with literature
Recently, an article was published about a scale-up programme that aimed to reduce the prescription of potentially inappropriate medication at the emergency department.39 No new determinants were described; the authors confirmed with focus groups the importance of the creation of a learning community, the need for buy-in from stakeholders, the use of data, continuous monitoring and providing feedback, and the adaptability of the strategy components, such as site-specific education.
Our literature search returned only one article that explicitly discussed the role of patients in the scaling of innovations.40 Barber et al described the importance of patients’ support and the roles patients played during the scaling of a medical passport. Their findings were in accordance with the view of the de-implementation experts provided in the current study. They emphasised that patients are important stakeholders in LVC and that their support is crucial. By involving patients in the scale-up, support can be gained, and possible resistance can be overcome. The literature underlines this reasoning as well. For example, Augustsson et al identified patient determinants of the de-implementation of LVC, and the majority of these determinants acted as barriers.41 To overcome these barriers, Born et al suggested partnering with patients and patient organisation, which could build trust among patients and improve de-implementation strategies.42 We emphasise that in addition to being partners, patients and patient organisations can also lead the scaling of a de-implementation strategy. Examples from several countries show that patient organisations can contribute to a reduction in the amount of LVC through the scaling of knowledge and tools that aim to increase shared decision-making.43
All determinants of the scaling of innovations also apply to de-implementation strategies, according to the experts; we expected this shared application due to the resemblance between innovations and de-implementation strategies. The experts added several topics and determinants of de-implementation strategies to the framework, such as medical training, the presence of clear clinical guidelines, and patients’ perspectives and roles. These factors are likely to also influence the scaling of innovations, despite not being described as determinants in our literature selection. We hypothesise that the main difference for scaling lies in the implications and importance of the determinants rather than the determinants themselves. For example, we identified ‘compatibility with the values and beliefs of adopters’ as a determinant of both innovations and de-implementation strategies. Some innovations are additional treatment options that naturally meet the values of healthcare professionals because they are trained to do something for their patients.23 44 45 De-implementation strategies often aim at ‘not doing’, which could seem to undermine professional integrity.46 This implies that de-implementation requires more attention and a different approach to meet the values and beliefs of healthcare professionals.
To our knowledge, this is the first determinant framework for the scaling of de-implementation strategies. Previous frameworks and reviews have focused on either the de-implementation process or the scaling of innovations or interventions.34 36 Our framework distinguishes itself from both types. Compared with determinant models on de-implementation, this framework adds topics such as a scaling plan and a coordination team responsible for the scaling and raising awareness among potential adopters.31 34 41 47 Compared with the literature on the scaling of innovations, for example, Rogers’ diffusion of innovations theory and the Consolidated Framework for Implementation Research, we have added several topics and nuanced the implications of the shared subdomains and determinants.18 21 For example, incentives could be created to support the use of an innovation, such as a payment system that covers its costs.48 Incentives are also facilitators for scaling de-implementation strategies. This framework adds the recommendation to also remove incentives for the use of LVC to support the scaling of de-implementation strategies. In addition, the potential conflicts in demands are addressed in this study. The scaling of innovations is facilitated by the demand for the innovation. In the case of scaling de-implementation strategies, a demand for an effective strategy also acts as a facilitator; however, there are also demands to keep providing LVC, for example, from the pharmaceutical industry. This complicates the scaling of de-implementation strategies.
Strengths and limitations
The methodology we applied to develop this determinant framework has several strengths. This framework is a result of a systematic analysis of recent literature, as well as a critical review of de-implementation experts. The participating experts all have experience with the de-implementation of LVC and have a wide range of backgrounds and professions. Moreover, we included experts from multiple countries. There are, however, also limitations to consider. First, the Dutch experts were sampled from within our network because there are only a few people in the Netherlands who meet our criteria for de-implementation expertise. However, this is unlikely to have influenced the discussion between the experts because no sensitive topics were discussed. Furthermore, we included participants with a variety of backgrounds; however, for some professions, for example, hospital chief executive officers, we included only one person. However, some participants were collaborating closely with hospital boards and could therefore also reflect on institutional factors. In addition, there was an over-representation of experts from the Netherlands. Nevertheless, this framework is internationally relevant because the literature-based framework is based on international literature and all international experts agreed on the described determinants. The experts pointed out that the main difference between countries lies in the implications of the determinants rather than the determinants themselves. Finally, the identified determinants were only reviewed and confirmed by de-implementation experts. Future empirical studies should validate the determinants of the scaling of de-implementation strategies.
Conclusion
The SPREAD framework describes the determinants of the scaling of de-implementation strategies. The determinants are classified into four domains: scaling plan, external context, de-implementation strategy and adopters. All the identified determinants relevant to scaling healthcare interventions are also relevant to the scaling of de-implementation strategies. The determinants present opportunities for a variety of parties to move toward the successful scaling of de-implementation strategies. Future research should validate these determinants of the scaling of de-implementation strategies.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study was conducted in accordance with the applicable legislation according to the Research Ethics Committee of Radboud University Medical Centre (file number: 2021-7519). All participants provided (verbal) informed consent before participating in the focus groups.
Acknowledgments
We thank Daan van Kuppeveld (DVK) and Alice Tillema (AT) for their contribution to this framework. Furthermore, we are grateful to the de-implementation experts for participating in our focus groups.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @tijnkool
Contributors DK, SAvD, GPW, PPTJ and RBK conceptualised and designed the study. DK and RBK performed the literature search, data screening and extraction. DK, RBK and SAvD conducted the interviews and analysed the data. DK, RBK and SAvD performed both data analyses, and the results were discussed with all authors. DK wrote the manuscript, and all authors commented on the sequential drafts of the paper. DK is the author acting as guarantor. All authors approved the final version of the manuscript.
Funding This study was supported by ZonMW, the Dutch Organization for Health Research and Development (grant number: 80-83920-98-803) and the Dutch Ministry of Health, Welfare and Sport (grant number: 331032).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.