Article Text

Abstract
Objective We undertook a systematic review of strategies adopted to scale up COVID-19 testing in countries across income levels to identify successful approaches and facilitate learning.
Methods Scholarly articles in English from PubMed, Google scholar and Google search engine describing strategies used to increase COVID-19 testing in countries were reviewed. Deductive analysis to allocate relevant text from the reviewed publications/reports to the a priori themes was done.
Main results The review covered 32 countries, including 11 high-income, 2 upper-middle-income, 13 lower-middle-income and 6 low-income countries. Most low- and middle-income countries (LMICs) increased the number of laboratories available for testing and deployed sample collection and shipment to the available laboratories. The high-income countries (HICs) that is, South Korea, Germany, Singapore and USA developed molecular diagnostics with accompanying regulatory and legislative framework adjustments to ensure the rapid development and use of the tests. HICs like South Korea leveraged existing manufacturing systems to develop tests, while the LMICs leveraged existing national disease control programmes (HIV, tuberculosis, malaria) to increase testing. Continent-wide, African Centres for Disease Control and Prevention-led collaborations increased testing across most African countries through building capacity by providing testing kits and training.
Conclusion Strategies taken appear to reflect the existing systems or economies of scale that a particular country could leverage. LMICs, for example, drew on the infectious disease control programmes already in place to harness expertise and laboratory capacity for COVID-19 testing. There however might have been strategies adopted by other countries but were never published and thus did not appear anywhere in the searched databases.
- COVID-19
- public health
- health policy
Data availability statement
Data may be obtained from a third party and are not publicly available. Data will be made available to others on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
There have been challenges in testing in both developed and developing countries.
The strength of this systematic review is that it covers many countries across different income categories and provides strategies that worked for countries that other countries could leverage to increase testing now and for future pandemics.
The findings point to the diverse nature of the laboratory response across both developed and developing nations, mainly driven by the nature of existing capabilities and expertise.
The major limitation of this systematic review is an inability to link the testing strategies to testing rates in each country.
Introduction
At the end of 2019, a disease that presented with pneumonia in the Chinese city of Wuhan emerged.1 The disease (caused by the SARS-CoV-2 virus) was later named COVID-19 and subsequently declared a global pandemic by the WHO on 11 March 2020. Almost 2 years into the pandemic, both big and small economies have been hugely affected, and countries will likely continue to suffer for many years after the pandemic’s peak. As of 16 December 2021, a total of 273 019 599 cases and 5 338 972 deaths from COVID-19 have been reported.2 In North America, the USA has notified most cases per 100 000 population while the UK, India, Brazil and South Africa top the list in Europe, Asia, South America and Africa, respectively.2
Initially, scientists knew little about the disease and the virus, but there have been significant scientific advancements regarding prevention, diagnosis, treatment and prevention. The world moved from having no or few diagnostic tools to a plethora of diagnostic tools. Furthermore, there has been an unprecedented rapid development and deployment of vaccines, which could be game-changing to ending the pandemic. However, control efforts have been complicated by the emergence of variants, threatening vaccine efficacy.3
Beyond the non-pharmacological interventions deployed by countries to combat the pandemic, testing has been deployed to control the spread of COVID-19 by identifying, isolating and treating those infected. Indeed, a few months into the pandemic, WHO called on countries to ‘test, test and test’.4 5 This was premised on the belief that early testing and contact tracing could interrupt transmission.
Amidst the calls for increased testing, WHO developed an emergency use listing procedure to expedite in vitro diagnostics to support testing,6 to ensure the availability of diagnostics needed for the public health emergency. WHO also made several recommendations to guide countries on testing. Initial guidance on approaches to testing was based on the number of cases reported per country (sporadic cases, clusters of cases and community transmission). WHO suggested the need for prioritised testing strategies within countries due to the variation in levels of community transmission.7 With the emergence of new tools like antigen detection rapid diagnostic tests (RDTs), the recommendations have been updated. WHO maintained nucleic acid amplification tests (NAAT) as the reference standard and recommended antigen RDTs as a complementary strategy.8
Despite the advice that testing should underpin the disease control efforts, there have been shortfalls across different countries. There is a noticeable lack of harmonised testing strategies across the globe due to several challenges, including the prepandemic laboratory capacity, barriers to access of tests due to increased demand and challenges with supply.9 To overcome some of the challenges, countries adopted different strategies to increase the number of tests per capita.
Developing countries (low- and lower-middle-income countries, see Results section for definitions) were deemed more likely to bear the heaviest burden of the pandemic, mainly due to fragile healthcare systems, political instability, economic vulnerability, limited fiscal space, equipment shortages, among others.10 11 This, however, does not seem to have been the case. For example, the number of cases in most African countries remains reasonably low, with low mortality rates reported.11 12 While there are many possible reasons why cases have stayed lower than anticipated, it is possible that there is inadequate testing in most of these countries. Indeed, low test per capita rates have been noted in Africa.13 Some reports have pointed to undercounting of deaths due to COVID-19.14
Challenges with testing have also been observed in developed countries,15 16 indicating that finances alone are not enough to achieve the desired testing capabilities. While the more affluent countries have outcompeted the rest on the COVID-19 diagnostics market,17 many developing countries have used what they have at their disposal to scale-up testing.
Future pandemics are always a possibility, and lessons must be learnt from the current pandemic to enable robust and expedited responses. There is an opportunity for countries at all income levels to learn lessons from each other. Based on this background, we undertook a systematic review of strategies adopted to scale up COVID-19 testing in countries of all income levels to identify successful approaches and facilitate shared learning.
Methods
The overall aim of the systematic review was to examine strategies adopted to scale up COVID-19 testing in low-, middle- and high-income-countries and identify drivers underlying the selection of strategy in a given setting.
Inclusion/exclusion criteria
We included original scholarly articles published in English between December 2019 and September 2021 describing strategies used to increase COVID-19 testing in different countries. Articles included original studies, situational and practice reports, case reports, features, commentaries, viewpoints, reviews and perspectives. Any scholarly articles that proposed strategies to scale up testing, but with no mention of whether these strategies had been implemented were excluded. The main outcome for the studies was COVID-19 testing strategy and given the diversity in the testing strategies, studies were grouped under themes to support the analysis.
Search strategy
The search was performed using resources and methods that ensure methodological transparency and reproducibility of the findings, leveraging the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P) guidelines.18 The search strategy was guided by the patient/population, intervention, comparison and outcomes (PICO) approach. For this case, the population was the individuals in the countries, intervention was the COVID-19 testing, while the outcome was COVID-19 testing strategy countries. The study did not have a comparative reference. We asked: What strategies were adopted to scale up COVID-19 testing in Low- Middle and High-Income countries? To obtain more relevant articles, we reviewed the bibliography section of the reviewed articles.
We used the following terms/statements to search the studies for consideration in the systematic review: COVID-19 diagnostics in Asia, South America, Latin America, Europe, North America; COVID-19 diagnostics in high-income countries; COVID-19 diagnostics in middle-income countries; COVID-19 diagnostics in low-income countries; COVID-19 testing in high-income countries; COVID-19 diagnostics in Asia, South America, Latin America, Europe, North America; increasing COVID-19 testing in Asia, South America, Latin America, Europe, North America and COVID-19 laboratory testing strategies. The publications returned by the search strategies are summarised in online supplemental table 1, while the publications included and the corresponding testing strategies are summarised in online supplemental table 2.
Supplemental material
Supplemental material
Data access and management
The investigation team of three researchers accessed the internet sources (PubMed, Google scholar, and google search engine), identified and retrieved all the articles. All the retrieved articles were carefully analysed to identify and remove duplicates and irrelevant articles. Researchers through consensus agreed on the final list to consider. The team used the Mendeley referencing manager to store, organise and manage all the articles.
Database/sources searched
The researchers independently searched for scholarly articles (original studies, situational and practice reports, case reports, features, commentaries, viewpoints, reviews and perspectives) in PubMed, Google scholar and Google search engine (all last searched on 17 September 2021). Titles and abstracts were independently screened by researchers based on the inclusion criteria.
Study selection criteria and process
All qualitative or quantitative scholarly articles describing strategies adopted were included in the general screen. Further refinement considered only studies that offered information on the strategy used to increase COVID-19 testing in low-, middle- and high-income countries were considered further for inclusion.
The selection was carried out by the three researchers working independently. They then convened and reviewed the individual lists and harmonised to agree on one list of studies to be included. The three researchers have postgraduate qualifications in health-related disciplines.
Data extraction
Both abstracts and full texts were read to identify strategies countries used to increase COVID-19 testing. The outcome was COVID-19 testing strategy and in reviewing the selected articles, researchers sought information on the different approaches that countries used to increase and expand COVID-19 testing. This was achieved through the use of a predeveloped codebook that captured the outcome (online supplemental table 3). The codebook guided the identification of strategies and included themes and narratives of what the researchers were to consider as strategies for increasing testing. Where the researchers found any strategy not captured by the codebook, they noted this. The other variable sought in the reviewed articles was the COVID-19 testing methods used. The findings were later harmonised and summarised in a table that included authors, source of publication, date of publication, country, income category and strategy or strategies used.
Supplemental material
Data analysis
Analysis entailed appraising and synthesising texts from the scholarly articles, which were then organised into major themes and content analysis, guided by the predeveloped codebook. We used deductive analysis to allocate relevant text from the reviewed publications and reports to the a priori themes. In the process of allocating text, there were emergent new themes. New and a priori themes included accessibility, diagnostics, regulatory and legislation, integration, personnel, technology and innovation and collaboration.
Patient and public involvement
Patients and the public were not involved in any way.
Ethics statement
No human participants were included.
Results
Study selection and characteristics
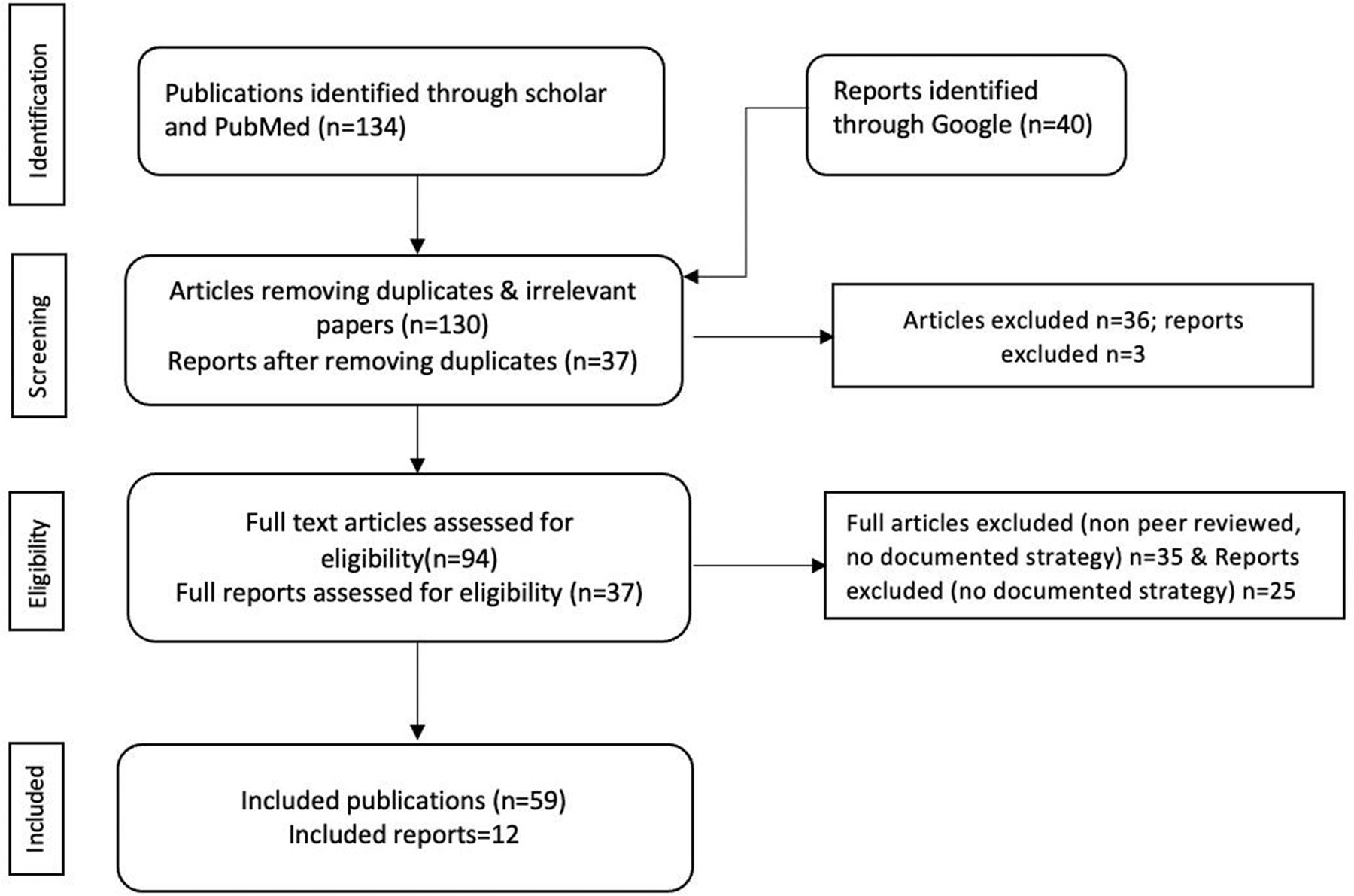
A total of 174 scholarly articles (134 publications and 40 reports) were identified by the search strategy, of which 59 peer-reviewed publications and 12 reports met the inclusion criteria and were reviewed in detail. The flow diagram (figure 1) summarises the steps to identify the publications and reports included in the review. Online supplemental table 4 represents the details of all papers and reports included and the findings.
Supplemental material
{kind=link}
Flow diagram of included publications.
Geoeconomic coverage of included publications/reports
The selected publications and reports covered six continents (Asia, Africa, North America, Europe, South America, Oceania). There are 32 countries, and of these 11 are high-income-countries, 2 are upper-middle-income, 13 are lower-middle-income and 6 are low-income-countries. Table 1 shows the countries’ corresponding gross domestic product per capita (US$).19
Countries included in the systematic review and the corresponding GDP
Testing strategies applied by different countries
Through content analysis, evidence was noted, demonstrating countries adopted diverse strategies to increase testing. These strategies are indicated in table 2 and summarised by income category in table 3 and by individual countries in online supplemental table 4. Notably, the strategies used were not exclusive, as some countries combined several strategies.
Thematic analysis of the different strategies used by the countries
Strategies by income country
The results are presented in the following seven thematic areas.
1. Increasing accessibility
Accessibility encapsulates the strategies countries adopted to ensure that the testing services had a wider geographical reach closer to the people and that whoever needed a test would be able to get it. Under this theme, most countries increased the number of laboratories available for testing, while others increased sample collection points and referral to the available laboratories. The frequency of using these strategies was high in low- and middle-income countries and low in high-income countries. The increment was gradual, with more laboratories being recruited to meet the demand during the pandemic. High-income countries introduced drive-through testing to bring testing closer to the people. Sample collection and referral was mainly deployed by the low-income and the lower-middle-income countries, while community-wide testing using community health workers was done by the middle-income countries. The high- and upper-middle-income countries increased testing rates by identifying the COVID-19 transmission hot spots in their countries and subsequently undertook mass testing. While the middle- and high-income countries could set up mobile testing units, this was not the case for the low-income countries.
2. Expanding and diversifying diagnostic platforms
Under this strategy, the diversity of diagnostics and testing modalities were considered. This included strategies that incorporated the use of RDTs, development of molecular tests, development and subsequent use of RDTs, repurposing manufacturing capacity to develop tests, community-wide testing with RDT and initiatives to support the production of diagnostics. Development of molecular diagnostics was undertaken in the high-income countries (South Korea, Germany, Singapore, USA) but not in the low- and middle-income countries except Vietnam, which reported producing a molecular diagnostic to increase testing. In a bid to increase testing, both high-income (South Korea, Chile, UK) and lower-middle-income countries (India, Bangladesh, Vietnam, Ghana) developed RDTs. Adopting RDTs increased the testing rates in these countries. Only one country (USA) reported repurposing manufacturing capacity to manufacture testing kits. Both high- and upper-middle-income countries carried out massive testing with RDTs.
3. Streamlining the regulatory and legislative landscape
Streamlining the regulatory and legislative landscape evolved in two ways: accelerating the manufacturing process and increasing the number of laboratories available for testing. Governments of high-income countries adjusted the regulatory and legislative frameworks to ensure the rapid development and the use of the developed tests. For example, the USA and South Korea deployed emergency use authorisation and saved the manufacturers from bureaucratic and administrative inefficiencies associated with the approval process for the diagnostics. The governments also linked test manufacturers with the clinical bodies to help fast-track the validation process. As a result, tests were readily available for use in a short timeframe. In Singapore, public–private partnerships were instrumental in ensuring the massive production of tests.
Governments also made regulatory and legislative adjustments to ensure more laboratories became available for COVID-19 testing. The added laboratories included the private, research and academic laboratories. This was noted mainly in the upper-middle-, lower-middle- and low-income countries. For example, France, brought private providers later in the pandemic to avoid the possibility of having non-harmonised reporting.
Also, as part of the regulations and strategies to attract private test developers, the high-income countries (USA, South Korea) deployed initiatives to interest private developers in manufacturing. Such initiatives included easing the approval processes and assurance that the governments would buy the developed kits.
4. Leveraging existing systems
The countries leveraged existing systems in two ways. One, using the current systems and frameworks to scale up the development of diagnostics and second, using the existing systems to incorporate COVID-19 testing.
High-income countries like South Korea leveraged structures established during the previous epidemics like Middle East respiratory syndrome (MERS) to be able to develop tests in a short time. Low- and middle-income-countries integrated COVID-19 testing within the existing disease systems to increase testing. The countries leveraged the testing systems available for other diseases like tuberculosis, HIV and influenza to embark on testing for COVID-19. In most of these countries, there were existing platforms for HIV viral load monitoring and Xpert MTB/RIF testing, which were leveraged to test for COVID-19. The integration also leveraged already set up systems to increase testing. For example, Nigeria leveraged the established polio systems to ensure the collection and transport of samples to the testing facilities.20
5. Human resource enhancement
Countries undertook human resource initiatives. Such initiatives included recruiting more health workers and increasing their capacity through training. Recruitment of more personnel happened mainly in the upper-middle-income countries, followed by lower-middle-income countries and then in the low-income countries. The trend was slightly different when it came to increasing capacity through training. The training was conducted mainly in the lower-middle- and low-income countries.
6. Creative use of technology and innovation
Countries such as South Korea and Ghana leveraged the technology to increase COVID-19 testing. South Korea was the first country to roll out a contact tracing and surveillance application to help increase testing. Ghana reported using a contact tracing application to increase testing. Ghana also increased testing by using drones to transport samples from the field to the testing facilities established. Furthermore, Ghana innovatively used pooled testing to increase the number of samples tested with limited kits. Only India reported undertaking health technology assessment (HTA) on a locally developed COVID-19 diagnostic, whereby they assessed the impact of an RDT on health systems in dimensions of efficiency, equity and quality guided by the HTA framework.21
7. Leveraging regional and continental networks
While most of the interventions happened at the country level, some of the efforts resulted from continent-wide collaborations led by the continental bodies. By far, the most extensive continental-led testing response was on the African continent, where the African Centres for Disease Control and Prevention (Africa CDC) increased testing across most African countries by building capacity through the provision of testing kits and training. In addition, through the Africa Task Force for Corona Virus and the Partnership to Accelerate COVID-19 testing, the Africa CDC helped increase testing. The Pan African Health Organisation (PAHO) led the efforts in South America and North America by ordering and providing test kits, conducting training and leveraging the national influenza centres to increase the laboratory network.
Discussion
This systematic review of strategies adopted to scale up COVID-19 testing has revealed strategies unique to some and common to all countries. We note that the choice of strategy was mainly driven by the previous outbreak management system to leverage the country’s income and manufacturing capacity. The adopted strategies fall under seven thematic areas: increasing accessibility, expanding and diversifying diagnostic platforms, streamlining regulatory and legislative landscape, leveraging existing systems, human resource enhancement, creative use of technology and innovation, and leveraging regional and continental networks.
The COVID-19 pandemic caught many countries unawares, irrespective of their income status. For example, in the USA and the UK, initial testing responses are marked by the absence of a clear testing strategy, defective tests and sluggish inclusion of private laboratories.22 23 These obstacles were later overcome; private and academic institutions were included and the categories of people prioritised for testing was expanded.23
Countries in a bid to avail tests to their people took on strategies to improve access. Most countries gradually increased the number of testing laboratories. This was largely done in the low- and middle-income countries and to a lesser extent in high-income countries. The high-income countries introduced drive-through/walk-in testing. The lower- and upper-middle-income countries undertook community-wide testing using community healthcare workers, a strategy supported by the decentralised nature of the healthcare system in most low- and middle-income countries. Countries like Zambia, South Africa, used community health workers with good results.24
In a bid to save resources, countries adopted the symptomatological approach to ration testing to only those exhibiting COVID-19 like symptoms. While this may have saved resources, it most likely missed many asymptomatic cases that are now thought to have driven the transmission of COVID-19. Both high-, middle- and low-income countries applied the approach, and gradually expanded the categories of individuals to test. High-income countries expanded testing faster than low- and middle-income countries though it is important to note that apart from contact tracing, test seeking is still largely driven by experience of symptoms. Despite healthcare workers being at the front line and the need to have them tested, the UK did not prioritise them until later in the pandemic.25 Whereas large economies like South Korea and Singapore opened up testing to everyone and did mass testing; several African, Asian and European countries across all income categories limited testing to the symptomatic and the high priority groups, and only expanded the categories later. This could largely have been due to the logistical challenges and the need to use the supplies available sparingly as it was hard for most of them to compete.24 26–29
Countries sought to expand and diversify the diagnostic platforms available for COVID-19 testing largely through the development and/or the adoption of molecular and RDTs. For the high-income countries, this was achieved through the development of molecular tests and RDTs, while for other countries, it was mainly through RDTs. All the molecular (reverse transcription PCR (RT-PCR)) diagnostics were developed in the high-income countries22 23 30–32 and this to some extent protected them from shortages of RT-PCR testing supplies that other countries had to contend with. RT-PCR testing required highly specialised laboratories that were few in most low- and middle-income countries. Some of these countries adopted RDTs in their testing algorithms as an interim measure. These were either imported or made from within. Some lower- and middle-income countries developed RDTs, and these helped increase testing21 33 and were gradually introduced in other low-income countries to boost testing.9 27 34
Some countries enhanced their regulatory and legislative landscape to maximise the number of tests within the shortest timeframe. High-income countries led the introduction of legislation mainly to increase manufacturing capacity, adoption of new diagnostic tests and accreditation of non-traditional facilities for involvement in testing COVID-19. In the USA, legislation to modify the regulatory framework governing laboratory developed tests led to more tests being introduced later.31 However, this came several months into the pandemic. The federal government was blamed for the bureaucracy that prevented the provision of tests by academic and private laboratories and product developers.35 In an emergency, an early response is the key, and lifting non-critical administrative barriers without compromising oversight can help expedite the delivery of vital products like diagnostics.36 As part of the regulation and licencing, countries included private, academic and research laboratories in the response.
There were differences in the engagement of private stakeholders between high-income countries and the low- and middle-income countries and the point at which they were engaged. While the high-income countries private sector was engaged in the early days of the pandemic as test developers,23 32 37 in the low- and middle-income countries, they were engaged in testing.38–43 In most of the high-income countries, the private laboratories were engaged in testing quite late.23 29 Countries called on academic institutions to support the testing efforts. This was noted across all countries that is, low-, middle- and high-income countries.44–46 The academic institutions in most countries have molecular platforms they use mainly for research purposes, and when leveraged could help supplement government level efforts to increase testing. Furthermore, most academic institutions in low- and middle-income countries have collaborative links with partners in the developed world. Such networks could have been leveraged to ensure the availability of kits for testing. Early in the pandemic, the UK engaged the academic institutions by asking them to avail their platforms for use in public facilities. This was later changed and instead the academic institutions were called on to do the testing.5
Countries also took advantage of available systems and previous experiences to mount responses to increase COVID-19 testing. While the high-income countries used prior experience to develop tests, the low-and middle-income countries leveraged the systems available to increase testing. The existing systems worked in favour of low- and middle-income countries as they could tap into these to effect testing. The PCR testing footprint within the disease programmes like tuberculosis (TB), HIV, influenza and schistosomiasis were used by most of the low- and middle-income countries.40 47–49 All they needed were supplies and the collaborations and donations helped with this.11 47 50 With most of the low- and middle-income countries accounting for the highest burden of TB,51 there have been progressive investments in diagnostics for TB and these have been leveraged for COVID-19 testing. Korea was able to rapidly develop testing kits by leveraging the test development strategy used for MERS.52
Human resources underpin most of the testing needed by the countries, as having equipment alone is not enough. As a result, countries recruited and trained more personnel.11 48 49 53 54 Recruitment of extra personnel was mainly reported by the upper-middle-income countries followed by the lower-middle-income countries, while the training of personnel was reported mainly by the lower-middle-income countries followed by the low-income countries. Human resource challenges in low- and middle-income countries have previously been documented,55 and the use of this as a strategy was possibly to meet the short falls in number available to run the COVID-19 tests. The recruitment and training of personnel were not noted in any of the high-income countries, possibly an indicator that these countries are not facing challenges of limited human resources for health.
Some countries were creative and innovative in their approach. To save the limited logistics, Ghana adopted pooled testing.33 Specimen pooling is a method of screening a large number of patients for an infection and typically involves combining multiple patient specimens into a single test tube than testing multiple samples in separate reaction tubes.56 This approach enabled Ghana to increase the number of tests done to the extent that in Africa they posted the highest number of tests done only behind South Africa.33
There were strategies at continental level, and these were overseen by the relevant bodies. By far, the greatest demonstration of continent-led efforts was in Africa where the African Centres for Disease Control and Prevention (Africa CDC) developed several response initiatives. Africa CDC demonstrated the need for harmonisation, solidarity and coordination at a continental level. They launched a joint continental strategy, the partnership to accelerate COVID-19 testing, purchased kits and equipped several African laboratories.11 50 African countries were outcompeted on the global supplies market and through the Africa CDC, pooled purchasing was implemented so that African countries competed as a block (as one large customer).47 Similar efforts are noted in South America where the Pan American Health Organisation oversaw country-level coordination, planning and monitoring. It mobilised experts and furnished countries with laboratory supplies for detection of the virus.57
The review has revealed that while the response was reactive, mostly trial and error in the early days of the COVID-19 pandemic, it yielded strategies that could be leveraged to support the implementation of evidence-based practices in the present and future epidemic–pandemic scenarios. We have noted how countries drew on the existing systems such as standard operating procedures used in responding to previous epidemics and/or refocusing manufacturing base to produce testing kits. The lesson that can be learnt from this is that preparedness is crucial to put systems in place that can be drawn on to effectively respond to disease outbreaks and epidemics. Testing was only part of the response that included clinical management of patients, contact tracing, quarantining, lockdowns to mention a few. This implies that preparedness should be holistic including health system strengthening (laboratory, clinical, referral system, disease surveillance, procurement and governance), socioeconomic empowerment of people and a flexible legislative and regulatory framework to enable rapid public health intervention in periods of health emergency.
The limitations of this review are that there might have been strategies adopted by other countries but were never published and thus did not appear anywhere in the searched databases. Further, the review only considered scholarly articles in English, and thus there might be under-representation of strategies used in the non-English-speaking countries.
Conclusion
All countries regardless of their income level had unique challenges associated with the scale-up of COVID-19 testing, and the review has revealed evidence that countries used different strategies to increase testing. While the low- and middle-income countries struggled to increase the testing rates as reflected by the low testing rates, they were able to post optimal testing rates because of experience in dealing with disease outbreaks and leveraging of the existing disease control programmes. The high-income countries in Europe and North America, despite their economic advantage, also struggled having enough tests available in the short term to medium term of COVID-19 pandemic. This was not the case in Asia where the high-income economies leveraged the previous disease outbreak experience like SARS, MERS to have in place diagnostics in a short period of time and quickly put in place effective testing strategies. Country’s epidemic handling experience, and manufacturing and financial landscape were critical in informing strategy to scale up testing. Learning lessons from the COVID-19 pandemic and strengthening health systems will equip the world to respond more effectively to any future pandemics.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data will be made available to others on reasonable request.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @winterzie
Contributors WM, WS, VS: conceptualisation, funding acquisition, project administration, data curation and formal analysis; WM, WS, BA-MO'H, VS, AR, BK, PT, MB: investigation, methodology and manuscript revision; WM: data curation, formal analysis and original draft writing. Overall guarantors: WM, WS. The guarantors accept full responsibility for the work and/or the conduct of the study, had access to the data and controlled the decision to publish.
Funding We acknowledge funding from the Scottish Funding Council/Global Challenges Research Fund grant (SMDO-XFC119) and the School of Medicine University of St Andrews that is funding Winters Muttamba’s PhD study.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.