Article Text

Abstract
Introduction Globally, rheumatic heart disease (RHD) is an important cause of acquired heart disease in children and adolescents. Clinical trials on RHD treatment with Traditional Chinese Medicine (TCM) or integrated medicine are gradually increasing in China. However, because the outcomes of clinical trials are subject to heterogeneity and selective reporting, similar studies cannot be merged and compared, complicating assessing the effectiveness and safety of TCM, and diminishing the value of clinical trials. Therefore, there is an urgent need to design a TCM or integrated medicine core outcome set (COS) for RHD.
Methods and analysis The development of this study will take place in four stages under the direction of a multidisciplinary advisory board. (1) Establishing a comprehensive outcomes checklist through a systematic review of previously published research, retrieval of clinical trial registration centres, patient’s semistructured interviews, and clinician’s questionnaire surveys; (2) Screen stakeholder groups from various fields to participate in the Delphi survey; (3) Two e-Delphi surveys will be conducted to determine the outcomes of various concerned stakeholder groups; (4) Hold a face-to-face consensus meeting to develop the COS-TCM-RHD.
Ethics and dissemination The ethical approval for this study has been obtained from the Tianjin University of Traditional Chinese Medicine Ethics Committee (TJUTCM-EC20210008). The findings will be disseminated in peer-reviewed journals and meetings.
Trial registration number This study has been registered at the Core Outcome Measures in Effectiveness Trials (COMET) database (Registration #1743).
- cardiology
- valvular heart disease
- cardiology
- complementary medicine
- congenital heart disease
Data availability statement
Data are available in a public, open access repository. Data are available upon reasonable request. This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This protocol is the first core outcome set registered on the Core Outcome Measures in Effectiveness Trials website for treating rheumatic heart disease through TCM or integrated medicine.
This study is guided by the Core Outcome Set-STAndards for Development, Core Outcome Set-Standardized Protocol Items and core Outcome Set-STAndards for Reporting.
This study will be supervised by a multidisciplinary advisory board constantly. This investigation will extensively incorporate the perspectives of various stakeholders, including patients, physicians, researchers and policy makers.
The development of the core outcome set will include systematic reviews, qualitative research (patient semistructured interviews and clinician questionnaire surveys), Delphi surveys and consensus meeting.
The main usage of TCM or integrated medicine is in China. Therefore, a restriction will result from the geographical distribution of stakeholders.
Background
Rheumatic heart disease (RHD) is a cardiac sequela of one or more episodes of rheumatic fever (RF), an autoimmune disease caused by group A Streptococcus infection.1 The incidence of RHD is directly related to sanitary conditions.2 3 In low-income and middle-income countries, it is the main cause of cardiovascular death in children and adolescents.4 In 2015,5 approximately 33.4 million patients were diagnosed with RHD worldwide, and 320 000 people died as a result. In 2019,6 the number of RHD cases globally was about 40 million, and approximately 340 000 people died. The number of patients with RHD is likely to continue to rise in the coming years.7 Therefore, RHD is still one of the major diseases affecting human health.8
Western Medicine (WM) treatment of RHD includes primary prevention (early detection and treatment of RF), secondary prevention (application of antibiotics such as penicillin) and tertiary prevention (medical and surgical treatment of RHD and complications).9 10 Although these measures can improve clinical symptoms to a certain extent, the treatment cost is expensive.11 Furthermore, long-term antibiotic therapy may result in major adverse effects, lowering the quality of life of patients with RHD.
Traditional Chinese Medicine (TCM) has rich experience and a unique theoretical system.12 A growing number of RHD clinical trials using TCM or integrated medicine (combining TCM and WM) have been published recently, reiterating the critical importance of TCM therapy.13–15 We differentiated the outcomes of randomised controlled trials (RCTs) on TCM or integrated medicine treatment for RHD. These are the issues we noticed:16 unclear definition of primary and secondary outcomes, a limited selection of surrogate outcomes, contempt of end point and safety outcomes, inconsistent measurement time points, and so on. The above-mentioned issues make it difficult to synthesise outcomes in systematic reviews to do a meta-analysis.17 18 The research findings neither accurately reflect efficacy and safety nor adequately address the needs of relevant groups.19 20
Developing a core outcome set (COS) can address these issues and concerns.21 22 COS is the minimum set of unified and standardised outcomes that must be measured and reported in clinical trials of specific diseases.23 The development of a COS aims to facilitate the comparison of outcomes of similar clinical studies and reduce the risk of selective reporting,24 thus improving the quality of clinical studies and saving the study design cost.25 26
COS studies registered on Core Outcome Measures in Effectiveness Trials (COMET) have increased significantly in recent years.27 But reports on the COS related to TCM or integrated medicine intervention in RHD are unknown. Therefore, a COS of TCM or integrated medicine for RHD is necessary to meet clinical research demands.
Objective
This study aims to determine which effectiveness and safety outcomes should be measured in TCM or integrated medicine clinical trials for RHD.
Scope
Health condition: Patients (≥18 years old) with RHD who have no additional comorbidities or acute exacerbations will be enrolled.
Interventions: TCM (includes herbal medicine decoctions, Chinese patent medicine, acupuncture, cupping, Tuina, moxibustion and other TCM rehabilitation therapy) or integrated medicine application.
Context of use: RCTs.
Methods and analysis
Steering Committee
A steering committee will be formed to examine and confirm research plans, provide advice, settle discrepancies, and participate in consensus meetings. The steering committee will consist of eight experts, two cardiologists, two TCM physicians, two methodologists, one clinical researcher and one COS developer. They will choose one of them to be the committee leader through mutual consent.
Working group
The main tasks of the working group consist of distributing questionnaires and statistical results and holding meetings. The working group will be composed of 8 members, including one TCM clinician, one WM clinician, one methodologist, two professors and three postgraduates from Chinese Clinical Trials COS Research Centre (ChiCOS), Tianjin University of Traditional Chinese Medicine (TJUTCM), China.
Design
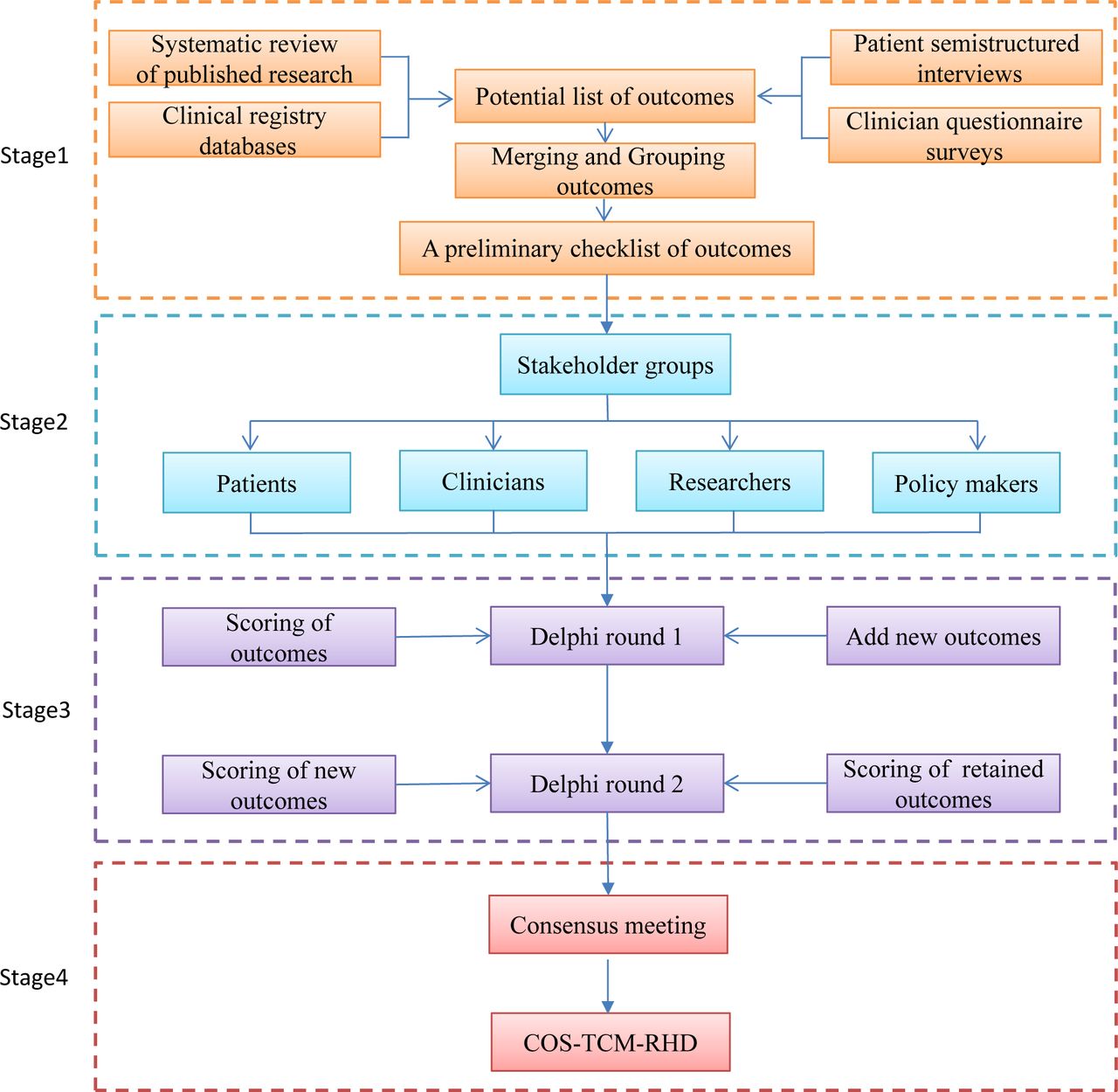
This COS will reference the guidelines from the Core Outcome Set-STAndards for Development (COS-STAD),28 the Core Outcome Set-Standardized Protocol Items (COS-STAP)29 and the Core Outcome Set-STAndards for Reporting (COS-STAR).30 Online supplemental file 1 contains the COS-STAP statement guidelines. This study will be carried out in four parts (figure 1), as follows:
Supplemental material
Stage 1. Identifying potential outcomes, merging and grouping the outcomes to generate a checklist of preliminary outcomes entries.
{kind=link}
The development process for COS-TCM-RHD. COS, core outcome set; RHD, rheumatic heart disease; TCM, Traditional Chinese Medicine.
Stage 2. Screening stakeholder groups in various fields for the Delphi survey.
Stage 3. Conducting two rounds of e-Delphi surveys to determine the outcomes of the various stakeholder groups.
Stage 4. Holding a face-to-face consensus meeting to approve the final COS.
Stage 1: Identification of preliminary outcomes
First, a comprehensive outcomes pool will be established through searching databases and clinical trial registration centres in China and foreign countries, conducting patient semistructured interviews and clinician’s questionnaire surveys. After submitting the results to the steering committee for evaluation, the working group will standardise and categorise the outcomes and create a preliminary list of RHD outcome checklists.
Step 1. A systematic review of published research
Search strategy
The following electronic databases will be searched: PubMed, Embase, Cochrane Library, the Web of Science, AMED (Allied and Complementary Medicine Database) (five English databases in total), China National Knowledge Infrastructure, Wanfang Database, SinoMed and VIP information resource integration service platform database (four Chinese databases in total). The trials published from January 2011 to December 2021 will be included. The languages will be limited to English and Chinese. The search strategy of English databases is shown in online supplemental file 2.
Supplemental material
Eligibility criteria
The inclusion and exclusion criteria for published articles will be as follows (see table 1).
Inclusion and exclusion criteria for published articles
Literature selection
Two reviewers will examine the title and abstract independently and then the full text for another review. A third person will be consulted in the event of a disagreement. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart will be presented,31 including the number of selected and excluded studies and the reasons for exclusion.
Data extraction
The two researchers will independently extract and crosscheck data. The extracted data will include: (1) Basic information of the research, such as title, first author’s name, the time of publication, author’s area, ethical approval, source of funding. (2) Baseline characteristics of the research will include age, course of the disease, sample size, TCM syndrome type (syndrome, symptoms, tongue, pulse). (3) Intervention measures will include the name of intervention, course of treatment, frequency and dose of treatment. (4) Outcome names or definitions, measurement techniques and time points of measurement will all be included.
Step 2. The search of clinical trial registries databases
Search strategy
We will look at the clinical trials.gov and Chinese clinical trials registries. The search period will be from January 2011 to December 2021, with the keyword ‘rheumatic heart disease’ as the search term.
Eligibility criteria
TCM or integrative medicine clinical trial protocols for RHD will be included, and the results of these protocols have not yet been publicly disclosed. The inclusion and exclusion criteria will be the same as in previously reported studies (table 1).
Data extraction
The extracted data will include the registered organisation/researcher’s country, the registered trial status, ethical approval, funding source, research stage, intervention measures, description of outcomes, outcomes measurement methods and time points.
Step 3. Patients’ semistructured interviews
The patient’s opinion is important because the patient directly experiences the benefits and side effects of the treatment. In past COS investigations, semistructured interviews were commonly employed to obtain patient perspectives.32 33 Therefore, we will conduct semistructured patient interviews to supplement patient concerns but not reported outcomes.
Eligibility criteria
We plan to recruit RHD patients (aged ≥18 years old) with experience in TCM or integrated medicine therapy in the First Teaching Hospital of Tianjin University of TCM, the second Teaching Hospital of Tianjin University of TCM, the fourth Teaching Hospital of Tianjin University of TCM and the Tianjin Academy of TCM Affiliated Hospital. Patients with serious mental problems, communication difficulties and other factors that are not conducive to the trial development will be excluded.
Sampling
Following the experience of semistructured interviews in prior COS research,34 35 simple samplings will be used to recruit at least 40 patients. We will consider each patient’s gender, age and treatment history.
Protection of participants
The trained members of the working group will explain the purpose of the interview to patients and ask them whether they want to participate. Patients who agree to participate will sign the basic information form and informed consent form, and the patients will be informed that they can withdraw at any time.
Topic guide
A face-to-face conversation will be used, and the interview will be documented anonymously. First, the working group members will introduce the content of this study to the participants and then ask the patients to point out the outcomes that they thought were important through asking and guiding. The outline content is shown in table 2. The outline content will be piloted and updated as needed.
Questions about semistructured interviews
Data analyses
We will also assess the outcomes of the semistructured interviews as we gather data. The framework methodology will be applied, along with familiarity techniques, to create thematic frameworks, index the data, construct thematic charts, map the data and evaluate the results. Two working group members will examine each outcome, and those found to be new outcomes will be included in the outcome pool with the steering committee’s approval. Any discrepancies will be discussed in order to reach an agreement.
Step 4: Clinicians' questionnaire survey
We will also use computerised questionnaires to acquire relevant outcomes by clinicians but not documented in the literature to diversify the sources of outcomes.
Eligibility criteria
The clinician should be specialised in TCM, WM and integrated medicine. Their main research direction will be cardiovascular disease, and they must have more than 3 years of medical experience.
Sampling size
Referring to previous COS research,36 37 we expect to recruit 40 participants. To ensure that the survey is representative, we will recruit participants from five distinct areas and hospital levels (including outpatient and inpatient departments). The clinicians will be selected from the membership lists of the China integrated TCM and WM Professional Committee and the Chinese Society of Chinese Medicine Cardiovascular Disease Professional Committee.
Protection of participants
The clinicians will be required to sign an informed consent form and fill out an outcome questionnaire and a general information form (education, major, age, gender and work unit).
Topic guide
The questionnaire will be developed in an open-ended format to avoid the restriction of outcome selection and allow clinicians to freely name important outcomes because the clinician group is well acquainted with RHD. Finally, the working group will summarise the survey information.
Step 5: Form a checklist of preliminary outcomes
The working group will summarise the data collected by the above four channels, conduct data analysis and review it by the steering committee. If there is a difference, it will be resolved through discussion or consultation with a third party. The process will be further comprised of four steps:
All outcomes will be numbered and imported into the Excel table, which is convenient to find the source.
The initial results will be validated by standardising outcome names, visualising and integrating results, removing duplicate findingsbefore sorting and recording all outcome names and frequencies.
According to the functional attributes of the outcomes, the initial outcome items will be categorised into seven outcome domains:38 symptoms and signs, TCM disease syndrome, quality of life, physical and chemical examination, economic evaluation, long-term prognosis, and adverse events.
The outcomes will be reviewed by the steering committee. If all outcomes exceed 100, the steering committee will vote internally to delete the outcomes. The outcomes approved by the steering committee will serve as the initial results checklist and will be included in the next Delphi survey.
Stage 2: Selection of Delphi stakeholder groups
The selection of stakeholders is crucial in the production of COS.39 40 We will gather stakeholders from various disciplines and divide them into the following four categories concerning COS-STAD: patients, physicians, researchers and policy makers. The greater the number of stakeholder groups, the more reliable it may be,41 but too many people may also increase the difficulty of investigation and consensus. Given that there is no consensus on the sample size of the Delphi survey,42 with reference to previous studies in which the number of stakeholders in the Delphi survey mostly ranged from 12 to 174,43 we therefore expect to recruit 60 participants using ‘snowball sampling’, 15 for each stakeholder group. If there is clear imbalance among the four groups to start with, we will send more invitation questionnaires to the smaller group, and continue to collect questionnaires for the larger group until the target number is reached. When a group’s size reaches 15, we will cease collecting questionnaires from that group, so that people who exceed this number will not be able to fill in this questionnaire.
An e-invitation letter will be sent to the mailbox of the potential team member, explaining the content of this research and the importance of Delphi, and stating that participants have the right to voluntarily and anonymously withdraw from the research at any time. Clicking on the link in the invitation letter means agreeing to participate in this research. Each member will be assigned a unique identification number to enable subsequent statistics and data storage.
Group 1
Patients ≥18 years of age diagnosed with RHD will be eligible for selection. We will place posters in the public areas of the selected hospitals. We will contact cardiology department doctors through email to invite their RHD patients who are currently diagnosed or have already been diagnosed and treated participate in . The working group members will explain the study’s purpose to the patients in plain language. The patients will have the opportunity to read separate written information sheets, and those who participate in the survey will sign an informed consent form.
Group 2
Clinicians such as cardiologists, TCM physicians, nurses, and clinical pharmacists will be recruited via the hospital’s official website and public WeChat account. In addition, clinicians recommended by the steering committee will be accepted.
Group 3
Researchers, including methodological, clinical, statistical, journal editors, COS developers, and other related experts,will be recruited. We will use social media for advertising job openings and screen high-impact RHD studies, contact the authors, and ask if they are interested in participating.
Group 4
Policy makers, including health management personnel at various levels such as the city, province and county, will be invited. Policy makers' primary sources will be recommendations from potential participants and searches on the health commission’s official website or WeChat. We will contact them by phone or email and ask if they will participate in this survey.
Stage 3: Online Delphi Surveys
A Delphi Survey is a group promotion technology that transforms individual opinions into group consensus through an iterative multistage process.44 We will conduct two rounds of Delphi Surveys in electronic questionnaires, ask stakeholders to score outcomes, and reach a preliminary consensus on the outcomes for RHD treatment with TCM or integrated medicine.
Scoring method
To score candidate outcomes we will use a 9-point Likert Scale45 46 which was developed by the Grading of Recommendations Assessment, Development and Evaluation Working Group and has been recommended by the COMET group47 to be widely used in the Development of COS48 (see table 3).
Showing the 9-point Likert Scale
Round 1
Implementation process
All participants will be required to complete a registration form with basic information, which will be generated independently based on the characteristics of each group. For example, the patient group will be asked to fill in disease information, current treatment plan, and so on, and the clinician group will fill in the job title, position, department, and so on. All candidate outcomes will be compiled and sent to all stakeholders via email. Participants must score every outcome on the Likert Scale described above. To maintain the integrity of the outcomes, we will also invite participants to add other outcomes that they believe are important but are not on the list without scoring them. Because of the patient group’s unique characteristics, we will create a simple questionnaire in plain language to assist patient comprehension. Meanwhile, team members will answer patients' questions online at any time. Participants will have 3 weeks to complete the questionnaire survey, and an email reminder will be sent at the end of the second week.
Data statistics and analysis
After completing the first round of the survey, members of the working group will collect all completed questionnaires, record the number of participants and responses, compute the average score of each outcome and the score distribution of each stakeholder group. The steering committee will review any new recommended outcomes. All saved outcomes will be presented in the next e-Delphi round.
Round 2
Implementation process
All participants completing round 1 will be invited to join round 2 of Delphi. The total number of participants, the proportion of each group and the entire group, the comparison of their scores with other group members, and the new round 1 outcome will be summarised and presented to participants. Participants will be required to use the same scoring criteria as round 1 and re-score the retention outcomes that meet the requirements for entering round 2 (including the newly added outcomes in round 1). If any participant’s score changes, they will be asked to provide reasons. They will have 3 weeks to complete the online survey, and the working group will email participants at the end of the second week, reminding them to respond on time.
Data statistics and analysis
The working group will count the number of participants and responders, the average score of each outcome, the distribution of scores for each stakeholder group, and the potential attrition bias. The average score of participants who complete or do not complete the two survey rounds will be used to compute the dropout bias. Suppose the attrition bias is caused by participants who do not complete both rounds of the Delphi survey. In that case, we will compute the average score of each outcome for participants who do and do not complete both survey rounds. Statistically significant outcomes will be discussed at the consensus meeting. Previous COS research and COMET recommendations42 will be used to develop the consensus definition, as shown in table 4. Finally, the working group will compile all findings into a table and submit it for evaluation to the steering committee.
Definition of consensus
Stage 4: Consensus meeting
In the last step of this study, a face-to-face consensus meeting will be held to discuss and review the final COS. The conference will be held in Tianjin, China, for 1 day. This meeting will be open to all members of the steering committee. Participants who have completed both rounds of the Delphi Survey are also eligible to represent. To reduce the imbalance in stakeholder representation, we will select participant representatives from each stakeholder group at random. The overall number of attendees for this meeting is expected to be 35. The meeting will be hosted by an experienced moderator with no voting privileges.
Consensus meeting content
To make the results of the two rounds of the e-Delphi Survey easier for everyone to understand, the working group will briefly summarise the findings in easy-to-understand language for the participants. According to table 4, the ‘Consensus in’ outcomes are immediately included in the final COS, whereas the ‘Consensus out’ outcomes are directly eliminated. Participants will vote anonymously on the ‘No consensus’ outcomes to determine whether it is ‘Consensus in’ or ‘Consensus out’. If there is any conflict of view, it will be resolved by the steering committee through the Modified Nominal Group Technique.49 After the consensus meeting, the working group will sort out the meeting minutes and form the final COS.
Patient and public involvement
The two rounds of Delphi Surveys, the final consensus sessions and the semistructured interviews will all include participation from patients and the general public.
Discussion
It is highly challenging to combine and analyse Similar studies because the clinical trials of TCM or integrated medicine for RHD have various limitations in their outcomes. This is the first COS-TCM-RHD study to be registered at COMET. Our study plan fully adopted the views of multiple stakeholder groups through systematic review, semistructured interviews, clinicians questionnaires, e-Delphi surveys and consensus meetings.
Suppose this COS can be widely used in clinical and scientific research. In that case, it will help increase the consistency of research, reduce the heterogeneity of reports and improve the value of clinical trials of TCM. COS can improve clinical care and patients' experience when it is relevant to clinicians and patients. Furthermore, COS could help healthcare providers better understand patients' needs and adjust funding priorities for interventions. In conclusion, we assume the COS-TCM-RHD plays a pivotal role in improving the quality of clinical trials, patient care, clinical decision making and policy making.
We will agree on how and when to measure outcomes after the final COS is formed. As a result, following consensus-based norms, the next work will finalise the evaluation of actual outcomes measurement tools.50 This will entail a review of systems, a quality assessment of measurement methods and agreement among stakeholder groups.51 52
Ethics and dissemination
The Ethics Committee has approved the entire project of the Tianjin University of Traditional Chinese Medicine Research Ethics Committee (TJUTCM-EC20210008).
After completing the final COS, we will publish the findings in peer-reviewed and open-access journals, report them at national and international meetings. We also intend to send the publication to all participants of this study. It is hoped that the scope of COS publicity can be expanded and recognised by relevant industry associations.
Data availability statement
Data are available in a public, open access repository. Data are available upon reasonable request. This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
XS and CC contributed equally.
Contributors XS, LG and JZhang conceived the project. XS and CC drafted the protocol and wrote the manuscript in English. BP, MZ and HW participated in the design amendment and helped with project coordination. ZJ and HH participated in the design of the systematic review. JZhai and DZ revised the details and the language. XS and CC are the principal investigators of the project. All authors have read, contributed to and approved the manuscript.
Funding This work was funded by the Special Support Plan for Talent Development of Tianjin-Young Top Talent Project (No. 201504)/Tianjin Graduate Scientific Research Innovation Project (No. 2021YJSB296/No. YJSKC-20211014).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.