Article Text

Abstract
Introduction Improved knowledge of prediabetic subjects’ profile and their risk of developing type 2 diabetes mellitus (T2DM) would enhance secondary prevention. The primary objective is to describe factors associated with incident T2DM in subjects with pre-diabetes diagnosed in primary care.
Methods and analysis The study is based on Reunion Island, a French overseas region that experiences a particularly high disease burden of T2DM. This is an observational, non-randomised prospective cohort study conducted in primary care in which private general practitioner (GP) investigators recruit participants with pre-diabetes from their practices regardless of the initial motive for consultation. Pre-diabetes is defined by WHO criteria, that is, fasting plasma glucose between 1.10 g/L and 1.25 g/L and/or plasma glucose 2 hours after ingestion of 75 g of glucose (2-hour post load plasma glucose) between 1.40 g/L and 1.99 g/L. The design is based on an annual follow-up by the GP (according to French National Health Authority recommendations) with collection of clinical and laboratory data and specific lifestyle questionnaires answered by telephone at three time points: inclusion, and at 2-year and 5-year follow-up visits. Follow-up clinical and laboratory data are collected by the investigating GP as part of the study, and study-specific laboratory collections (serum, DNA and urine) will be obtained 2 and 5 years after inclusion. The primary outcome is transition to T2DM.
Ethics and dissemination This protocol has been approved by the research ethics committee of Saint Etienne (CPP Saint Etienne reference number: 2019–03). Enrolment began in August 2019. Results will be disseminated in at least three papers published in peer-reviewed medical journals, one oral communication and a large-scale communication to the local population and healthcare policymakers.
Trial registration number NCT04463160 and ID-RCB 2018-A03106-49.
- DIABETES & ENDOCRINOLOGY
- PRIMARY CARE
- PUBLIC HEALTH
- PREVENTIVE MEDICINE
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Data from the PREDIABetic subjects from Reunion Island cohort will facilitate the optimisation of the screening and care pathway of Reunionese patients at high risk of type 2 diabetes mellitus (T2DM) and will consequently reduce its incidence.
This project is innovative as it is one of the rare cohort studies conducted in French primary care.
The study will strengthen the network of investigating general practitioner (GPs) in primary care, which will encourage the conduction of other preventive care studies.
This study does not impose additional burdens for follow-up of prediabetic patients compared with official care recommendations.
The major study limitation is that if prediabetic participants do not visit their GPs annually as recommended, relevant data such as the precise period of transition to T2DM might be lost.
Introduction
The rise of plasma glucose levels that precedes the onset of type 2 diabetes mellitus (T2DM) is a continuous phenomenon reflecting the progressive exhaustion of the organs that maintain carbohydrate homeostasis.1 Thus, the WHO defines impaired fasting glucose (IFG) as a fasting plasma glucose (FPG) level between 1.10 g/L and 1.25 g/L (6.1–6.9 mmol/L) and impaired glucose tolerance (IGT) as a 2-hour post load plasma glucose (2hPG) between 1.40 g/L and 1.99 g/L (7.8–11.0 mmol/L) measured by the oral glucose tolerance test (OGTT).2 Patients with IFG and/or IGT are a target population at very high (up to 70%) risk of developing T2DM,3 explaining origin of the ‘prediabetic’ diagnostic category. However, the transition to T2DM is evitable and a return to normoglycaemia is still possible with the early implementation of appropriate lifestyle interventions.4 The prediabetic state is, therefore, targeted for secondary prevention of T2DM.5 A meta-analysis published in 2007 found that the annual incidence of diabetes in subjects with pre-diabetes varied from 5% to 10% depending on different IFG and IGT profiles.6 This variability underscores the importance of the identification of T2DM-associated risk/protective factors for the follow-up and management of subjects with pre-diabetes. Among these risk factors, both IFG and IGT highly increase the risk of incident T2DM.6–8 Other associated factors include male sex, hyperuricaemia, elevated fasting insulin levels and fasting and postprandial free fatty acid levels.7 8 It is also important to note that independently of their diabetic risk, individuals with pre-diabetes are at increased risk of cardiovascular and all-cause mortality9–12 that could be reduced through early detection and management.
In Reunion Island, a French overseas region in the Indian Ocean with a large multiethnic and multicultural diversity, T2DM is a leading public health problem due to its high associated morbidity and mortality. This island has the highest standardised prevalence of pharmacologically treated T2DM of all French regions according to data from the French national health data system (10% vs 5% in Mainland France in 2015).13 In addition, the ENTRED (Échantillon National Témoin Représentatif des personnes Diabétiques) study showed that the epidemiologic profile of Reunionese diabetics differed substantially from that of Mainland T2DM patients, with younger age (48 vs 52 years old at first diagnosis), female preponderance (60% vs 46% women), less prevalent obesity and overweight (27% and 30%, respectively, in Reunion Island compared with 41% and 41% in Mainland France) and complications that occur on average 10 years earlier.14 T2DM prevention is, thus, one of the island’s priority health objectives. Consequently, pre-diabetes is a highlighted target for intervention. Diabetes prevention programmes targeting prediabetic patients have shown worldwide that nutrition and lifestyle interventions are effective to reduce the risk of transition to diabetes in prediabetic patients.15–17 In France, the recommendations for general practitioners (GPs) regular practice are to detect diabetes using FPG and/or 2hPG based on the evaluation of patient’s risk using the Findrisk screening tool.15 If a prediabetic status is discovered, then advices on lifestyle habits are provided, prescription of medication is not recommended. Adherence to the GP recommendations by patients with pre-diabetes is frequently low due to the lack of dedicated programmes in France. In this matter, the French health insurance developed a prevention programme based on the American Diabetes Prevention Program targeting subjects with pre-diabetes in three French department including La Reunion in 2018: the ‘Say no to diabetes’ programme. As GPs are the frontline health actors for pre-diabetes diagnosis, the enrolment of patients in the programme was made by their GP. In this context of GP mobilisation regarding pre-diabetes, we decided to conduct this study in primary care setting. Indeed, we believe that improved knowledge of this population and of the risk or protective factors of the transition to T2DM would assist GPs in the screening and care pathway of subjects with pre-diabetes to reduce T2DM incidence.
PREDIABetic subjects from Reunion Island (PREDIABRUN) is a cohort of subjects with pre-diabetes established in Reunion Island to respond to this need for improved knowledge of pre-diabetes. Subjects with pre-diabetes are included and followed by private GP voluntary investigators. The primary objective of the PREDIABRUN study is to investigate personal, social, clinical and laboratory characteristics of subjects with pre-diabetes and to research those associated with T2DM incidence. Secondary objectives are to:
Study factors associated with normalisation of plasma glucose levels (transition from pre-diabetes to normoglycaemia).
Calculate the annual incidence of T2DM in subjects with pre-diabetes.
Compare PREDIABRUN subjects with existing cohorts of subjects with pre-diabetes in Mainland France (IT DIAB, DAISY) as well as with the subjects of the CONSTANCES cohort study (French general population) to identify possible factors specific to our Reunionese sample.
Study factors associated with the incidence of major cardiovascular events during the study period.
Engage investigating GPs in the screening and management of pre-diabetes.
Methods and analysis
Patient and public involvement
By aiming to improve knowledge on subjects at risk of developing T2DM, PREDIABRUN responds to a primary care issue. In this research context, GPs are the health professionals most likely not only to obtain relevant health data but also to carry out an optimal therapeutic education and follow-up of these subjects. The setting up of this protocol required the collaboration of several GPs who provided essential real-life expertise. The patients were not directly involved in the design of the study, but the follow-up of the patients in PREDIABRUN is based on the national recommendations for annual follow-up of subjects with pre-diabetes.15
The participants will be informed, at their request, of the overall results of the research and a large-scale diffusion to the local population, and healthcare policymakers will also be planned.
Setting and study design
This is an observational, non-randomised prospective cohort study conducted in primary care in which the investigating private GPs recruit subjects with pre-diabetes from their practices. Follow-up is planned for 5 years. Extension of follow-up to 10 years could be considered depending on future funding. Enrolment began in August 2019.
Participants
Inclusion criteria
Age between 25 and 70 years and a diagnosis of pre-diabetes defined as an FPG between 1.10 g/L and 1.25 g/L (6.1 mmol/L and 6.9 mmol/L) and/or a 2hPG between 1.40 g/L and 1.99 g/L (7.8 mmol/L and 11.0 mmol/L) within the preceding 3 months.
Having consulted one of the GP investigators, regardless of the initial reason for seeking care.
Ability to answer a telephone survey questionnaire in French.
Affiliate or beneficiary of a social security plan.
Free and informed written consent signed by the participant and the investigator.
Criteria for non-inclusion
Diagnosis or treatment of diabetes (except gestational diabetes).
Likely to leave Reunion Island within 2 years.
Under guardianship, curatorship or safeguard of justice.
Participation in another research study with an exclusion period still in progress.
Severe physical and/or psychological disorders.
Pregnancy.
Measurements
The French National Authority for Health recommends that subjects with pre-diabetes should visit their GPs annually.15 At a minimum, an annual FPG for T2DM screening should be prescribed. Study data are divided in routine and study-specific categories.
Routine data
Clinical data expected during annual visits include anthropometric measurements, major health events and current medications. The annual laboratory measurements collected are FPG, lipid profile, liver function, complete blood count, blood electrolytes, creatininemia, urea, creatinuria, creatinine clearance and albuminuria based on the National recommendations on prediabetic patients follow-up. The investigating GP is responsible for the recording of clinical and biological data using a standardised questionnaire (online supplemental appendix 1). In addition, specific biological measurement and blood sample are collected at 2 and 5 years of follow-up (see the Study-specific data section). All these data collected will allow at least an annual update on the transition to T2DM.
Supplemental material
Study-specific data
Study-specific laboratory tests planned at the 2 and 5-year follow-up visits include uric acid, glycated haemoglobin (HbA1c), plasma glucose, insulin and C-peptide levels at fasting state and then at 30, 60 and 120 min after the ingestion of 75 g of glucose, associated to the collection of a urine sample (10 mL), serum and DNA (collection of two dry 10 mL tubes of blood.
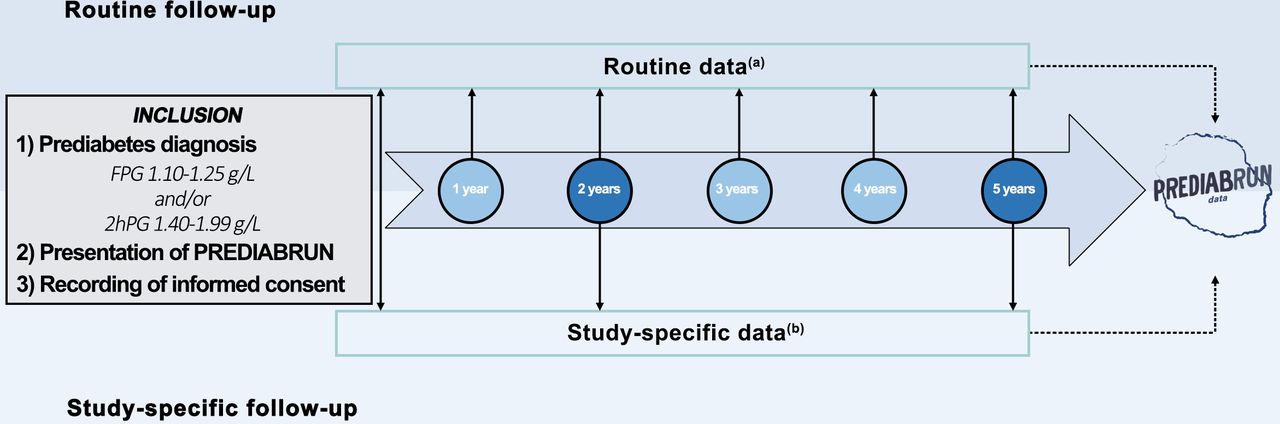
Finally, participants are invited to answer a 30 min telephone survey primarily regarding their social status (inclusion only) and lifestyle habits regarding food, physical activity, sleep and mood at three visits: at inclusion, and at the 2-year and 5-year follow-up sessions (online supplemental appendix 2). Questions regarding depressive symptoms were from the Centre for Epidemiologic Studies Depression Scale16 and the other questions were extracted from the lifestyle questionnaire used in the French national cohort ‘Constances’.17 A summary of the study design is shown in figure 1.
Supplemental material
{kind=link}
PREDIABRUN study design (a) clinical data are recorded during recommended annual visits to the GP for pre-diabetes monitoring and routine laboratory tests including at least FPG (b) 30 min telephone survey regarding social data and lifestyle habits (inclusion, 2-year and 5-year follow-up); study-specific laboratory tests conducted only at the 2-year and 5-year follow-up visits (uric acid, HbA1c, plasma glucose, insulin and C-peptide levels at fasting state and then 30, 60 and 120 min after ingestion of 75 g of glucose; urine, serum and DNA collection). FPG, fasting plasma glucose; GP, general practitioner; PREDIABRUN, PREDIABetic subjects from Reunion Island.
Additionally, a linkage to the French national health data system is planned to explore outcomes that occur beyond the 5-year study period or during intervals lost to follow-up. The French national health data system has a large database that includes but is not limited to data from the national health insurance fund (SNIIRAM database) and hospitals (PMSI database) as well as data on medical causes of death (Inserm CépiDC database). This will enable us to study future potential outcomes such as transition to pharmacologically treated T2DM and major adverse cardiovascular events such as myocardial infarction, stroke and cardiovascular mortality according to different prediabetic profiles.
Outcomes
The primary outcome is the transition to T2DM reported by the investigating GPs, defined by two measurements of FPG ≥1.26 g/L and/or one 2hPG ≥2.0 g/L. In cases of missing laboratory data, diabetes will be defined by the registration of a diabetes diagnosis or diabetes-specific treatment in the patient’s medical record
Regarding secondary outcomes, normoglycaemia is defined by FPG <1.10 g/L and 2hPG <1.40 g/L. Major cardiovascular events comprise stroke, myocardial infarction and cardiovascular mortality and will be studied through data collected by GPs during the study period.
To evaluate the effect of participating in a pre-diabetes research study, changes in pre-diabetes management by the investigating GP sample will be assessed by comparison of knowledge, attitudes and practices (KAP) questionnaires on pre-diabetes obtained at inclusion and after at least 1 year of participation. Specifically, the questionnaire focused on knowledge about pre-diabetes biological definitions, pre-diabetes screening practices and the pre-diabetes management and monitoring (online supplemental appendix 3).
Supplemental material
Sample size
To perform sufficiently detailed and powerful analyses, we chose to include 2000 subjects. The results of the CONSTANCES study presented at the 2018 French Society of Diabetology congress estimated that 7.5% of the population aged 18–70 years in Mainland France is prediabetic, a prevalence 1.5 times higher than that of treated diabetics.18 These results allow us to estimate the number of Reunionese individuals with pre-diabetes of the same age group to between 37 600 (7.5% of the age group as in Mainland France) and 75 300 (15% of the age group due to the twice-higher proportion of subjects with diabetes), based on the estimation of the Reunionese population age groups by the French National Institute for Statistical and Economic Studies in 2018.19 Considering a homogeneous distribution of these individuals between 1200 GPs (Regional health agency 2017 data),20 each physician would follow between 30 and 60 subjects with pre-diabetes. As recruitment for clinical studies is not routine in primary care, the required number of investigating physicians was estimated between 100 GPs and 150 GPs.
Data analysis plan
First, a general description of the sample characteristics at inclusion will be provided. Quantitative variables will be described by mean and SD, median, minimum and maximum values. Nominal variables will be reported by frequency and percentage.
A p value ˂0.05 will be considered statistically significant. Associations between different factors (sociodemographic, clinical, laboratory and lifestyle factors) and the incidence of T2DM will be evaluated by using Cox models. The selection of significant factors will use a stepwise descending procedure. The same procedure will be employed to study the association of the normalisation of plasma glucose and the incidence of major health events.
The annual incidence of T2DM will be presented with a 95%CI by considering the time of follow-up since inclusion in the cohort and the total number of patients followed over the period.
The comparison of the PREDIABRUN sample with samples extracted from other prediabetic cohorts will be achieved by the χ2 test (or Fisher’s exact test) and Student’s t test depending on whether the variables are nominal or quantitative. Sensitivity/specificity analyses of different HbA1c thresholds will be performed in comparison with the classification by OGTT. A receiver operating characteristic curve will be conducted to select the most discriminating threshold. Paired sample comparisons between the results of the KAP questionnaire were completed by investigating GPs at inclusion and 1 year later will be performed by the McNemar test.
Ethics and dissemination
Regulatory aspects
This study has been approved by a research ethics committee of Saint Etienne (CPP Saint Etienne reference number: 2019–03). Informatisation of data is congruent with the 003 reference methodology of the French Commission on Information Technology and Liberty (CNIL). In accordance with the French public health code, the University Hospital of Reunion, promoter of this research, has provided a civil liability insurance policy, and the research is registered on Clinicaltrial.gov and EudraCT. The research is conducted in accordance with this protocol. With the exception of emergencies requiring specific therapeutic procedures, the investigators undertake to adhere to the protocol, with particular regards to the collection of consent and the reporting and follow-up of serious adverse events. The procedure for laboratory specimen collection is declared to the minister in charge of research and to the director of the Regional Health Agency.
Informed consent
During the pre-inclusion visit, which takes place during a usual consultation, the investigating GP presents the PREDIABRUN study to the previously diagnosed prediabetic patient. The investigating GP informs the patient and answers any questions regarding the objectives, potential constraints, foreseeable risks, expected benefits and the rights of the participant in a research study. After this information session, the candidate is given a period of reflection. Written informed consent is obtained before any research clinical or paraclinical examination. In addition, separated signatures are required for the collection of urine, serum and DNA.
Steering Committee
A steering committee composed of the two coordinating principal investigators, representatives of all institutions that collaborated to write the study protocol (the University Hospital of Reunion, the University primary care Department, the regional medical association of private physicians, the association of teaching GPs), the methodologist, statistician, project manager, data manager and a representative of the biological resource centre met before initiating the research and will meet at least annually until the study is completed. Its mission is to make all important decisions concerning the good progress of the research and compliance with the protocol.
Dissemination plan
Results will be disseminated in at least three papers published in peer-reviewed medical journals, one oral communication and a large-scale diffusion to the local population and healthcare policymakers.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CM, EN, SL, J-MF, AD and CK conceptualised the study. CM, EN and LB wrote the first draft of the protocol. NA reviewed and edited it in the BMJ open format. EN and CM validated the final version of the paper.
Funding This work was supported by institutional grants from region of Reunion Island (Région Réunion) and European Regional Development Fund (grant number 20200399–0022774) and by the regional health agency.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.