Article Text

Abstract
Objectives Hospital-acquired pressure injuries (PIs) are a source of morbidity and mortality, and many are potentially preventable.
Design This study prospectively evaluated the prevalence and the associated factors of PIs in adult critical care patients admitted to intensive care units (ICU) in the UK.
Setting This service evaluation was part of a larger, international, single-day point prevalence study of PIs in adult ICU patients. Training was provided to healthcare givers using an electronic platform to ensure standardised recognition and staging of PIs across all sites.
Participants The characteristics of the ICUs were recorded before the survey; deidentified patient data were collected using a case report form and uploaded onto a secure online platform.
Primary and secondary outcome measures Factors associated with ICU-acquired PIs in the UK were analysed descriptively and using mixed multiple logistic regression analysis.
Results Data from 1312 adult patients admitted to 94 UK ICUs were collected. The proportion of individuals with at least one PI was 16% (211 out of 1312 patients), of whom 8.8% (n=115/1312) acquired one or more PIs in the ICU and 7.3% (n=96/1312) prior to ICU admission. The total number of PIs was 311, of which 148 (47.6%) were acquired in the ICU. The location of majority of these PIs was the sacral area, followed by the heels. Braden score and prior length of ICU stay were associated with PI development.
Conclusions The prevalence and the stage of severity of PIs were generally low in adult critically ill patients admitted to participating UK ICUs during the study period. However, PIs are a problem in an important minority of patients. Lower Braden score and longer length of ICU stay were associated with the development of injuries; most ICUs assess risk using tools which do not account for this.
Trial registration number NCT03270345.
- Adult intensive & critical care
- AUDIT
- PREVENTIVE MEDICINE
- Adult anaesthesia
Data availability statement
Data are available upon reasonable request. An online training module was developed for all clinical data collectors and was published on the study website (https://www.esicm.org/trials-group-2/decubicus/ online supplemental appendix A). See also Labeau S O, Afonso E, Benbenishty J, et al. Prevalence, associated factors and outcomes of pressure injuries in adult intensive care unit patients: the DecubICUs study. Intensive Care Medicine 2021;47:160-9. https://doi.org/10.1007/s00134-020-06234-9.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study ever completed to evaluate the impact of pressure injuries (PIs) in the adult population.
It is a robustly planned and executed study.
Limitations are mainly due to the low incidence and severity of PIs.
The inability to link preventive measures used in patients to the prevalence of PIs is also a limitation.
The study was conducted in the pre-COVID-19 era and majority of the patients were nursed in the supine position.
Introduction
In 2014, the UK National Institute for Health and Care Excellence (NICE) published a document for prevention and management of pressure injuries (PIs) in primary and secondary care in the UK.1 2 This document was revised in 2019 and states that ‘pressure ulcers are serious and distressing adverse events that can represent a failure of care’.3 PIs result when an area of the skin and/or the underlying tissues are damaged due to being placed under sufficient pressure for a period long enough to impair blood supply or when shearing forces generate friction on the skin during manual handling.1 2 An international classification categorises the injuries into stages 1–4, unstageable and suspected deep tissue injury according to the extent of tissue damage.3 4
Pressure ulcers caused by both moisture and shear stress are directly associated with the quality of care provided as well as patient outcomes.1–4 NICE guidelines2 state that PIs consume significant resources and that these should be preventable in the National Health Service (NHS), which has therefore employed tissue viability nurses (TVN) in the majority of hospitals. TVNs provide expert advice in the prevention and treatment of wounds including PIs.
Unfortunately, critically ill patients in intensive care units (ICUs) are extremely vulnerable due to the severity of their illness, immobility, sedation, poor tissue perfusion, hypoxia and frequent haemodynamic instability. The current prevalence of PIs in the UK ranges widely, with estimates from 4.7% to 32.1% in ward areas, while in the ICUs the prevalence is not known.2 5 6 The aim of this service evaluation was to provide up-to-date information on PIs within UK adult ICUs. The specific objectives were (1) to provide a picture of the prevalence of PIs in adult critically ill patients, specifically in relation to the presence of PIs on admission and PIs acquired within the ICU; (2) to provide the characteristics of PIs in terms of severity and anatomical distribution; and (3) to contribute data to the international Decubitus in Intensive Care Units (DecubICUs) study, of which this project formed a part.1
Methods
Study design and participants
This service evaluation was conducted using a single-day (midnight to midnight) point prevalence survey of all adult ICU patients. A full description of the methods can also be found in the DecubICUs global study report.1 The study was registered at ClinicalTrials.gov (NCT03270345).
Patient and public involvement
There was no patient and public involvement in this study.
Data collection
The study website provides the protocol and an electronic case report form (CRF; online supplemental appendix A and https://www.esicm.org/trials-group-2/decubicus/). Data were collected from all participating centres before the study day. Anonymous data were collected in the CRF on all adult patients present in the participating ICUs on 15 May 2018 (online supplemental appendix A). Admission data included patients’ demographic, type of ICU admission (ie, medical, elective or emergency surgical, or trauma/burns), principal diagnosis leading to ICU admission, mechanical ventilation on admission and whether the patient already had PIs at the time of ICU admission. Data included PI assessment, which included site and stage (generally referred to as ‘grade’ in the UK),3–6 and whether injuries were present at ICU admission (specifically these were areas exhibiting PIs, rather than discrete injuries; referred to as PIs for simplicity). Injury risk was evaluated using the Braden Scale.7 This scale combines six subscales (mobility, activity, sensory perception, skin moisture, nutritional state and friction/shear) and scores range from 6 to 23, with lower scores reflecting higher risk. Follow-up data gathered were survival status and length of ICU and hospital stay until hospital discharge, maximally at 12 weeks following the study day (7 August 2018). An online training module was developed for all clinical data collectors and was published on the study website (protocol available in online supplemental appendix A or online at https://www.esicm.org/trials-group-2/decubicus/; training module available online on the European Society of Intensive Care Medicine website at https://www.esicm.org/wp-content/uploads/2018/04/Module-DecubICUs-LR.pdf) prior to initiation in order to assist with consistency of data collection. Hospital and follow-up data were collected by clinical and research nurses and the site study coordinator. Individual patient data were collected by the bedside nurse by direct skin observation according to international staging definitions.3–6
Supplemental material
Statistics
Data were summarised as mean (SD) or median (IQR) as appropriate; categorical data were summarised as proportions (%). Overall PI prevalence was calculated as the proportion of the sample who had at least one PI on the study day. ICU-acquired prevalence was calculated as the proportion of the sample who had at least one PI determined to be acquired in the ICU present on the study day. Prevalence is reported as percentage with 95% CI.
Associations with ICU-acquired PI were explored using a mixed multiple logistic regression analysis with the logit link function and including a random intercept for site.
This method was chosen to balance potential effects resulting from variability in care processes across the participating sites. All demographic variables as well as those related to acute illness and chronic conditions were included. The variable ‘length of ICU stay before study day’ was included based on both clinical judgement and the literature on PI risk factors.8–10 As such, all variables were included following an exploratory approach, irrespective of their relationship with PI in univariate analysis.11 Results are reported as OR with 95% CI. Statistical analysis was performed using IBM SPSS for Windows V.26.0 and R statistical software V.3.6.1.12
Results
Ninety-four adult ICUs distributed across the whole of the UK participated in this study. In 2018, the Scottish Intensive Care Society Audit Group collected data from 72 adult ICUs,13 while the Intensive Care National Audit and Research Centre report was based on data from 263 NHS adult ICUs in the rest of the UK.14 The definition of an ICU can be broad; however, for the purpose of this study, the authors assumed that 28% (94 out of 335) of ICUs participated in this study in the UK; 51% declared themselves to be university-affiliated. The majority of ICUs were mixed medical and surgical (75; 80%), and the remainder were surgical of one type or another, with one specialist burns unit. Four participating units did not submit descriptive data. The ICUs had a median of 14 beds (IQR 10–20) and 68% declared themselves to be ‘closed’. There were six very large units with more than 40 beds.
Local investigators collected data from 1312 critically ill patients, the majority of whom were cared for in university-affiliated centres (67.3% of patients). The median nurse to patient ratio for the night shift on the survey day was 1:1 (IQR 0.8–1), reflecting the UK national standard of 1:1 nursing for level 3 patients (these are individuals requiring ventilatory and multiple organ support) and 1:2 for level 2 ‘high dependency’ patients. Only one hospital reported that neither physiotherapy nor dietetic support was available on the study day. Four units did not report on this specification. A list of the preventive measures used is provided in online supplemental appendix B tables 1 and 2. Four units reported that they did not have a section on the patient record for describing PI, and four units entered no data. Of the units, 59 (63%) employed the Waterlow Scale, 11 (12%) used the Braden Scale, 19 (20%) reported using a different PI risk assessment scale, and 1 unit reported not using a scale (4 units entered no data).
Supplemental material
The characteristics of the patients included in the study are shown in table 1; the majority were men (59.7%) and the median age was 62 years (IQR 50–72). The median number of days in the ICU before the study day was 4 (IQR 1–10), and 51% of these patients were requiring invasive mechanical ventilation on ICU admission. The source of admission to the ICU was the operating theatre in 34.2% of cases, followed by the emergency room (30.5%) and the general ward (23.3%). Of the patients, 992 (76%) were known to be alive at 84 days, with 271 (20.7%) known to have died (missing data on 49 patients).
Characteristics of patients
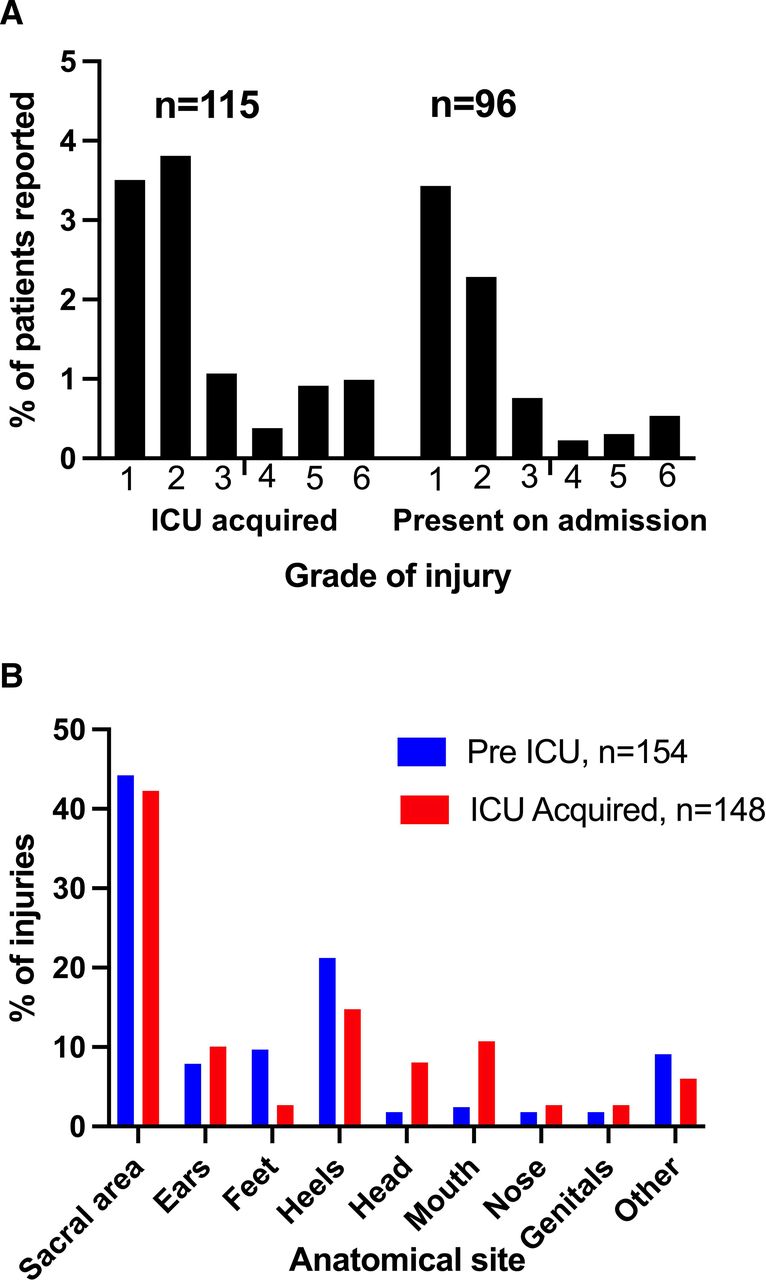
The total number of PIs was 311, of which 148 (47.6%) were acquired in the ICU and 154 (52.4%) prior to ICU admission. Thus, 54.5% of patients with PIs acquired their injuries following their ICU admission. Majority of the PIs were classified as grade 1 or 2 (figure 1A). Of the patients, 115 had ICU-acquired PIs and 96 had injuries that were pre-existing at the time of admission. The number of PIs per patient varied from one to nine sites. Anatomical site of 311 injuries (47.6% present priori to ICU admission) were acquired in the ICU and 163 (52.4%) were prior to ICU admission. The sacral area, along with the heels, mouth and nose, appeared the most vulnerable, with the sacral area and heels accounting for most of the higher grade injuries; of 97 areas with injuries classified as grade 3 or above, 33 (34%) were sacral areas and 28 (29%) were heels (figure 1B).
{kind=link}
(A) Grade of injury and (B) anatomical site of injury. ICU, intensive care unit.
The mixed multiple logistic regression analysis identified the following factors as independently associated with ICU-acquired PIs: decreasing Braden scores (OR=0.77 (95% CI 0.69 to 0.85), p<0.001) and increasing prior duration of ICU stay (0–3 days as reference; 4–6 days in ICU before study day, OR=2.29 (95% CI 1.06 to 4.95), p=0.03; 7–9 days in ICU before study day, OR=2.30 (95% CI 0.91 to 5.84), p=0.08; 10–12 days in ICU before study day, OR=7.77 (95% CI 3.42 to 17.69), p<0.001; >12 days in ICU before study day, OR=7.73 (95% CI 3.94 to 15.15), p<0.001; table 2).
Mixed multiple logistic regression model
Discussion
This service evaluation identified that 16% of 1312 patients in a large sample of UK ICUs had an area exhibiting pressure damage on the study day. Although 96 patients already had injuries on admission, 115 had acquired them during their ICU stay. Generally, these injuries were not severe; however, there were some that were, and these injuries come with a human and institutional cost. The impact of PIs is not easy to measure in terms of patient outcome and total cost. In 2004, the estimated annual cost paid by the NHS for treatment of PIs was between £1.4 billion and £2.1 billion a year. A more recent estimate suggests that the cost of treating a PI varies from £1214 (stage 1) to £14 108 (stage 4 more severe).2
Recently, Labeau et al1 conducted a worldwide, prospective, point prevalence study comprising 1117 ICUs in 90 countries and found 6747 PIs in 3526 patients. The proportion of ICU-acquired PIs was 59.2%. They identified several factors associated with ICU-acquired PIs, including older age, presence of organ support and high severity of illness scores. This analysis of the UK data identified a low prevalence of generally low severity of PIs. However, having a lower Braden score and a longer length of prior ICU stay were associated with a greater likelihood of acquiring a PI in the ICU. The global study (including data from many significantly lower resource settings) identified numerous risk factor associations, but the overall prevalence was greater (26.6%), as was the total sample (n=13 254).1 Importantly, the global cohort was able to identify that local factors, case-mix and especially the type of ICU admission (ie, medical, elective or emergency surgery) were associated with ICU-acquired PI risk.15
The locations of PIs were mainly the sacral area and the heels, and the more severe injuries tended to be in these areas. This clearly needs continuous focus on equipment and practice development and education, along with communication among the multidisciplinary team. It is a reasonable assumption that the overwhelming majority of the patients were nursed in the supine position on the study day; nevertheless, there were reported injuries to the nose, mouth and ears. The results might have been different had the study been conducted during the COVID-19 pandemic, during which there was a widespread need for nursing patients in the prone position.16–24 The prevalence and location of PIs likely would reflect staff experience and training, positioning of patients, and workload.21 The mouth and the nose may be damaged when using non invasive ventilation with limited options for interface or suctioning.23 The nurse to patient ratio was 1:1 for level 3 patients and this is a reflection of UK standards of good care. Due to limitations of the data collected, we cannot comment on the detailed acuity which contributing units experienced in the period running up to the study day. Similarly, we cannot infer that staffing has an impact on the prevalence of PIs; the impact of a period of inadequate staffing will be reflected in PIs sometime later.
The study sought information on preventive measures used.2 4 The NICE guidance does not cover the specific issues relating to the critically ill patient2–4; however, a list of preventive measures used in the ICUs is provided in online supplemental appendix B table 1. Data in this table are reflective of current NICE guidelines, but the lack of longitudinal data and the low prevalence of PIs precluded exploration of the relative effectiveness of such measures.
In the UK, the presence of ICU PIs generates a mandatory investigation generally initiated via adverse event reporting systems such as ‘Datix’ (https://rldatix.com). This triggers investigation and challenge but may not account the specific issues relevant to the critically ill. The ability to differentiate which PIs were preventable with appropriate measures and those which were not, due to acuity, nutrition, vasopressors, hydration status, etc, would ensure appropriate attention but cannot be evaluated with this study methodology. It has been acknowledged that some PIs, particularly in a critical care setting, are unavoidable.23
The mixed multiple logistic regression analysis identified decreasing Braden scores as associated with ICU-acquired PIs. The Braden Scale includes largely static factors, and a dynamic system which adjusts risk as time goes on may be worth evaluating. This is even more relevant given that prior length of stay has a significant association with the incidence of PIs demonstrated in both this and other studies.24 The development of such a scale including elapsed time as a variable would require an extensive longitudinal study; it is not currently clear whether the effort would be justified. Of note, the majority of sites reported using the Braden Scale or the Waterlow Scale; such scales would be the primary trigger for additional measures (online supplemental appendix B table 3); neither Braden or Waterlow has a notion of prior length of stay. The importance of length of stay has been highlighted previously, but this seems not to have translated into current risk assessment.25 Although better risk prediction can be valuable for comparative audit as part of quality improvement, we do not know if an improved risk prediction score would translate into fewer PIs.
One potential limitation of the study is the sample of ICUs contributing data; we estimate 28% of UK services contribute and we cannot assume this to be a representative sample. However, the site data submitted and the patient diagnostic data are in line with broader UK critical care (online supplemental appendix B table 2).26 Conceivably, participating sites may have had greater interest in PI or evaluative practice, which may be different from non-contributing sites, and be reflected in the quality of care. Finally, bedside nurses may perhaps have been inhibited from reporting injuries over anxieties that this would be regarded badly by managers. An important mitigation of this is that PI reporting is mandatory in the UK and has arguably become routine.
Conclusion
The prevalence and the stage of severity of PIs, both ICU-acquired and non-ICU-acquired, were low in adult critically ill patients admitted to UK ICUs. Nevertheless, 16% of patients had evidence of PI on the study day, and this clearly represents an opportunity for improvement. Decreasing Braden scores and increasing ICU stay were identified as risk factors associated with the prevalence of ICU-acquired PIs. The sacral area and the heels are clearly very vulnerable areas with greater numbers and are the sites of more severe injuries.
Data availability statement
Data are available upon reasonable request. An online training module was developed for all clinical data collectors and was published on the study website (https://www.esicm.org/trials-group-2/decubicus/ online supplemental appendix A). See also Labeau S O, Afonso E, Benbenishty J, et al. Prevalence, associated factors and outcomes of pressure injuries in adult intensive care unit patients: the DecubICUs study. Intensive Care Medicine 2021;47:160-9. https://doi.org/10.1007/s00134-020-06234-9.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was reviewed by the Joint Research Compliance Office at Imperial College Healthcare NHS Trust London and by the Health Research Authority. These bodies deemed the survey a service evaluation. All participating trusts/hospitals confirmed registration as a service evaluation according to their local protocols and non-objection from the relevant local Caldicott Guardian. A full description of the methods can also be found in the DecubICUs global study report.1 Participants gave informed consent to participate in the study before taking part.
Acknowledgments
This work was supported by the European Society of Intensive Care Medicine.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
FR and SB are joint first authors.
Twitter @frubulotta, @MiekeDeschepper
Collaborators UK Collaborating Site Investigators: Aberdeen Royal Infirmary (Aberdeen): Faye Morren; Buckinghamshire Healthcare Trust (Aylesbury): Charlotte Young; Ysbyty Gwynedd (Bangor): Nicola Vaughan-Jones; North Devon District Hospital (Barnstaple): Stephanie Harris; Furness General Hospital (Barrow-in-Furness): Karen Burns; Basildon Hospital (Basildon): Carmel Georgiev, Rosina Shayamano; Royal United Hospital Bath NHSFT (Bath): Ian Kerslake, Peter Creber; Bedford Hospital NHS Trust (Bedford): Ana Vochin, Catherine O’Brien; Belfast Trust (Belfast): Paul Caddell; Ulster Hospital (Belfast): Samantha Hagan, Mandy Hughes; Queen Elizabeth Hospital Birmingham (Birmingham): Tomasz Torlinski, James Sherwin; City Hospital (Birmingham): Santhana Kannan, Amber Markham; Blackpool Teaching Hospitals NHS Foundation Trust (Blackpool): Richard Lebon, Jason Cupitt; Royal Bournemouth Hospital (Bournemouth): Julius Cranshaw, Nigel White; Bradford Teaching Hospital (Bradford): Victoria Marriott, Wendy Milner; Brighton and Sussex University Hospitals (Brighton): Casiano Barrera Groba; Cambridge University Hospitals NHS Foundation Trust (Cambridge): Joao Azoia, Petra Polgarova; Kent and Canterbury Hospital (Canterbury): Shaly George, Ritoo Kapoor; Royal Glamorgan Hospital (Cardiff): Ceri Lynch; Broomfield Hospital GICU (Chelmsford): Nathalie Fox, Karen Cranmer; Broomfield Hospital St Andrews Burns Unit (Chelmsford): Natalie Fox; Cheltenham General Hospital (Cheltenham): Thomas Llewellym, Kelly Matthews; St Peter's Hospital (Chertsey): Louise Maltby, JowenaIbao; Countess of Chester Hospital NHS Foundation Trust (Chester): Karen Boulton, Rachel Jarman; Colchester Hospital (Colchester): Karen Baxter; Croydon University Hospital (Croydon): Ashok Sundai Raj, Arif Moghal; Ysbyty Glan Clwyd (Denbighshire): Joanne White; Doncaster Royal Infirmary (Doncaster): Suzanne Barrowcliffe; Dorset County Hospital (Dorchester): Mark Pulletz, Vaarisan Ganeshalingam; Western General Hospital (Edinburgh): Rosaleen Baruah; Royal Devon and Exeter NHS Foundation Trust (Exeter): Carole Boulanger, Helen Baker; Frimley Park Hospital (Frimley): Justin Woods, Poe Poe Ei; Medway Maritime Hospital (Gillingham): Vongayi Ogbeide, Paul Hayden; Royal Gloucestershire Hospital (Gloucester): Kelly Matthews; Bolton Royal Hospital (Greater Manchester): Jennifer Hughes, Madhu Balasubramanian; Royal Surrey County Hospital (Guildford): Armorel Salberg; The Princess Alexandra Hospital NHS Trust (Harlow): Rajnish Saha, Dagmar Holmquist; Wycombe Hospital (High Wycombe): Charlotte Young; Calderdale and Huddersfield NHS Foundation Trust (Huddersfield): Claire Derbyshire; Hull Royal Infirmary (Hull): Neil Smith, Elizabeth Stones; Ipswich Hospital NHS Trust (Ipswich): Jane Ademokun; West Middlesex University Hospital (Isleworth): Monica Popescu, Maria Schofield Legorburo; Jersey General Hospital (Jersey): Samantha North, Carole Brett; Queen Elizabeth The Queen Mother Hospital (Kent): Helen Jaundoo; Royal Lancaster Infirmary (Lancaster): Jayne Craig; St James University Hospital (Leeds): Simon Whiteley; Leeds General Infirmary (Leeds): Clare Howcroft, Liz Wilby; Royal Liverpool University Hospital POCCU (Liverpool): Peter Delve, David Shaw; Royal Liverpool University Hospital ICU (Liverpool): Karen Williams, Ingeborg D Welters; Liverpool Heart and Chest Hospital (Liverpool): Jane McMullen; Hammersmith Hospital GICU (London): Stephen Brett, Leah Flores; Hammersmith Hospital CICU (London): Treiza Trueman-Dawkins; Charing Cross Hospital (London): Francesca Rubulotta, Mae Templeton; St Mary's Hospital (London): John Adams; The Royal London Hospital (London): Catherine Smith, John Prowle; St Bartholomew's Hospital (London): Heather Byers, Andrea McDonnell; University Hospital Lewisham (London): Bernd Oliver Rose, Rosie Reece-Anthony; King's College Hospital NHS Foundation Trust (London): Luis Mendes; Chelsea and Westminster Hospital (London): Marcela Vizcaychipi, Rhian Bull; St George’s University Hospitals NHS Foundation Trust (GICU, London): Grace Lacaden, Eleanor Santiago; St George’s University Hospitals NHS Foundation Trust (CTICU, NICU, London): Carlos Castro Delgado, Sarah Farnell-Ward; University College Hospital (London): Elaine Thorpe; Macclesfield District General Hospital (Macclesfield): Justine Somerville, Anne Williams; Manchester Royal Infirmary (Manchester): Donna Cummings, Helen Derrick; Freeman Hospital (Newcastle): Sarah Brumwell, Claire Randell; Royal Victoria Infirmary Ward 18 (Newcastle upon Tyne): Nicola McCann, Emma Aves; Royal Victoria Infirmary Ward 38 ITU (Newcastle upon Tyne): Gillian Berry; Royal Gwent Hospital (Newport): Tamas Szakmany, Una Gunter; King's Mill Hospital (Nottingham): Paul Pulak; Nottingham University Hospitals NHS Trust (Nottingham): Nikki Sarkar, Kerry Wright; The Manor Hospital (Oxford): Vitor Gomes; Tunbridge Wells Hospital (Pembury): Jo Jones, Ruth Palfrey; Poole Hospital NHS FT (Poole): Julie Camsooksai; Queen Alexandra Hospital (Portsmouth): Abby Lewis, Antony Eneas; St Helens and Knowsley Teaching Hospitals NHS Trust (Prescot): Ascanio Tridente, Louise Barr; Queen's Hospital (Romford): Tomas Jovaisa, Beverley Thomas; Salford Royal NHS Foundation Trust (Salford): Emma Parkin, Daniel Horner; South Tyneside District Hospital (South Shields): Christian Frey; Royal National Orthopaedic Hospital (Stanmore): Suzanne Bench, Rachel Baumber; Stepping Hill Hospital (Stockport): Phil Broadhurst, Matthew Jackson; North Tees and Hartlepool NHS Foundation Trust (Stockton-on-Tees): Lynne Williams, Michele Clark; Royal Cornwall Hospital Trust (Truro): Jonathan Paddle, Sarah Bean; Mid Yorkshire Hospital (Wakefield): Sarah Buckley, Christopher Palfreeman; Warrington Hospital (Warrington): Sophie Liu, Nicola Allison; Warwick Hospital (Warwick): Ben Attwood, Penny Parsons; West Hertfordshire Hospitals Trust (Watford): Victoria Houghton, Sarah Jane Turner; Southend University Hospital (Westcliff-on-Sea): David Higgins, Egidija Bielskute; Royal Albert Edward Infirmary (Wigan): Nicola Horrigan; Wirral University Teaching Hospital (Arrowe Park Hospital) (Wirral): Reni Jacob, Karen Habgood; Queen Elizabeth Hospital (Woolwich): Ahmed Zaki, Amy Collins; Worthing Hospital (Worthing): Jenny Lord, Charalice Ramiro; Yeovil District Hospital (Yeovil): Agnieszka Kubisz-Pudelko, Michelle Kotze; Wrexham Maelor Hospital (Wrexham): Helen Williams.
Contributors FR, SBr, CB and BB were responsible for coordinating the study in the UKFR. SBr drafted the manuscript. MD, SOL and SBl produced a UK extract of data from the global study database. FR, SBr, BB, MD and SOL conducted the analysis. SOL and SBl were the lead investigators for the global study. FR is responsible for the overall content as the guarantor. All authors revised the manuscript for important intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.