Article Text

Abstract
Objectives The introduction of information and communication technology influences the work environment of large groups of employees in healthcare. In Sweden, a national healthcare service providing patient accessible electronic health records (PAEHR) has been deployed, and this paper investigates nurses’ expected effects of this implementation.
Setting Nurses associated with the Swedish Association of Health Professionals working in healthcare such as primary care, hospitals and midwives in Sweden. Before a full-scale national implementation of PAEHR, a web survey study was distributed nationally. The respondents represented all 21 Swedish regions. Questions included five-point Likert scale questions and open questions.
Participants A survey link was distributed via email to 8460 registered nurses, midwives and union representatives in Sweden. The response rate was 35.4% (2867 respondents: registered nurses 84%; midwives 6%; chief position 5%; in projects 2% and other 3%). Three reminders were sent out, all of them increasing the response rate. A majority of the respondents were female (89.9%), 8.4% male, whereas 1.7% did not indicate their gender. 31.4% were under 40 years old, 53.8% 40–59 and 13.7% over 60.
Results Data were analysed using exploratory factor analysis with principal component analysis as the extraction method. The analysis revealed three distinct factors related to nurses’ expectations of PAEHR: (1) PAEHR improves the quality of care, (2) PAEHR improves the quality of the work environment and (3) risk and fears concerning patients’ well-being. Some interesting results include that more experienced nurses are more favourable to PAEHR. Our analysis also shows that the view of the nurse–patient relationship is an essential underlying factor related to positive or negative expectations.
Conclusions Results show that the expectations and perceptions of PAEHR vary depending on the nurse’s view of who the electronic record belongs to. Younger nurses are somewhat more negative towards PAEHR than older nurses.
- human resource management
- health informatics
- information technology
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
A strength of the study is that it combines exploratory factor analysis and qualitative content analysis to understand nurses’ expectations of the impact of patient accessible electronic health records (PAEHR) in their work environment.
The data were collected using a large nationwide survey of nurses, midwives and union representatives in Sweden.
A limitation of the study is that there is no validated survey instrument to measure the effect of PAEHR on nurses’ work and work environment.
It is possible that the prevalence of specific expectations and experiences has changed since the data collection. However, it is less likely that it has affected to a similar degree the expectancy models.
Introduction
There is a worldwide shortage of nurses and a high rate of turnover.1 An important antecedent to nurse turnover is the quality of their working life. Some of the problems mentioned related to the quality of working life in the literature are high workload, control, responsibility, workload and unsatisfactory working conditions.2 Another factor in nurses’ decreased quality of working life is the increasing reliance on information and communication technology solutions in nurses’ work.3–6 There is an increased digitalisation and, for example, the number of patient services launched, which further affects nurses’ work environment. However, despite several benefits, digitalisation often has unexpected negative consequences in healthcare.5 7 8 .
Launching patient accessible electronic health records (PAEHR) has become a global trend. The trend is also reflected in the growing corpus of studies around the world, from the Nordic region8–10 and Australia11 to the USA, where both the OpenNotes12–14 and Blue Button15 initiatives have been studied extensively. Using the PAEHR services, patients can read medical documentation themselves. Many studies have shown that, in general, patients appreciate PAEHR services and use the information to recall what was decided during earlier medical visits, follow their care process and read test results.8 16 17
Whereas the launching of the PAEHR services has frequently been motivated by patients’ needs, the launch of PAEHR services also influences healthcare professionals’ work environment. In many cases, the launch of PAEHR has been a very controversial process.18–23 Healthcare professionals have expressed worries related to, for example, confusion among patients, increased workload and negative changes in documentation practices.17 24–26 A few studies look into the experienced effects of PAEHR on the nurses’ work environment in the short27 28 and the long run.29 These studies point to both positive and negative impacts on the work environment. The positive impact includes patients being more actively involved in their care and better cooperation between nurses and patients. The negative impact on the nurse’s work environment is an increased workload, especially through answering patient questions and new technical knowledge requirements related to PAEHR use.
However, up to this date, very few studies have investigated nurses' expected or anticipated effects of PAEHR. Two studies have looked into expected effects in emergency and psychiatry care nurses,28 30 but not the whole nursing profession. Expected or anticipated effects for nurses are interesting to understand since they affect the usage of the system when launched and can also influence the work environment through worries and uncertainty of what will happen. A better understanding of the expected effects of eServices can also contribute to future implementations of eServices for patients, both in Sweden and internationally.
Method
A questionnaire was developed in collaboration with the Swedish Association of Health Professionals (SAHP) to survey the attitudes and opinions of Swedish nurses regarding a nationwide implementation of a PAEHR service. The questions of the study were designed to measure the expected effects that nurses have related to the implementation of PAEHR and the effects on their work environment and work situation. The survey was developed based on earlier research on professional and patient perceptions of Swedish PAEHRs and eHealth technologies.31–33 The survey design is exploratory, and the instruments have not been validated in earlier studies. The survey was administered as a web survey and contained eight background questions and five sets of statements (in total 36 statements) on a 5-point Likert (from strongly agree to disagree strongly) scale with free text fields to each set. In the present study, 15 statements of the total 36 about the impact of PAEHR on nurses' work and working environment were analysed. The SAHP distributed the survey using their internal web survey tool to reach their members. The respondents were assigned codes starting from 1349XXXXX that refer to free-text comments used to illustrate respondents’ views and attitudes.
The survey was conducted according to the principles of the Helsinki Declaration. All answers are delivered anonymously to the researchers, and presentations are made on an aggregated group level.
A survey link was distributed via email in March 2014 (20140307–20140405) to 8460 registered nurses, midwives and union representatives in Sweden. The response rate was 35.4% (2867 respondents: registered nurses 84%; midwives 6%; chief position 5%; in projects 2% and other 3%). Three reminders were sent out, all of them increasing the response rate. 89.9% of the respondents were female, 8.4% were male and 1.7% did not indicate their gender. 31.4% were under 40 years old, 53.8% 40–59 and 13.7% over 60. All 21 Swedish regions were represented in the data.
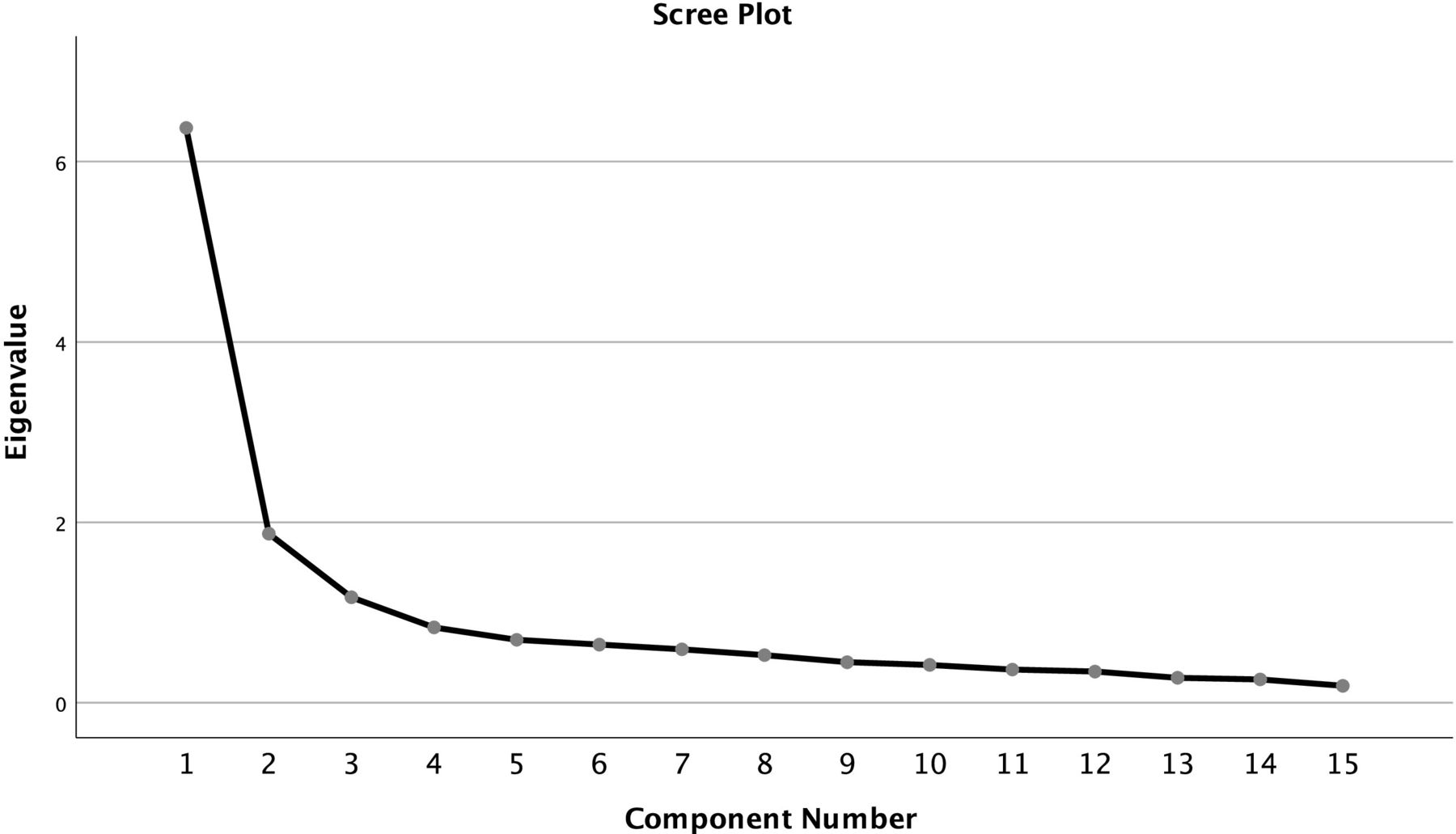
A preliminary descriptive statistics analysis was done to identify general trends in the data, see table 1. After the initial analysis, data were analysed using exploratory factor analysis (EFA) in SPSS V.25.0 using principal component analysis as the extraction method with varimax rotation. The data fulfil the commonly accepted criteria of EFA: N=2302, Kaiser-Meyer-Olkin Test of Sampling Accurac 0.915 and Sig. 000 Bartlett’s Test. For EFA, a three-factor solution (table 2) was selected based on the analysis of the Scree plot (figure 1) and the (non-)triviality of the factors. The solution explained 65.2% of the total variance. The chosen solution fulfils Hatcher’s (1994) recommendation of a 5:1 subject variable ratio. The variation of the factors and the contextual variables was tested using one-way Analysis of variance (ANOVA) with Tamhane post hoc tests.
{kind=link}
The screen plot determines the number of factors in the EFA. EFA, exploratory factor analysis.
Descriptive statistics (mean, SD) of the analysed statements
Results of the exploratory factor analysis (factor matrix with factor scores)
After conducting the EFA, free-text answers commenting on the statements were analysed qualitatively for a more in-depth understanding of the three factors by identifying patterns in answers from respondents scoring high (score >1.5) on each of them. The analysis was conducted iteratively by one of the authors, the preliminary results were discussed with all authors, turned into narrative descriptions of expectancy models (see below), and revisited and finalised after reaching a consensus in the group.
Patient and public involvement
This study did not include patient or public involvement.
Results
The factor analysis resulted in three different factors, which were interpreted as expectancy models, for example. different ways to relate to the expected reform of patient-accessible health records. The naming of the expectancy models was discussed among the authors with considerable experience in research on PAEHRS and decided when a consensus was reached. The three models are as follows: (1) embracing the reform, (2) being favourable to the reform with reservations and (3) being adverse to the reform. Individuals with a high factor ratio with these expectancy models were identified in the data set. Their free-text answers were analysed to better understand the different attitudes. Further analyses were performed to investigate the correlations of the expectancy models with varying background factors to see correlations between gender and the years worked as nurses. Below, we describe each expectancy model in detail.
Expectancy model 1: PAEHR improves the quality of care
High loading in items:
My work environment is positively affected by the introduction of PAEHR.
PAEHR increases the quality of care.
The quality of the documentation increases with patients’ access to PAEHR.
PAEHR will affect the content of the care meeting in a positive way.
PAEHR influences my contact with patients in a positive way.
PAEHR decreases the number of misunderstandings between patients and healthcare professionals.
PAEHR will give us more informed patients.
Patients’ compliance to treatment will increase as a result of their access to PAEHR.
PAEHR increases patient participation.
Unauthorised people will be able to read patients’ information through PAEHR (negative loading).
In expectancy model 1, the quality of care is in focus and is expected to increase with PAEHR. According to this model, the quality of care will be influenced positively. Quality is connected to the empowerment of patients, for example, by giving them a more participatory role. Meetings between healthcare staff and patients become more positive when patients are better informed. Quality of care is enhanced as misunderstandings are reduced. Patients’ compliance to different treatments is enhanced when decisions are made between two equal parties rather than dictated by the other. PAEHR is expected to disarm suspicion, increase openness and facilitate discussions with the patient, who has been able to better prepare for the visit.
Also, the quality of documentation itself is expected to increase with PAEHR. This expectation may be induced by the idea that today when we have an unequal relationship between healthcare staff and patients, healthcare staff may be less careful in their recording since it is only to be read by other healthcare staff in a similar exclusionary position. Perhaps they will need to improve when people who are the objects of these records can check their accuracy. All these positive aspects were expected to contribute to a better working environment. In this expectancy model, the possibility of unauthorised persons accessing the records was not seen as a particular risk.
Expectancy model 1 is the most positive to PAEHR, and several nurses who embodied this model were enthusiastic about the reform:
I think the suggestion is fantastic! In my opinion, it’s self-evident in patient-centred care. (Respondent 134933928)
Expectancy model 2: PAEHR improves my work environment
High loadings in items
My work environment is positively affected by the introduction of PAEHR.
PAEHR decreases the frequency of patient contact.
PAEHR contributes to lowering my workload.
PAEHR influences the content of the care meeting in a positive way.
PHAER impacts my contact with patients in a positive way.
Patients’ compliance with treatment will increase due to their access to PAEHR.
PAEHR decreases the number of misunderstandings between patients and healthcare professionals.
Expectancy model 2 is also favourable to PAEHR, and similar to model 1, in foreseeing better meetings between patients and healthcare staff: The content of the sessions will be better, misunderstandings will be fewer, patients’ compliance with treatment will be improved, and overall, contacts with patients are influenced positively by PAEHR.
However, in contrast to expectancy model 1, nurses’ workload is an essential item in expectancy model 2, while things related to the benefits to patients (participating and informed patients) are absent. Thus, the positive view on PAEHR is based on improvements in nurses’ work environment instead of patient empowerment. PAEHR is viewed positively because it is expected to lead to fewer misunderstandings, better compliance and fewer contacts with patients. As contacts with patients become more infrequent, the workload is reduced seems to the logic here. However, reduced contacts with patients can also be seen as a negative consequence of PAEHR as direct contact with patients might increase the quality of care. Rationalisation of work and excellent but effective patient meetings are the expected positive features of PAEHR.
However, this expectancy model does not look forward to PAEHR quite as enthusiastically as model 1. Following the view on PAEHR as means of improving effectiveness, some nurses scoring high with this model were concerned about its efficacy in their free-text comments and gave concrete examples of possible problems:
It is important that records from all healthcare providers can be in the same system, so the record is complete. (Respondent 134937198)
Some of the nurses scoring high with the expectancy model 2 were also concerned about online security. Besides, they expressed worries about the impact of PAEHR on different patients. The benefits of PAEHR for their work environment should not come with the cost of patient safety and integrity.
Model 2, thus, takes its point of departure in the current situation in healthcare. Possibilities of rationalisation are brought up, and concrete issues are based on everyday experiences that need to be solved to justify the rationalisation.
Expectancy model 3: risks and fears concerning patients’ well-being
High loadings in items
There will be an increased need to explain words or results of laboratory tests for patients.
Because of PAEHR, notes will be made outside the health record.
Your way of writing in the electronic patient records will change because of PAEHR.
Unauthorised people will be able to read patients’ information through PAEHR.
Expectancy model 3 sees PAEHR in negative terms. Interestingly, while nurses scoring high in expectancy model 2 were also worried about unauthorised persons accessing patient records, this was considered a concern in the complementary comments. At the same time, the Likert scale question did not feed into model 2. In model 3, it is one of the four misgivings that make up the core of this model and significant concern. Contrary to model 2, an increased workload is envisioned, as patients are expected to clarify what they read in their records.
In model 3, the introduction of PAEHR is expected to lead to record-keeping deterioration. The question on the Likert scale asks only whether the respondent’s way of keeping records will change. Still, the free comments reveal that this change is seen as unfavourable: Adapting the record to be read by a patient, who is seen as inexperienced, makes it less useful for professional communication. This model embodies expectations that parallel records are about to emerge. Increasing patient anxiety was also seen as an overarching negative effect.
The worst suggestion ever! Why? We can as well stop educating healthcare staff. There are so many reasons for not unleashing the records on the net. 1) Unnecessary anxiety about lab results when the patients don’t have the competence for what they read. 2) when there’s partner violence, for example, the woman can feel forced to show the record for next-of-kin, that’s not good if the next-of-kin is violent 3) patients are afraid to tell everything and staff is afraid of documenting everything. (Respondent 134933838)
The comments from nurses scoring high in expectancy model 3 mirror a view of a nurse–patient relationship, according to which nurses are sheltering and caring for a vulnerable and unknowledgeable patient. Giving the patient access to professional information would disturb this relationship. A concern for the status of one’s professional knowledge and position can also be discerned. Overall, comments from nurses scoring high with model 3 were highly negative.
Expectancy models, gender and professional age
Women are more likely to be aligned with expectancy model 3 than men (F(1,2263)=11.343, p<0.01), even when we controlled for nursing specialisation. We found no other gender effects.
Contrary to what might be expected, the longer nurses had worked, the more positive they were to PAEHR. A Jonckheere-Terpstra test (TJT) for ordered alternatives showed that there was a statistically significant trend of higher tendency to align oneself with the expectancy model 1 (TJT=746 3570.00, z=2.204, p<0.05) and the expectancy model 2 (TJT=7 57 4380.00, z=2.998, p<0.05) when a longer time (in years) had passed since getting a nurse legitimation. There was an opposite tendency to align oneself with the expectancy model 3 (TJT=6 55 8440.00, z=−4.280, p<0.001).
In particular, in model 2, with its practical concerns about PAEHR from both nursing and patient perspective, there is a significant difference between younger and older nurses: Those having had a nursing certificate for 0–5 years are less prone to be aligned with the expectancy model 2 than those with 20–29 or 30+years F(3,1956)=5.376, p<0.01. Hence, the concrete concerns of those nurses embodying model 2 are anchored in a long time nursing experience.
Whose record is it, anyway?
An analysis of the variance of the three expectancy models concerning the three items ‘Health record belongs to the healthcare provider’, ‘Health record belongs to the professionals’ and ‘Health record belongs to the patient’ illustrates concisely how the different expectancy models are based on different views of the patient–professional–provider relationship.
Those nurses aligned with model 1, with a strong emphasis on patient empowerment through PAEHR, are more likely to think that medical records belong solely to the patient and not to the healthcare provider or professionals responsible for the documentation (F(2,2243)=48.394, p<0.001).
The nurses aligned with the expectancy model 2 do not, either, think that the healthcare provider ‘owns’ the record instead of the patient (F(2,2243)=11.060, p<0.001). They are also more likely to think that it belongs to the patient than the professionals, but the difference is insignificant. Thus, there are different opinions in the expectancy model 2 group in this respect. In contrast to model 1 nurses, some of the model 2 nurses regard the health record primarily as their tool, even if they do not object to patients having access to it. Those nurses who are aligned with model 3 are more likely to think that medical records belong to the healthcare providers and professionals responsible for the documentation rather than the patient (F(2,2243)=9.409, p<0.001).
Discussion
The factor analysis revealed three different expectancy models concerning an anticipated introduction of a PAEHR service that would provide patients with easy access to their medical records. These models can easily be ordered on a positive to very negative scale, with one model at both ends of the scale and one somewhat on the positive side.
Our analysis shows that the nurse–patient (and doctor–patient) relationship is an essential underlying factor related to positive or negative expectations of PAEHR.34 The positive expectancy model 1 seems to be shared among nurses who already view the records as something that the patient owns, who argue for more patient empowerment to enhance healthcare quality and sometimes express irritation towards the current hierarchical healthcare–patient relationship.
The statements from nurses scoring high in expectancy model 3 mirror a view of a nurse–patient relationship, according to which nurses are sheltering and caring for a vulnerable and unknowledgeable patient. This can be seen as an example of a hierarchical healthcare–patient relationship. In this hierarchical relationship, healthcare workers decide about patients by virtue of their superior knowledge. We would argue that the underlying attitudes to patient empowerment, for example, seeing patients as collaborative partners in care, colour the expectations of PAEHR and expectations concerning technical and security issues. For example, the security risk of unauthorised persons receiving access to the records is acknowledged in both models. Still, while it is not seen as a significant problem in model 1, it is seen as a significant obstacle in model 3.
One interesting point to discuss is why younger nurses are somewhat unexpectedly more negative towards PAEHR than older and more experienced nurses. Contrary to what might be expected, the longer nurses worked, the more positive they were towards PAEHR. A feature in negative model 3 is worrying about one’s professional competence being questioned. While the most recently educated nurses should have been educated in a context where patient empowerment is a significant value, they are also the most inexperienced. They might be the most insecure about their position, making them more hostile towards their expertise being questioned. Thus, it might not be their relation to technology as such that decides their standpoint but instead their experience of being secure in their profession. However, more research is needed to further explore these results.
Model 2, the somewhat positive model, which also takes up some concerns, seems to regard electronic patient records as a new tool with no crucial influence on the relationship between patients and healthcare professionals. Here, the attitude to new technology is coloured by expectations and questions about how the tool could be modified to be practical and safe. This model was more often embraced by experienced nurses who have presumably experienced the arrival of several digital tools and their positive and negative contributions to nurses’ everyday work.
When looking into nurses’ expectations on the implementation of PAEHR some aspects of each expectancy model are confirmed by other studies. However, no previous study on nurses' expectations of the implementation of PAEHR present expectancy models. In expectancy model 1, the positive expectations on the work environment, and the positive influence on patient contacts are verified in an interview study with five nurses,27 and the increased efficiency expectation is verified in one large interview study with healthcare professonals.35 One example of a similar expectation presented is a documentation quality increase,35 increased trust35 and correctness of documentation.35 Very little of expectancy model 1 was found in two studies on nurses on psychiatry care and emergency care.28 30 Expectancy model 2 also has some support in the smaill interview study27 and a survey study on healthcare professionals (both nurses and physicians)35 related to positive effects on the expectations on better communication. The last expectancy model that reflects risks and fears concerning the implementation of PAEHR has strong support in all previous studies found.27 28 30 35 One large survey study points to the expectation that the content would change in the health record, for example.35 Previous studies have also highlighted security risk expectations,28 30 and altered documentation in the medical journal,30 35 which is confirmed in this study.
When comparing the PAEHR expectations of nurses in this study to the existing literature on the experiences after implementing such systems, one can note that the nurses’ experienced negative effects are not as big as originally feared.29 Typically, the introduction of this service has been heavily criticised by all healthcare professionals after the launch and welcomed by patients.19 21 36
One can conclude from this study that some nurses have negative expectations about the implementation of PAEHR. Such negative thoughts could be mitigated by informing about the patient’s implementation experience. Patients who access their records online are generally positive about the opportunity to read their records online.8 14 36 Informing about the reasons for patients’ reading could also be one way of mitigating the negativity. Patients read their records for numerous reasons, such as to have an overview of their healthcare visits, access test results and become more involved in their care.37 Patients report a better understanding of care plans14 and an increased sense of control in handling their health.8 37 Moreover, presenting recent research on patient participation could also mitigate negative expectations. This research includes that patients who are more knowledgeable and involved have more satisfactory health outcomes38 and are associated with lower costs.39 Another aspect to consider when implementing PAEHR is communication and different information channels.40 Finding efficient strategies for supplying information to various professional groups is essential.
This study has some limitations related to legal gender imbalance as the majority of the respondents were women. However, this legal gender distribution reflects the nursing profession in Sweden and is not surprising.
Expectations towards new technology should not be interpreted as concerning technology alone but in the context of broader attitudes and concerns, where technical experiences and professional experiences play a decisive role. These results align with the research on the general acceptance of technology41 and here verified in the context of PAEHR. Nurses have quite different expectations and perceptions related to this eHealth implementation. They vary depending on a view of whose record it is, view of patient empowerment, gender and age.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study followed the ethical recommendations for research studies in Sweden, but we did no ethical vetting as our institution does not require this. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are grateful to all respondents to the survey and the Swedish Association of Health Professionals administering the survey.
References
Footnotes
Twitter @AsaC
Contributors ÅC and IS did the conception and design of the study. IH and MS-K did the analysis and interpretation of the data and ÅC, IH, MS-K, TL and IS wrote the paper. ÅC, IH, MS-K, TL and IS contributed to the discussion of the results, finalising the manuscript, and approving the final manuscript. ÅC, IH, MS-K, TL and IS are all accountable for all aspects of the work, and ÅC is the guarantor of the work.
Funding This work was (partly) supported by NordForsk through the funding to Nordic eHealth for Patients: Benchmarking and Developing for the Future (NORDeHEALTH), project number 100477, and by AFA in the project System Development Methods for a Digital Work Environment (STRIA) grant number 180250.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.