Article Text

Abstract
Objective The perioperative chemotherapy with fluorouracil, leucovorin, oxaliplatin plus docetaxel (FLOT) was recommended by the Chinese Society of Clinical Oncology Guidelines for gastric cancer (2018 edition) for patients with resectable gastric or gastro-oesophageal junction adenocarcinoma (class IIA). However, the economic impact of FLOT chemotherapy in China remains unclear. The analysis aimed to compare the cost-effectiveness of FLOT versus epirubicin, cisplatin plus fluorouracil or capecitabine (ECF/ECX) in patients with locally advanced resectable tumours.
Design We developed a Markov model to compare the healthcare and economic outcomes of FLOT and ECF/ECX in patients with resectable gastric or gastro-oesophageal junction adenocarcinoma. Costs were estimated from the perspective of Chinese healthcare system. Clinical and utility inputs were derived from the FLOT4 phase II/III clinical trial and published literature. Sensitivity analyses were employed to assess the robustness of our result. The annual discount rate for costs and health outcomes was set at 5%.
Outcome measures The primary outcome of incremental cost-effectiveness ratios (ICERs) was calculated as the cost per quality-adjusted life years (QALYs).
Results The base-case analysis found that compared with ECF/ECX, the use of FLOT chemotherapy was associated with an additional 1.08 QALYs, resulting in an ICER of US$851/QALY. One-way sensitivity analysis results suggested that the HR of overall survival and progression-free survival had the greatest impact on the ICER. Probabilistic sensitivity analysis demonstrated that FLOT was more likely to be cost-effective compared with ECF/ECX at a willingness-to-pay threshold of US$31 513/QALY.
Conclusions For patients with locally advanced resectable tumours, the FLOT chemotherapy is a cost-effective treatment option compared with ECF/ECX in China.
Trial registration number NCT01216644.
- gastroenterology
- health economics
- gastrointestinal tumours
Data availability statement
Data are available in a public, open access repository.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Perioperative fluorouracil, leucovorin, oxaliplatin plus docetaxel (FLOT) significantly improved overall survival compared with perioperative epirubicin, cisplatin plus fluorouracil or capecitabine (ECF/ECX) in patients with locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma. However, the cost-effectiveness of perioperative FLOT among Chinese patients remains unknown.
To our knowledge, this is the first cost-effectiveness analysis comparing FLOT with ECF/ECX for patients with resectable gastric or gastro-oesophageal junction adenocarcinoma in China.
The use of data in clinical trials may not represent the data in real clinical practice because clinical trials have certain time constraints. For example, we used log-logistic distribution to extrapolate survival beyond the lifetime horizon of the trial.
Introduction
According to the latest global cancer burden data in 2020 released by the International Agency for Research on Cancer of the WHO, China ranked first in the cancer-related deaths with approximately 480 000 cases recorded. Gastric cancer is the third most prevalent malignant tumour in the world and the third leading cause of cancer-related death in China.1
Although significant progress has been made in early detection, the prognosis of patients with resectable gastric and gastro-oesophageal junction adenocarcinoma is still poor.2 Perioperative chemotherapy, adjuvant chemotherapy and adjuvant chemoradiotherapy had demonstrated their superior survival benefit in patients with this disease when compared with a simple surgery.3–6 Based on this, perioperative chemotherapy is recommended as the preferred treatment for locally resectable diseases.3 7–9 For patients whose surgical scope is less than D2 lymph node dissection, postoperative chemoradiotherapy is the preferred treatment.6 10 11 Other treatment strategies, such as postoperative chemotherapy, are applicable to patients who have undergone primary lymph node dissection.12–14 In Asian countries, accumulating clinical evidence has shown that, compared with D2 gastrectomy alone, adjuvant chemotherapy after a D2 surgery significantly improves the tumour remission rate and R0 resection rate is associated with a favourable safety profile.15 16
The Medical Research Council Adjuvant Gastric Infusion Chemotherapy trial was the first clinical trial to confirm the survival benefits of perioperative chemotherapy.3 In this trial, 503 patients with locally advanced resectable gastric and gastro-oesophageal junction adenocarcinoma were enrolled and were randomly assigned to receive three cycles of epirubicin, cisplatin and fluorouracil (ECF) chemotherapy or surgery alone. The survival rate in the chemotherapy group was significantly higher than the simple surgery group (5-year survival rate, 36% vs 23%). The FNCLCC/FFCD II/III trial (multicenter phase trial) also found that perioperative chemotherapy for gastric cancer provided greater survival benefits than the surgery alone.4 According to the trial evidence, the National Comprehensive Cancer Network Clinical (NCCN) Guidelines recommended perioperative chemotherapy as a routine regimen for advanced gastric cancer (class I evidence) in 2022, and a standard adjuvant chemotherapy for gastro-oesophageal adenocarcinoma.17 Subsequently, the Chinese Society of Clinical Oncology (CSCO) Guidelines18 recommended several chemotherapy regimens as preferred schemes, including cisplatin combined with fluorouracil (PF),4 improved ECF scheme,19 oxaliplatin combined with capecitabine,20 oxaliplatin combined with fluorouracil21 and oxaliplatin combined with S-1 (SOX).22 Although the great progress had been made on chemotherapies, the clinical prognosis of patients with advanced gastric or gastro-oesophageal junction cancer is still unsatisfactory, especially those with advanced cancers. In view of this, there is a pressing need for any novel chemotherapy regimen with a greater effectiveness than the existing ones.
In the phase II/III clinical trials of FLOT4, the researchers compared the perioperative chemotherapy fluorouracil, leucovorin, oxaliplatin plus docetaxel (FLOT) with the standard chemotherapy epirubicin, cisplatin, fluorouracil or capecitabine (ECF/ECX).23 24 Fluoropyrimidine and platinum combined with or without anthracycline are the most used chemotherapeutic regimen. In the FLOT4 trial, adding docetaxel to triple-drug regimen (FLOT regimen) was associated with improved survivals among patients with resectable gastric or gastro-oesophageal junction cancer with clinical stage CT2 or higher and lymph node positive (CN+) when compared with ECF/ECX regimen (50 months vs 35 months; HR=0.77; 95% CI, 0.63 to 0.94). In this phase II/III trial, the proportion of patients with complete regression of pathology was significantly higher in the FLOT group than that in the ECF/ECX group. In addition, compared with the ECF/ECX group, patients in the FLOT group had a lower incidence of grade 3–4 adverse events (AEs), including neutropenia, leucopenia, nausea, infection, fatigue and vomiting (25% vs 40%), but had the same incidence of serious chemotherapy-related AEs (27% in both groups).
In response to the positive results from FLOT4 trial, FLOT chemotherapy is recommended for patients with resectable gastric or gastro-oesophageal junction adenocarcinoma (class IIA) by the CSCO Guidelines for gastric cancer (2018 edition). However, its financial impact has not been studied yet from the perspective of Chinese healthcare system. Considering the high prevalence of gastric or gastro-oesophageal junction cancer, and limited health resources in China, the therapeutical benefits of FLOT chemotherapy must be weighed against the economic burden that it has imposed. This study aimed to evaluate whether the perioperative chemotherapy FLOT is cost-effective compared with ECF/ECX among patients with gastric and gastro-oesophageal junction adenocarcinoma from the perspective of Chinese medical system.
Methods
Patients and regimens
The patient population analysed in this study mirrored the patient enrolled in the FLOT4 randomised controlled trial, which assessed the clinical efficacy of FLOT and ECF/ECX chemotherapies in patients with gastric and gastro-oesophageal junction adenocarcinoma. In this study, a total of 716 patients were randomly assigned to receive FLOT (356 cases) or ECF/ECX (360 cases). Patients in the ECF/ECX group received three 3-week cycles preoperative chemotherapy and three 3-week cycles postoperative chemotherapy. The chemotherapy regimen for each 3-week cycle was epirubicin 50 mg/m2 on the first day, cisplatin 60 mg/m2 on the first day and continuous intravenous infusion of PF 200 mg/m2 or oral capecitabine 1250 mg/m2 from the first to the 21st days at the discretion of investigators. Patients in the FLOT group received four 2-week cycles preoperative chemotherapy and four 2-week cycles postoperative chemotherapy, which were docetaxel 50 mg/m2 on the first day, oxaliplatin 85 mg/m2 on the first day, calcium folinate 200 mg/m2 on the first day and 5-FU 2600 mg/m2 as 24 hours infusion the first day.
The operation was scheduled 4 weeks after the last preoperative chemotherapy. The interval between the two groups was 4 weeks (28 days). As per this clinical trial, patients may discontinue treatment due to unacceptable toxicity, disease progression, death or patient requirements. When patients experienced disease progression, they would receive second-line treatment, including irinotecan, calcium folinate and PF.25
Patient and public involvement
There was patient representation in the FLOT4 trial. However, this cost-effectiveness analysis does not involve human participants.
Analytic model
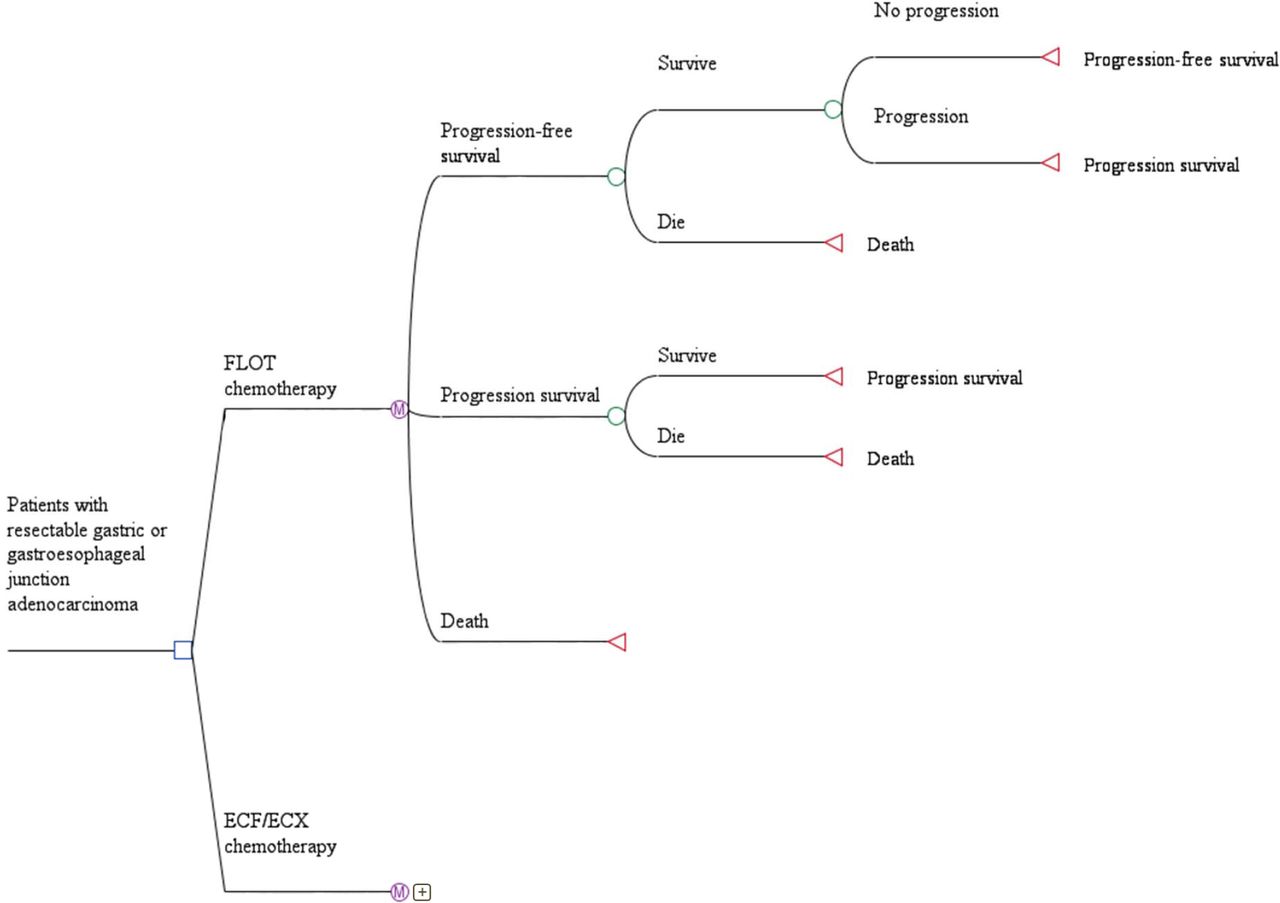
Based on the FLOT4 trial, a Markov model was constructed using Treeage Pro 2018 software to estimate the clinical outcomes of two perioperative chemotherapy regimens (FLOT and ECF/ECX) for patients with gastric and gastro-oesophageal junction adenocarcinoma in China (figure 1).

Markov model structure of fluorouracil, leucovorin, oxaliplatin plus docetaxel (FLOT) and epirubicin, cisplatin plus fluorouracil or capecitabine (ECF/ECX) strategies for the treatment of patients with locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma.
The model comprised three mutually exclusive health states: progression-free survival (PFS), progressed survival (PS) and death. The Markov cycle length was set as 2 weeks to fit the treatment schedule of the two groups. At the beginning of the model, the whole cohort was in PFS state, and the transitions between health states in the model may occur during each Markov cycle. From the perspective of Chinese medical system, we used a lifetime horizon and a half-cycle correction to estimate the total cost, quality-adjusted life year (QALY) and incremental cost-effectiveness ratio (ICER). According to the Chinese Guidelines for Pharmacoeconomic Evaluations, the annual discount rate for both costs and health outcomes was set at 5%.26 All costs used in the model were adjusted based on the consumer price index provided by the People’s Bank of China and the US$ to ¥ in 2020 (US$1=¥6.88).27 A willingness-to-pay (WTP) threshold of US$31 513 was used in the current analysis. This is based on the WHO recommendation based on which a health intervention should be considered as cost-effective if the ICER is between one and three times the gross domestic product (GDP) per capita of that country.26 At this point, it should be mentioned that this WTP threshold has been widely used in cost-effectiveness studies within global health.28–30 The GDP per capita in China was estimated at US$10 504 in 2020.31
PFS and overall survival (OS) data were derived from the Kaplan-Meier survival curve in the trial. First, we used GetDataGraph Digitizer software V.2.24 to extract datapoints from published PFS and OS curves in the publications (http://getdata-graph-digitizer.com). Then, these extracted point data were fitted with different parametric survival models (including exponential, weibull, lognormal and log-logistic). According to the result of statistical goodness-of-fit test using Akaike information standard and Bayesian information criterion, the log-logistic distribution was selected for survival fitting. The two parameters of log-logistic distribution, scale parameters (θ) and shape parameters (κ) are shown in table 1. Finally, we used the parameters to calculate survival rate, which is  , where t is time. Figure 2 shows the log-logistic parameters estimated for the FLOT and ECF/ECX regimens.
, where t is time. Figure 2 shows the log-logistic parameters estimated for the FLOT and ECF/ECX regimens.
Log-logistic parameters

The log-logistic curves of (A) disease-free survival and (B) overall survival. ECF/ECX, epirubicin, cisplatin plus fluorouracil or capecitabine; FLOT, fluorouracil, leucovorin, oxaliplatin plus docetaxel; OS, overall survival; PFS, progression-free survival.
Utility
Since the quality of life data were not published along with the results of the FLOT4 trial, the utility related to gastric cancer was taken from the literatures.20 31 Gockel et al used the Gastrointestinal Life Quality Index to evaluate the quality of life of 338 patients with gastrectomy, and then estimated the utility of patients with PFS health state as 0.81.32 In addition, Sakamaki et al used the time trade-off to evaluate the utility of hospitalised patients with gastric cancer.33 In their study, the utilities of patients receiving intravenous chemotherapy and advanced care were 0.68 and 0.50, respectively. In the current model, we assumed that the utilities of the three health states were identical in both groups. Therefore, 0.68 (1–5 years) and 0.81 (5–10 years) were used as the utilities of patients with PFS health state in both groups. In addition, the utility of patients in PS health state was set to 0.5 and the utility of patients who survived for more than 10 years was set to 1.0.34 The disutility of AEs was calculated by multiplying the utility decrement due to AEs by the incidence of AEs.35 36 We assumed that all AEs occurred in the first cycle.
Cost
From the perspective of Chinese medical system, we considered the direct healthcare expenditure costs in the model, including drug and administration costs, AE management costs, follow-up examination costs, second-line treatment costs, supportive treatment costs and surgery treatment costs. Drug and administration costs, follow-up examination costs and drug price were extracted from the local health system.37 To calculate the dosage of chemotherapeutic drug, we assumed that a baseline patient’s weight was 65 kg and body surface area was 1.72 m2.38
After disease progressed, 25% of the patients in both groups who would receive second-line treatment and the second-line chemotherapy regimen was selected from the FLOT4 trial.39 When the patient experienced further disease progression, they would receive supportive treatments until death.40 The second-line chemotherapy regimen included intravenous injection of irinotecan 180 mg/m2 on days 1, calcium folinate 400 mg/m2 on days 1, PF 400 mg/m2 on day 1, continuous intravenous injection of PF 1200 mg/m2 for more than 24 hours on day 1 and day 2, and circulation every 14 days.25 41 42 Data of the costs for drug administration, supportive and surgery treatments were extracted from the published literature.43–45 The follow-up examination included CT or MRI every 3 months until disease progression, recurrence or death. The price of CT or MRI came from the local health system.37 According to expert suggestions and clinical practice, we calculated the grade 3–4 AEs with a significant difference (p>0.05) between the two groups. Therefore, according to the data available in the FLOT4 trial, the following AEs were included in the model: vomiting (F/E:2%/8%), nausea (F/E:7%/16%), neutropenia (F/E:51%/39%), anaemia (F/E:3%/6%), infections (F/E:18%/9%) and diarrhoea (F/E:10%/4%). Costs for treating AEs were estimated by multiplying the cost per event by the incidence of each AE. The incidences of AEs were obtained from the FLOT4 trial and the unit cost were from the published literature.34 43 46 Table 2 lists all direct costs used in the model.
Baseline costs with ECF/ECX and FLOT perioperative chemotherapy in patients with resectable gastric or gastro-oesophageal junction adenocarcinoma in China
Sensitivity analyses
One-way sensitivity analysis was performed to investigate the impact of individual changes in model parameters on our model results, the results are shown as a tornado diagram. The median, distribution and range of model input parameters are shown in tables 2 and 3, and the ranges corresponding to the model parameters were derived from the published literature or within a reasonable range (±20% or ±50% of the base-case value). In accordance with Chinese Guidelines for Pharmacoeconomic Evaluations, the discount rate in this analysis was assumed to vary between 0% and 8%.26 We also performed a 10 000 repeated Monte Carlo probabilistic sensitivity analyses to evaluate the impact of simultaneous changes in parameters on the model results. In this probabilistic sensitivity analyses, each variable was randomly sampled from the appropriate distribution. A lognormal distribution was applied for the cost data and a beta distribution was applied for the utility value, probability or proportion. The result of PSA was depicted by a cost-effectiveness acceptability curve (CEAC).
Baseline risks and utility values with ECF/ECX and FLOT perioperative chemotherapy in patients with resectable gastric or gastro-oesophageal junction adenocarcinoma in China
Result
The economic and health results calculated by the model are displayed in table 4. The QALYs associated with the FLOT (4.08 QALYs) chemotherapy was longer than that with ECF/ECX (3.0 QALYs), and the FLOT achieved an increase of 1.08 QALYs over the course of disease. Compared with the cost of ECF/ECX regimen of US$45 311.91, the direct medical costs of FLOT regimen was increased by US$921.51 (US$46 233.42 vs US$45 311.91). The corresponding ICER of the FLOT regimen was US$850.68 per QALY. A detailed analysis of cost breakdown (table 5) shows that FlOT increased the second lines of treatment and supportive treatment costs in US$1080.41, plus US$473.34 in drug costs, but allows to save US$1264.89 in the management of the patient. Other cost groups were similar between treatments.
The base-case model results for two treatments
Cost breakdown base-case results
Tornado diagram (figure 3) revealed that the HR of OS was the most influential parameter in our model. When the HR of OS was increased from 0.63 to 0.94, the ICERs ranged from US$3868.18 per QALY to US$−16 856.98 per QALY. Other influential parameters included the HR of PFS, the proportion of surgery patients in the ECF/ECX chemotherapy group and the discount rate. Parameters that have a minor influence on the model included the proportion of AEs, such as nausea, diarrhoea and vomiting (grade 3 or 4). In generally, the ICERs remained below the WTP US$31 513 (three times of China’s per capita GDP) within the fluctuation of all parameters.
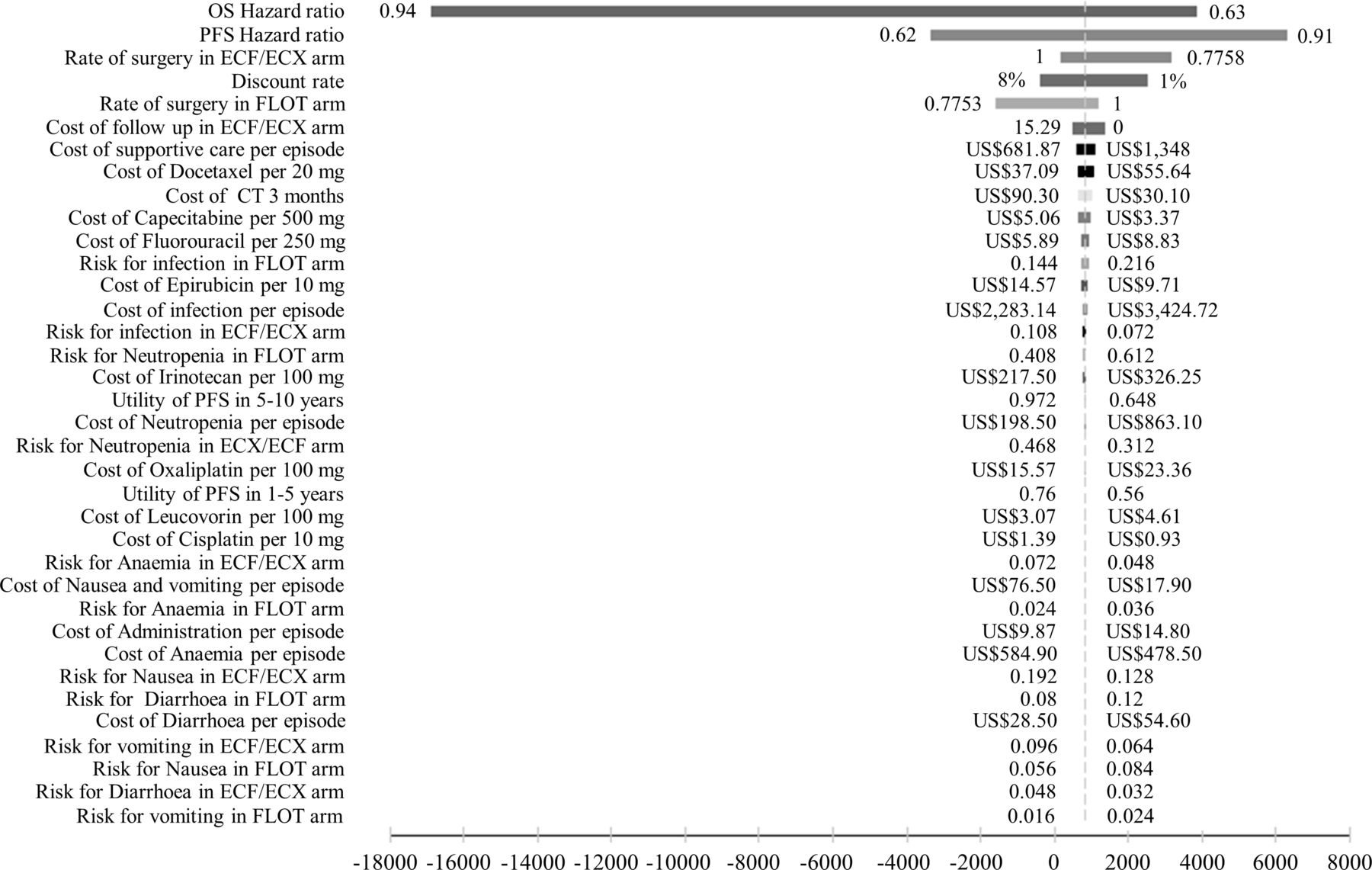
Tornado diagram for univariable sensitivity analyses. The grey dotted line represents the incremental cost-effectiveness ratio of US$850.6842 per quality-adjusted life year from the base-case results. ECF/ECX, epirubicin, cisplatin plus fluorouracil or capecitabine; FLOT, fluorouracil, leucovorin, oxaliplatin plus docetaxel; OS, overall survival; PFS, progression-free survival.
The ICER scatter plot (figure 4) shows the results of the probabilistic sensitivity analyses, including a set of points representing the incremental cost and benefit value pairs in Monte Carlo simulation (10 000 repetitions). The slash is the WTP threshold line, and 95% CIs of the estimates are surrounded by the ellipse. It can be seen from figure 4 that ICER is mostly distributed in the first and fourth quadrants and below the threshold line. The plot below the threshold line accounted for 99.5% of all scatter plots, indicating that the possibility of FLOT chemotherapy regimen being cost-effective compared with the ECF/ECX treatment was 99.5%.

The results of Monte Carlo probabilistic sensitivity analysis for the strategies of fluorouracil, leucovorin, oxaliplatin plus docetaxel (FLOT) versus epirubicin, cisplatin plus fluorouracil or capecitabine (ECF/ECX) in scatter plots. The solid lines indicate the US$31 513 threshold. The estimates of 95% were surrounded in the ellipses. WTP, willingness to pay.
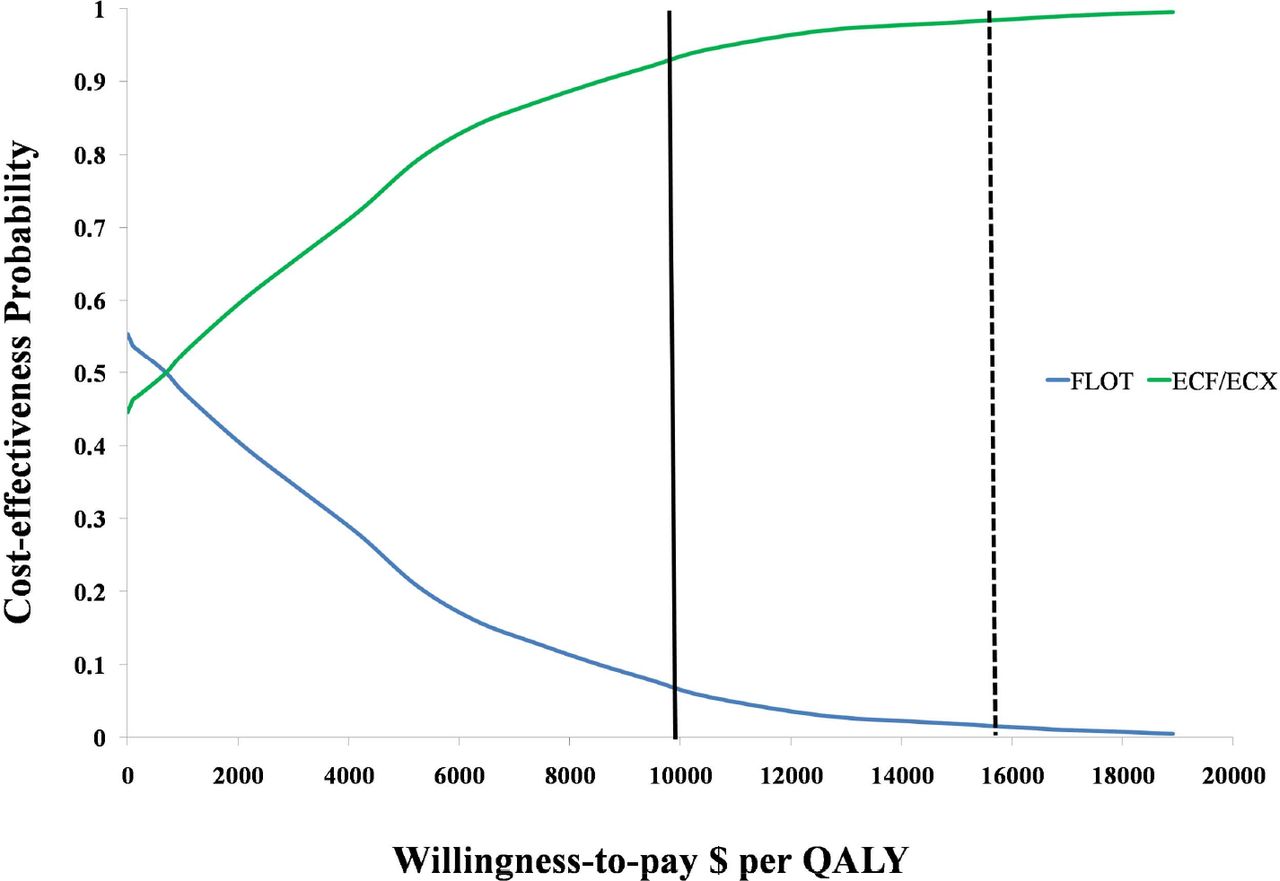
The CEAC (figure 5) shows the cost-effectiveness probabilities of the FLOT chemotherapy generated by Markov Model simulation at different cost-effectiveness thresholds. The cost-effectiveness probability of the FLOT chemotherapy was increased with the increasing WTP thresholds. When the WTP threshold was greater than US$699.2/QALY, the probability of the FLOT chemotherapy being cost-effective was nearly 50% for patients with resectable gastric or gastro-oesophageal junction cancer. When the threshold exceeded US$17 090/QALY, the cost-effectiveness possibility of the FLOT chemotherapy reached 99%.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acceptability curves for the two strategies at willingness-to-pay (WTP) thresholds in locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma patients. The vertical dashed line represents the threshold that the cost-effectiveness probability of fluorouracil, leucovorin, oxaliplatin plus docetaxel (FLOT) chemotherapy reached 99%, and the solid line represents the WTP threshold of US$10 504 (the per capita gross domestic product in China). ECF/ECX, epirubicin, cisplatin plus fluorouracil or capecitabine; FLOT, fluorouracil, leucovorin, oxaliplatin plus docetaxel.
Discussion
Since 2018, the FLOT chemotherapy regimen has occupied an important position in the CSCO guidelines in China and the NCCN in the USA.17 18 Although previous chemotherapy has proved to be effective in improving the OS of patients with advanced gastric cancer after resection, the prognosis of later-stage patients (stages IIIB and IIIC) is still suboptimal. Therefore, further clinical studies are needed to find more effective perioperative treatment for gastric cancer.
In recent years, the use of anthracycline and platinum drugs has sprouted in the field of perioperative treatment of resectable gastric cancer. Two published phase III studies have demonstrated the clinical efficacy of docetaxel in the treatment of advanced gastric cancer, involving docetaxel, oxaliplatin, S-1 and docetaxel combined with S-1.47 48 Moreover, oxaliplatin has showed favourable safety in the treatment of gastrointestinal tract, liver, kidney and bone marrow than cisplatin and carboplatin. Therefore, oxaliplatin has gradually replaced cisplatin in the current commonly used chemotherapy regimens. In the ARTIST-II trail, the SOX regimen showed superiority over single drug (S-1) in prolonging patient’s survival.49 Two pivotal phase III trials from Japan and South Korea also found that oxaliplatin combined with folic acid and S-1 was associated with a clinically significant improvement among patients with advanced gastric cancer, when compared with S-1 plus cisplatin.50 Based on these positive results, docetaxel and oxaliplatin have been introduced into FLOT chemotherapy regimen. At present, FLOT regimen is considered as a preferred strategy for perioperative chemotherapy combined with surgery, including three chemotherapeutic drugs that suitable for patients with good performance status. Notably, for patients with good-to-moderate performance status and patients who are not able to tolerate the combination regimen of these three drugs, the two-drug combination regimen is recommended.
In China, the climbing incidence and mortality of gastric cancer have imposed considerable physical, psychological and economic burdens on the society, patients and their families. Therefore, it is very crucial to study the economic significance of this chemotherapy strategy in the field of medicine and policy. In this economic evaluation that compared with the ECF/ECX, the use of FLOT in patients with gastric and gastro-oesophageal junction adenocarcinoma achieved additional 1.08 QALY at an incremental cost of US$921.51, resulting in an ICER of US$850.68/QALY. Based on the WTP threshold set for this analysis, the FLOT strategy was considered to be cost-effective. However, due to the extreme imbalance of economic development in Chinese Mainland, the per capita GDP of the 32 provincial-level administrative regions varies greatly. The highest per capita GDP was reported in Beijing’s per capita GDP (US$23 968) and the lowest was reported in Gansu’s (US$5238).51 For the whole Chinese Mainland, the per capita GDP was US$10 504 and three times the per capita GDP was US$31 513. Because the ICERs of the FLOT strategy were much lower than three times the per capita GDP in Gansu province (US$15 714). This suggests that the FLOT perioperative chemotherapy regimen is more cost-effective than ECF/ECX in the treatment of locally advanced resectable gastric or gastro-oesophageal junction adenocarcinoma in all provincial-level administrative regions in Chinese Mainland.
The one-way sensitivity analysis showed that the most influential parameter on the model results was the HR of OS. Specifically, when the HR decreased from 0.94 to 0.63, the ICER of FLOT strategy versus ECF/ECX strategy ranged from US$−16 856.98 per QALY to US$3868.18 per QALY. The other sensitive parameters included the HR of PFS, the proportion of patients with ECF/ECX who underwent surgery and the discount rate. The change of HR for OS made ICER fluctuate the most, but the ICER was still less than WTP (US$10 504/QALY). Moreover, the ICER of FLOT strategy versus ECF/ECX strategy was always much lower than WTP regardless of the large fluctuation of model parameters. Consequently, we can conclude the uncertainty of parameters will not affect the robustness of our results.
It should be noted that, docetaxel prices played a more important role than the prices of other drugs in our model. From the perspective of patients with cancer, the use of high-priced new drugs might impose a heavy financial burden on the both social and patients, which likely leads to delay, abandonment and discontinuation of treatment.52 In recent years, the Chinese government has conducted a series of price negotiation with many pharmaceutical enterprises with the aim of reducing the price of oncology drugs. Fortunately, docetaxel passed the price negotiation and the consistency evaluation of generic drugs successfully in March 2021.53 This means that the market price of docetaxel will drop, which will make docetaxel less costly and more widely used in China. Since the implementation of the national drug centralised procurement policy and the generic drug consistency evaluation, we can expect that patients with cancer may benefit from these policies in China. To the best of our knowledge, this study is the first cost-effectiveness analysis of FLOT chemotherapy in patients with resectable gastric or gastro-oesophageal junction adenocarcinoma.
There are some limitations in the current study. First, there is uncertainty regarding the outcomes of patients with gastric and gastro-oesophageal junction adenocarcinoma beyond the trial period, despite the use of validated extrapolation techniques. Second, some potential bias lied in only direct medical costs were incorporated in the model; however, our sensitive analysis found that our results were almost unaffected by changes in costs. Third, another limitation of the current economic analysis was that other treatment strategies for advanced resectable gastric cancer have not been fully explored. With the successful application of targeted therapy and immunotherapy for advanced gastric cancer clinically, the pattern of perioperative treatment of resectable gastric cancer have been refreshed. For example, the research on treatment of HER-2 (Human epidermal growth factor recptor-2) positive gastric cancer has attracted considerable attentions in recent years. Meanwhile, combining the perioperative chemotherapy with targeted treatment was found to increase the pathological complete remission rate and improve OS benefit, while the safety is acceptable.54 55 Therefore, we can expect that receiving higher cost-targeted therapy can increase more cost-effectiveness.
Data availability statement
Data are available in a public, open access repository.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Contributors Study design and supervision were contributed by HZ and XZ. Data analysis and interpretation were contributed by HZ, XZ and L-YS. Data collection was contributed by HZ and CW. Manuscript writing was contributed by HZ, XZ, S-JJ and QL. HZ is responsible for the overall content as guarantor. HZccepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish. Final approval of the manuscript was contributed by all of the authors.
Funding This work was supported by the Provincial Natural Science Foundation (grant number 2021JJ80080).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.