Article Text

Abstract
Objectives This study aimed to explore the vitamin D status of children in northern China and the association between vitamin D and glucose metabolism.
Design Cross-sectional study was conducted among child participants and retrospective study designs were conducted among adult participants.
Setting and participants Both studies were recruited from Harbin, 326 children were included in children’s study, 8469 adults were included in adult study.
Primary and secondary outcome measures Physical examination, lifestyle and dietary habit data were recorded in all the participants. Serum insulin, glucose, 25(OH)D3 concentrations in children and serum glucose and lipids levels in adults were measured. Rickets history was also investigated in adults, which was used to define vitamin D deficiency in childhood. The associations were tested by linear regression and binary logistic regression.
Result In the children’s study, only 10.7% of participants were vitamin D sufficient (≥30 ng/mL). Inverse correlations between serum 25(OH)D3 concentration and fasting insulin and homeostasis model assessment - insulin resistance (HOMA-IR) were found, and children with lower serum 25(OH)D3 concentrations were likely to have insulin resistance (IR) (OR: 0.955, 95% CI: 0.917 to 0.995, p value: 0.027). In an adult study, rickets in childhood increased the risk of type 2 diabetes in male participants (OR=1.414, 95% CI=1.013 to 1.972; p value=0.042), but this result was not observed in female participants.
Conclusion Our findings suggest that vitamin D deficiency is widespread in northern China. Vitamin D deficiency in childhood was associated with IR and increased the risk of type 2 diabetes in male adults.
- DIABETES & ENDOCRINOLOGY
- Paediatric endocrinology
- NUTRITION & DIETETICS
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Two studies from Harbin, a city with a high rate of vitamin D deficiency, have important implications for studying vitamin D deficiency in high latitudes and the long-term effects of vitamin D on non-skeletal health.
The analysis of children’s study and the analysis of adults’ study with similar environments and dietary habits were included to support each other’s findings on the association between vitamin D deficiency and glucose metabolism in the two populations.
There was possible selection bias and we did not do the external validity of the sample due to a limitation of external sample. Information on rickets that was used to define vitamin D deficiency in childhood was obtained from self-report, the recall bias was not avoidable although we excluded the uncertain participants.
The sample size of children was small and it was a cross-sectional study. We used odds ratio value to interpret the association of vitamin D deficiency with insulin resistance and diabetes, which may overstate effect sizes.
Introduction
According to the International Diabetes Federation (IDF) statistics, there are 450 million adults with type 2 diabetes worldwide, accounting for approximately 90% of diabetes mellitus cases. Type 2 diabetes has become a global public health problem.1 2 Some recent population studies have found that risk factors such as obesity, impaired glucose tolerance or insulin resistance (IR) in childhood may also increase the risk of type 2 diabetes in adults.3–6 These results suggested that controlling risk factors in childhood is an early prevention strategy to reduce the prevalence of type 2 diabetes in adulthood.
Vitamin D is a fat-soluble vitamin with several physiological functions, one of the most important of which is its effect on skeletal health.7 At present, vitamin D deficiency is still a serious public problem worldwide, particularly in children.8 The prevalence of vitamin D deficiency was approximately 50% in both developing and developed countries.9–12 Serum 25(OH)D3 is less affected by body regulation and is often used to evaluate vitamin D levels. It is usually considered that serum 25(OH)D3<10 ng/mL indicates severe deficiency, 10–20 ng/mL indicates deficiency, 20–29 ng/mL indicates insufficiency and≥30 ng/mL indicates sufficiency.13 Vitamin D deficiency in children is associated with many skeletal diseases, and one of the typical diseases is rickets. The clinical signs of rickets include skeletal deformity, restlessness, motor retardation and bone pain.14
Recently, the association between vitamin D deficiency and extraskeletal health has been of great concern, such as its association with glucose metabolism, obesity, respiratory tract infection and atopic dermatitis, among which the association with glucose metabolism has been of particular concern.15–17 A population study of children and adolescents in Mexico found that low vitamin D levels were associated with IR; when the concentration of serum vitamin D increased, the possibility of presenting IR decreased.18 Reis et al reported that adolescents in the lowest quartile of vitamin D (<15 ng/mL) are more likely to have hyperglycaemic compared with those in the highest quartile (>26 ng/mL).19 Furthermore, randomised controlled trials showed that vitamin D supplementation could increase insulin sensitivity and decrease IR and fasting glucose concentrations in obese children.20–22 Since IR in children is a risk factor for type 2 diabetes, we hypothesised that vitamin D deficiency in childhood might increase the risk of type 2 diabetes in adulthood by affecting insulin sensitivity. A recent 31-year follow-up prospective study in 3–18-year-old young Finns found that high vitamin D levels in childhood could reduce the incidence of type 2 diabetes in adulthood.23 This study further supported our hypothesis, but current research is very limited.
Harbin is a typical northeast city of China, with a latitude between 44°04′N and 46°40′N and is a relatively high-latitude area. The winters in Harbin are long, and the sunlight is relatively insufficient year round, which makes the region’s residents vulnerable to vitamin D deficiency. In our study, we first described the vitamin D nutritional status in children and explored the association between vitamin D deficiency and IR from the Investigation and Intervention of Vitamin D Deficiency in Children (IIVDDC). Then, the association between rickets in children and the risk of type 2 diabetes in adults was analysed using data from the Harbin Cohort Study on Diet, Nutrition and Chronic Non-communicable Diseases (HDNNCDS) in a retrospective study. This study aimed to provide a theoretical basis for the early prevention and control of adult type 2 diabetes development in children.
Materials and methods
Design
A cross-sectional study was conducted among child participants and retrospective study design was conducted among adult participants.
Study population
The child participants were from the baseline survey of IIVDDC from March to May 2019. They were recruited from four kindergartens in Nangang district of Harbin by convenient sampling method, including two public kindergartens and two private kindergartens based on the consideration of different economic levels. The sample size required of children was determined by events per variable criterion≥10, the minimum sample size was calculated to be 90 participants. The parents and teachers of children were invited to informational meetings at which the study and its procedures were explained to them. A total of 440 children aged 3–7 years who had lived in Harbin for the past 3 years were eligible as participants. The exclusion criteria included spending the last winter vacation in the lower latitude areas of Harbin (n=60), who’s information of questionnaire losing>50% (n=54). A total of 326 children were included, and informed written consent was obtained from all custody holders (figure 1).

The follow chart of the children’s study. IIVDDC, Investigation and Intervention of Vitamin D Deficiency in Children; IR, insulin resistance.
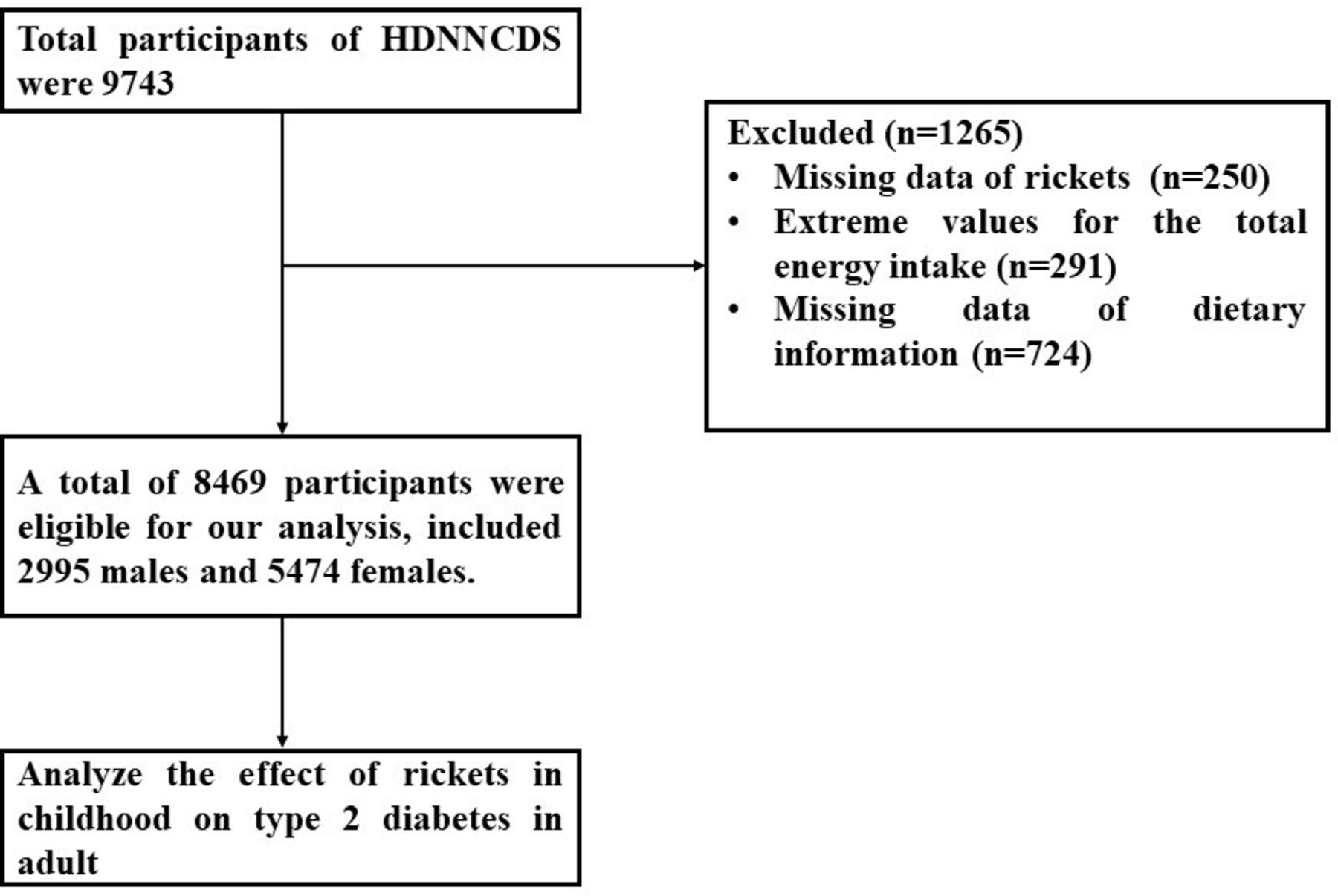
The adult participants were from the baseline of the HDNNCDS.24 Seven urban administrative regions of Harbin were covered in HDNNCDS. According to their financial situation, each region was divided into 3 strata and a total of 42 communities were randomly selected from each stratum in each administrative region by employing a stratified multistage random cluster sampling design. Residents were eligible to participate in the study if they: (1) were between 20 and 74 years old, (2) have been living in Harbin for at least 2 years and (3) were without cancer or type 1 diabetes mellitus. A total of 9734 people aged 20–74 completed the in-person baseline survey in 2010–2012. The sample size required in our analysis was calculated by  , Z1-α/2=1.96, p=12.8%,25 ε=10%. By calculating N=2617, design efficiency value was 2, the final calculated minimal sample size was 5234. Rickets in childhood were investigated in the survey, and participants who had definite answers were included in our study. In the present study, we excluded participants who reported uncertainty about information on rickets in childhood (n=250), who reported extreme values for total energy intake (<500 kcal/day or >4500 kcal, n=291) and who had missing dietary information data (n=724). Finally, a total of 8469 participants were eligible for our analysis, including 2995 male and 5474 female participants (figure 2). Written informed consent was provided by all participants.
, Z1-α/2=1.96, p=12.8%,25 ε=10%. By calculating N=2617, design efficiency value was 2, the final calculated minimal sample size was 5234. Rickets in childhood were investigated in the survey, and participants who had definite answers were included in our study. In the present study, we excluded participants who reported uncertainty about information on rickets in childhood (n=250), who reported extreme values for total energy intake (<500 kcal/day or >4500 kcal, n=291) and who had missing dietary information data (n=724). Finally, a total of 8469 participants were eligible for our analysis, including 2995 male and 5474 female participants (figure 2). Written informed consent was provided by all participants.

{kind=link}
{kind=link}
The follow chart of the adult study. HDNNCDS, Harbin Cohort Study on Diet, Nutrition and Chronic Non-communicable Diseases.
Data collection by the questionnaire
Detailed in-person interviews were administered by trained personnel using a structured questionnaire to collect information on demographic characteristics, lifestyle and dietary intake.
In the IIVDDC, the questionnaire was completed by parents and teachers in kindergartens, together. The demographic characteristics of the children included age and gender. Outdoor physical activity in the past 6 months was investigated, children who had more than 60 min of daily activity or more than 3 days of weekly activity were considered as high exercise frequency, otherwise they were considered as low exercise frequency. Children who took calcium or vitamin D orally or intravenously in the past 6 months were considered as supplementation with calcium and (or) vitamin D. Dietary information was collected by using a Food Frequency Questionnaire (FFQ), and a total of 48 food items were included in the questionnaire, which covered most of the foods in the recipes of the kindergartens included in our study. For each food item, parents and teachers of participants were asked how frequently participants consumed over the preceding year, followed by a question on the amount consumed in lians (a unit of weight equal to 50 g) or mL (for liquid food item) per unit of time. The consumption frequency was transformed to obtain mean consumption a day. Nutrient intakes for each food item consumed were calculated by multiplying the nutrient content listed in the China Food Composition.26 Before dietary surveys, 60 participants from the IIVDDC were recruited and asked to complete two FFQs (FFQ1 and FFQ2) and a 3-day dietary record to validate the reliability of the FFQs. Major nutritional factors (staple food, poultry, fish, vegetable, fruit and milk products) were assessed by the two FFQs and the FFQ2 and 3-day dietary records, and they correlated well after adjusting for energy intake. In IIVDDC, Cronbach’s α coefficient of major nutritional factors between FFQ1 and FFQ2 were 0.67–0.72 and major nutritional factors between FFQ1 and 3-day dietary record were 0.62–0.76. Seventeen factors were extracted, and the cumulative variance contribution rate was 0.649, which suggested the good construct validity.
In the HDNNCDS, the demographic characteristics mainly included age, gender and educational level. Lifestyle referred to smoking, alcohol consumption and physical activity. Current smokers were defined as those who have smoked at least 100 cigarettes lifetime and smoke every day or some days now. Participants who consumed more than 100 mL of white wine, highland barley wine, rice wine, grape wine per day or more than 250 mL beer per day were considered to have a drinking habit. And regular exercise was defined as any kind of recreational or sport physical activity other than walking for work or life performed at least 30 min for 3 or more days per week. Family history of diabetes was also collected. In the FFQ for adults, a total of 103 food items were included in the questionnaire, which covered most of the commonly consumed foods in urban Harbin. The method to validate the reliability of the FFQs in the HDNNCDS was the same as that in the IIVDDC. The correlation coefficients of major nutritional factors between FFQ1 and FFQ2 were 0.61–0.70 and major nutritional factors between FFQ1 and 3-day dietary record were 0.61–0.69, respectively.24 Fifteen factors were extracted, and the cumulative variance contribution rate was 0.832, which suggested the good construct validity. Participants were asked to recall the history of rickets in childhood by specific questions in the questionnaire. The questions included whether they had been diagnosed of rickets at the hospital, had the signs of rickets, such as square head, delay in tooth development, rachitic chest, bow legs or X-shaped legs. The answer options included definitely yes, definitely no and uncertain. Participants who chose one or more ‘definitely yes’ were considered to have rickets in childhood. Participants who reported ‘uncertain’ were excluded from our analysis.
Anthropometric measurement
Anthropometric measurements, including height, weight and waist circumference (WC), were taken by well-trained examiners, with participants wearing light, thin clothing and no shoes. Body weight, height and WC were measured to the nearest 0.1 kg, 0.1 cm and 0.1 cm, respectively. Body mass index (BMI) was calculated as weight (kg) divided by the square of the height in metres (m2). Children’s sex-adjusted and age-adjusted z-scores for BMI (zBMI) were calculated as the calculated value of child BMI minus the median BMI of children of the same age and sex, and then divided by the SD of BMI for children of the same age and sex with the use of WHO AnthroPlus software V.1.0.4.27
Biochemical assessment
Fasting (more than 10 hours) blood samples were collected in children in the IIVDDC. Fasting glucose was determined by an automatic biochemistry analyzer (Hitachi, Tokyo, Japan). 25(OH)D3 was measured using enzyme linked immunosorbent assay (ELISA) kits (Mlbio, Shanghai, China). Serum insulin was measured using the immunofluorescence method (Tosoh automated enzyme immunoassay analyzer AIA-2000ST).
Fasting and postprandial (2 hours after drinking 75 g glucose-containing water) blood samples were taken from all adult participants in the HDNNCDS. Fasting glucose and 2-hour postprandial plasma glucose, blood lipids, including triglycerides (TG), total cholesterol (T-CHO), low-density lipoprotein cholesterol (LDL-c), and high-density lipoprotein cholesterol (HDL-c), were measured using an automatic biochemistry analyzer (Hitachi, Tokyo, Japan). Serum insulin was measured in the same way as children.
Definition of variables
Exposures
In the IIVDDC, serum 25(OH)D3<10 ng/mL was considered severe deficiency, 10–20 ng/mL was considered deficiency, 20–29 ng/mL was considered insufficiency and≥30 ng/mL was considered sufficiency.13 In the HDNNCDS, vitamin D deficiency in childhood was defined as a diagnosis of rickets at the hospital, self-reported rickets or signs of skeletal deformity during childhood.
Outcomes
In the IIVDDC, HOMA-IR was calculated from fasting insulin and glucose using the following formula: fasting insulin concentration (mmol/L) × fasting glucose concentration (mIU/L)/22.5. Children in the highest quartile of HOMA-IR were defined as IR28, the cut-off value of IR was HOMA-IR≥4.58 in our study. In the HDNNCDS, type 2 diabetes was defined as fasting glucose≥7.0 mmol/L and/or 2-hour glucose≥11.1 mmol/L and/or self-report of type 2 diabetes and/or use of hypoglycaemic medicine.
Potential confounders
In the IIVDDC, age, gender, zBMI, intake of energy, vegetable, fruit and livestock, exercise frequency, calcium or (and) vitamin D supplements were included in the analysis as potential confounders of IR. In the HDNNCDS, age, education, BMI, WC, smoking, drinking, exercise, intake of energy, vegetable, fruit and livestock and family history were included as potential confounders of type 2 diabetes.
Statistical analysis
SPSS V.22.0 was used to analyse the data, and a two-sided p value<0.05 was considered statistically significant. Values are mean±SD and n (%) per group for all other variables. Analysis of Variance (ANOVA) and χ2 test were used to compare the differences in the continuous variables and categorical variables between the groups. The linear regression analysis was used to analyse the association between serum 25(OH)D3 concentration and fasting glucose, insulin and HOMA-IR in children, expressed as unstandardized β value and standardised β value. Binary logistic regression analysis was used to analyse the association between serum 25(OH)D3 concentration and IR in children, adjust for age, gender, zBMI, exercise frequency, intake of energy, vegetable, fruit and livestock, calcium or (and) vitamin D supplements, expressed as odds ratio (OR) value and 95% confidence interval (CI). The data from children were finally analysed and presented in general as no gender difference was observed after stratified by sex. Binary logistic regression analysis was used to analyse the association between rickets in childhood with type 2 diabetes in adulthood stratified by sex, adjusted for age, education, BMI, WC, smoking, drinking, exercise, intake of energy, vegetable, fruit and livestock and family history. Bootstrap test of binary logistic regression analysis was used as sensitivity analysis in order to confirm the risk of rickets on diabetes in adulthood male participant.
Patient and public involvement
Participants were not involved in developing research questions, nor the outcome measures/the study’s design. Also, they were not involved in the recruitment to or conduct of the study. In our study, the participants are informed about their blood parameters, and the results of other examinations are gradually shared with them by text message or phone call. The overall findings and benefits of the study will be disseminated through public media.
Results
Results from IIVDDC
Basic information and diet characteristics of children across HOMA-IR quartiles
A total of 326 children were included, 53% were boys and 47% were girls, aged 3–7 years, the average age is 5.24±1.32 years. There were 21 (6.4%) children with severe vitamin D deficiency, 163 (50%) children with deficiency, 107 (32.8%) children with insufficiency and only 35 (10.7%) children with sufficiency.
The basic characteristics of HOMA-IR quartiles grouped children are summarised in table 1. Serum 25(OH)D3 concentration in four quartiles from lowest to highest were 20.82±6.96 ng/mL, 20.96±9.07 ng/mL, 19.94±8.09 ng/mL and 18.19±6.37 ng/mL. Children in higher quartile group had lower proportion of higher sport frequency. There were no significant differences for age, gender, zBMI score, or the supplementation of calcium or (and) vitamin D in recent half year among different quartile groups. The characteristics across quartiles were consistent in boys and girls, and the data were not shown.
Characteristics of the subjects in different homeostasis model assessment - insulin resistance quartiles group
Furthermore, a significant difference in energy intake among quartiles of HOMA-IR was observed, with a slightly higher level in quartile 2 than that in other quartiles (table 2). There were no differences in fruit, vegetable and livestock intakes among different quartiles of HOMA-IR. The above analysis results were consistent in boys and girls, and the data were not shown.
Characteristics of diet in different homeostasis model assessment - insulin resistance quartiles group
The association between serum 25(OH)D3 and fasting glucose, insulin and HOMA-IR
Serum 25(OH)D3 concentration were negatively correlated with fasting insulin and HOMA-IR after adjusting for age, gender, zBMI, exercise frequency, intake of energy, vegetable, fruit and livestock, calcium or (and) vitamin D supplements (fasting insulin: unstandardised β coefficient=−0.178, standardised β coefficient=−0.194, p value=0.001; HOMA-IR: unstandardised β coefficient=−0.032, standardised β coefficient=−0.161, p value=0.005) (table 3). However, the significant association between serum 25(OH)D3 concentration and fasting glucose had not been observed. There was no difference in above analysis results between boys and girls, data were not shown.
Linear regression analysis of the association between serum 25(OH)D3 concentration and fasting glucose and insulin
The association of serum 25(OH)D3 concentration with IR
Children in the highest quartile of HOMA-IR were defined as IR, the cut-off point of HOMA-IR was 4.59. As shown in table 4, after adjusting for age, gender, zBMI, exercise frequency, intake of energy, vegetable, fruit and livestock, calcium or (and) vitamin D supplements, children with low serum 25(OH)D3 concentration were likely to have IR (OR: 0.955, 95% CI: 0.917 to 0.995, p value: 0.027). This association was consistent in boys and girls, and the data were not shown.
Binary logistic regression analysis of the association between serum 25(OH)D3 concentration and IR
Results from HDNNCDS
Basic information, diet and blood biochemical characteristics of adult participants
The basic characteristics of adult participants are shown in table 5. A total of 8469 adult participants, 2999 men and 5474 women were included in our analysis. The average age was 49.58±10.51 years. In both men and women, participants with type 2 diabetes had older age, larger BMI, WC and higher proportion of family history of diabetes, compared with participants without type 2 diabetes. Additionally, the proportion of regular exercise in participants with type 2 diabetes was higher than those without type 2 diabetes. In women, the proportion of drinking was lower in participants with type 2 diabetes and they had lower education levels, whereas the above phenomenon was not observed in men. Furthermore, type 2 diabetes participants had higher T-CHO, TG and LDL-c concentrations and lower HDL-c concentration in both men and women.
Characteristics of the subject in type 2 diabetes and non-type 2 diabetes group, by gender
In men and women, participants with type 2 diabetes had less consumption of fruit, but the difference in energy intake and consumption of vegetable and livestock were not observed (table 6).
Characteristics of energy vegetable, fruit, livestock intake in type 2 diabetes and non-type 2 diabetes group, by gender
The association of rickets in childhood with type 2 diabetes in adulthood
Binary logistic regression analysis showed that rickets in childhood was significantly associated with an increased risk of type 2 diabetes in adult men (OR=1.420, 95% CI=1.017 to 1.983; p value=0.040), after adjusting for sex, adjusted for age, education, BMI, WC, smoking, drinking, exercise, intake of energy, vegetable, fruit and livestock and family history. However, there was no significant association of rickets in childhood with type 2 diabetes in adult female participants (table 7). The result of the bootstrap test was consistent with the result of the binary logistic regression analysis (p value=0.041) (table 8).
Binary logistic regression analysis of the association of rickets on the risk of diabetes in adulthood with different sex
The bootstrap test of binary logistic regression analysis of the association of rickets on the risk of diabetes in adulthood male participants
Discussion
This study examined the association of vitamin D status in childhood with glucose metabolism in the north of China. The results showed that, in children, only 10.7% of participants with vitamin D sufficient, there was a negative association between serum 25(OH)D3 concentration and fasting insulin and HOMA-IR, and children with lower 25(OH)D3 concentration were likely to develop IR. Childhood rickets were associated with an increased risk of type 2 diabetes in adulthood.
Vitamin D deficiency in children is widespread in worldwide. Regardless of the economic level, the vitamin D deficiency rate was very high in children from different countries.9–12 29 30 Vitamin D can be obtained from sunshine and foods, such as meat, eggs and milk. It was generally thought that exposure of skin to ultraviolet rays in the sunshine was the main source of body obtain vitamin D.31 Therefore, the status of serum vitamin D can be influenced by several factors, such as skin tone, the latitude of residence, season or use of sunscreen products.32 Sunshine in areas with high latitude was insufficient for skin to synthesise vitamin D; a previous study showed that residents living in areas above 37°N were insufficiently synthesising vitamin D in winter.33 In relatively low latitude areas of China, 50% of preschooler children had sufficient vitamin D nutritional status (≥30 ng/mL).34 In our study, only 10.7% of children had sufficient vitamin D nutritional status, which was significantly lower than children at low latitudes, vitamin D insufficiency was even more serious. Therefore, we should pay more attention to the health problems caused by vitamin D deficiency and insufficiency at high latitude.
In addition to skeletal health, the association between vitamin D and glucose metabolism in children and adults has also obtained wide concerned. In children, vitamin D deficiency was connected to IR and impaired fasting glucose.13 35 36 However, there were a lack of children studies on the association between vitamin D deficiency and IR in the northern area of China. This study found a negative correlation between serum vitamin D concentration and fasting insulin, HOMA-IR and IR. In adults, previous research suggested that low vitamin D status was associated with IR, impaired glucose tolerance, decreased insulin sensitivity and reduction of insulin secretion18 37–39. Observational study showed that patients with type 2 diabetes had lower level of vitamin D than healthy people.40 An intervention studies have shown that glycated haemoglobin levels decreased after vitamin D supplementation.41 Additionally, prospective studies had indicated that vitamin D deficiency in adults might increase the risk of type 2 diabetes.42–45 According to recent years’ studies, IR in childhood was considered as a risk factor for type 2 diabetes in adulthood.46 Therefore, we speculate vitamin D deficiency in childhood may increase the risk of type 2 diabetes in adulthood by influence IR in childhood. However, this deduction needs a long-term cohort study spanning decades from childhood to adulthood, there have been no reports about this so far.
Nutritional rickets is the most common type in rickets, caused by deficiencies of vitamin D, calcium or phosphate.47 48 The clinical signs of rickets include square head, delay in tooth development, rachitic chest, bow legs or X-shaped legs. Rickets needs to be diagnosed in combination with vitamin D level and clinical signs, and vitamin D deficiency alone cannot be diagnosed as rickets, but children who had serum 25(OH)D3 level under 10.90 ng/mL were likely to have rickets.49 A retrospective survey was conducted on the prevalence of rickets in our adult study, rickets was determined by whether participants had a diagnosis of disease or had symptoms. In adult population of this study, the prevalence of rickets in men and women was 6.3% and 7.9%, respectively. An earlier study reported that the prevalence of Chinese infants with rickets in 1980s was approximately 18%,50 it was higher than our study. This difference may be due to the birth year of our participants being approximately 20 years earlier than those in that study, when China was experiencing societal hardships. Poverty and poor health conditions may lead to the lack of awareness of disease. Furthermore, the information on rickets was retrospective, since some participants were uncertain whether they had rickets in childhood, which may contribute to the low prevalence of rickets. In our adult study, participants who had rickets were defined as having vitamin D deficiency in childhood. The association between rickets and type 2 diabetes in adults was analysed to explore the effect of childhood vitamin D deficiency on type 2 diabetes in adulthood. The results showed that male participants who had rickets in childhood had a higher risk of type 2 diabetes in adulthood, but this result was not observed in female participants. However, the reason for this phenomenon is still unclear. In addition, a study from Finland found that individuals with high levels of vitamin D in childhood and adolescence had a significant lower risk of type 2 diabetes in adulthood compared with those who had lower level of vitamin D.23 These findings collectively suggest that vitamin D deficiency in childhood might increase the risk of type 2 diabetes in adulthood, which needs to be further be explored in more cohort studies and intervention studies.
Some scholars have explored the pathogenesis through which vitamin D deficiency might induce IR in children. The results of some studies shown that, vitamin D levels were inversely related to oxidative stress and inflammation, the increase of reactive oxygen species and formation of cytokines such as interleukin 6 played major roles in IR.51–53 In addition, the findings of an obese, African-American adolescent study showed that low vitamin D levels were correlated with low adiponectin levels, which was associated with IR in children and adolescents.54–57 These results support the finding that vitamin D deficiency in childhood increases the risk of type 2 diabetes in adulthood. At the same time, the results of lab studies also support such pathogenesis: there was a close connection between vitamin D and β-cell function. By regulating cytokines to impact β-cell survival, vitamin D receptor and 1-hydroxylase in β-cell played a role in regulating pancreatic β-cell function, insulin secretion, IR and systemic inflammation.32 58 59 Furthermore, the mechanism of vitamin D decreased IR might relate to the inhibition of vitamin D on inflammation and activation on insulin receptor.60 61 In a term of epigenetics, results showed that vitamin D can also affect the occurrence of type 2 diabetes by regulating the expression of methyltransferase to prevent hypermethylation of diabetes-related genes.62 Above all of these might be the pathogenesis of vitamin D deficiency in childhood increased the risk of type 2 diabetes in adulthood.
An advantage of our study was the inclusion of both children’s study analysis and adult study analysis. The children and adults were both from Harbin, a northeast city of China, was chosen with high prevalence of vitamin D deficiency due to its geographic location. Basically, they had similar geographic and climatic environment and dietary habits. In children, we observed the serum 25(OH)D3 concentration was reversely associated with HOMA-IR. Based on theoretical speculation, we hypothesised that vitamin D deficiency in childhood might increase the risk of type 2 diabetes in adulthood by affecting insulin sensitivity. We defined rickets in adult study as a vitamin D deficiency condition in childhood to simulate the vitamin D deficiency in children’s study. The growth environment related to vitamin D status in the adults was similar with the children. The adults might simulate children’s future growth trajectories to some extent, in terms of the association of childhood vitamin D deficiency with adult type 2 diabetes. The results of the two populations provided mutual support. However, there were also some limitations in our study. First, there was possible selection bias and we did not do the external validity of the sample due to a limitation of external sample. Second, the sample size of children was small and it was a cross-sectional study. We used ORs to interpret the association of vitamin D deficiency with IR and diabetes, which may overstate effect sizes. Third, the rickets information was obtained from self-report, the recall bias was not avoidable although we excluded the uncertain participants. The proportion of self-report rickets was 6.3% and 7.8% for male and female participants, respectively. We assumed that there were some missing reports of rickets in their recalling based on the medical and nutritional condition, and lack of health awareness in China 40 years ago. In addition, the definition of vitamin D deficiency in childhood was rickets, which might have led to some participants, who did not have rickets but vitamin D deficiency, to be classified as non-deficient. Therefore, long-term design and cohort studies with stricter vitamin D nutritional status monitoring are needed to further verify our results.
Conclusions
In summary, vitamin D deficiency in childhood was associated with IR and might increase the risk of type 2 diabetes in adult male participants. Early prevention strategies should be undertaken in children to control the rapid increase in type 2 diabetes worldwide, and management of vitamin D deficiency is probably an effective method.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol of Investigation and Intervention of Vitamin D Deficiency in Children (IIVDDC) and Harbin Cohort Study on Diet, Nutrition and Chronic Non-communicable Diseases (HDNNCDS) was approved by the ethics committee of Harbin Medical University, and written informed consent was provided by all participants. The methods in this study were in accordance the approved guidelines. IIVDDC: ChiCTR1800020294; HDNNCDS: ChiCTR-ECH-12002721.
Acknowledgments
We are grateful to all participants who took part in this study and the research team.
References
Footnotes
Contributors LN and CS designed the study and acquired funding. JL and LN wrote the paper. LF and JZ prepared the original draft. JL, SJ and YJ collected the data. JL and LF analysed and interpreted data. LN is the guarantor. All authors read and approved the final manuscript.
Funding This study was supported by National Nature Science Foundation of China (grant numbers 81872614).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.