Article Text

Abstract
Introduction Pancreatic cancer is a leading cause of cancer deaths worldwide. Screening for this disease has potential to improve survival. It is not feasible, with current screening modalities, to screen the asymptomatic adult population. However, screening of individuals in high-risk groups is recommended. Our study aims to provide resources and data that will inform strategies to screen individuals with new-onset diabetes (NOD) for pancreatic cancer.
Methods and analysis The United Kingdom Early Detection Initiative (UK-EDI) for pancreatic cancer is a national, prospective, observational cohort study that aims to recruit 2500 individuals with NOD (<6 months postdiagnosis) aged 50 years and over, with follow-up every 6 months, over a 3-year period. For study eligibility, diagnosis of diabetes is considered to be clinical measurement of haemoglobin A1c ≥48 mmol/mol. Detailed clinical information and biospecimens will be collected at baseline and follow-up to support the development of molecular, epidemiological and demographic biomarkers for earlier detection of pancreatic cancer in the high-risk NOD group. Socioeconomic impacts and cost-effectiveness of earlier detection of pancreatic cancer in individuals with NOD will be evaluated. The UK-EDI NOD cohort will provide a bioresource for future early detection research to be conducted.
Ethics and dissemination The UK-EDI study has been reviewed and approved by the London-West London and GTAC Research Ethics Committee (Ref 20/LO/0058). Study results will be disseminated through presentations at national and international symposia and publication in peer-reviewed, Open Access journals.
- pancreatic disease
- diabetes & endocrinology
- hepatobiliary tumours
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
United Kingdom Early Detection Initiative will generate the first UK cohort of individuals with new-onset diabetes, designed specifically with the intention of facilitating earlier detection of pancreatic cancer.
The study is designed to obtain pre-diagnostic data and biospecimens from pancreatic cancer patients and controls.
Prediagnostic samples and data will be generated for the validation of existing early detection biomarkers and for future biomarker discovery.
The study will apply health economic models to quantify the costs and benefits of detecting pancreatic cancer earlier in individuals with new-onset diabetes.
It is anticipated that approximately 1% of the cohort of 2500 individuals will have underlying pancreatic cancer, generating a limited number of case samples.
Introduction
Pancreatic ductal adenocarcinoma (PDAC) has the bleakest outlook in terms of survival of all common cancers. The current UK 5-year survival rate of 7.3% has improved only slightly in 40 years.1 2 Late disease presentation is the main contributor to high mortality rates, with approximately 85% of individuals not suitable for potentially curative therapy due to locally advanced or metastatic disease. Where surgery is possible, overall survival is significantly increased.3 Rapid intervention through earlier detection is key to improving prognosis. With a relatively low incidence rate, population-wide screening as a route to earlier detection is not justified for PDAC.4 Screening is recommended for select high-risk groups; however, this currently represents a minority (~10%) of cases.5 There remains a need to robustly characterise other high-risk groups for targeted screening strategies capable of capturing a larger proportion of cases.6
Approximately, 40%–65% of individuals with PDAC have diabetes at the time of diagnosis,7–10 with the majority being of new-onset (<3 years).8 10–13 Occurrence of diabetes in this setting is a paraneoplastic manifestation of PDAC,14 and individuals with new-onset diabetes (NOD) over the age of 50 are widely recognised as the highest risk group for PDAC.6 The prevalence of pancreatic cancer-related diabetes (PDAC-DM) in this group is approximately 1%.15 Consequently, screening all individuals with NOD is not feasible, as any test applied would require near-perfect specificity to avoid large numbers of false positives. Methods that enrich for PDAC-DM within the group of individuals with NOD are urgently needed to aid the development of new, practical screening strategies.
PDAC-DM is a form of type 3c diabetes (T3cDM), a classification that also includes chronic pancreatitis-related diabetes, as well as other aetiologies.16–18 T3cDM is associated with rapidly worsening glucose control and significant weight loss.10 12 19 Depending on study design, different estimates exist for the prevalence of T3cDM among those diagnosed with diabetes, ranging from 1.8% to 9.2%.16 20 21 Molecular biomarkers along with epidemiological and clinical characteristics that enable distinction of T3cDM, or PDAC-DM, among NOD could facilitate screening. To date, most studies aimed at identifying early-stage biomarkers of PDAC have used samples and associated data from patients already diagnosed with PDAC and are, thus, compromised by late changes during tumourigenesis that are not seen in early-stage disease. Tailor-made, prediagnostic cohorts are required to provide the necessary samples and associated data to support effective early detection pathways for this high-risk group.
The UK Early Detection Initiative for Pancreatic Cancer will generate a cohort of individuals with NOD, with the necessary clinical information and associated biospecimens to guide the development of a screening strategy for detection of PDAC-DM among NOD, ensuring its suitability within regional healthcare systems.
Methods and analysis
Study setting
The United Kingdom Early Detection Initiative (UK-EDI) Study is a national, prospective, observational cohort study, recruiting individuals with NOD aged 50 years and over to facilitate the development of screening pathways for PDAC. The study will align with a larger international effort, including studies in the USA22 and the European Union. The UK-EDI study is hosted by the Liverpool Clinical Trials Centre at the University of Liverpool.
Dates of the study
From 18 January 2021 to 31 March 2024.
Study design
The UK-EDI Study has seven work packages (WPs) centred on the establishment of the UK-EDI cohort (WP1, figure 1). Additional WPs include banking of blood samples to the standards of Good Clinical Practice (GCP) for laboratories (WP2), validation of existing promising biomarkers for their ability to distinguish T3cDM, including PDAC-related DM, from T2DM (WP3), interrogating epidemiological and demographic factors to further stratify risk of PDAC in the NOD population (WP4), undertaking new biomarker discovery (WP5), cost-benefit analysis (WP6) and managing and engaging stakeholders (WP7). The primary aim of the UK-EDI Study is to gather and interrogate key data to advance early detection of occult PDAC in the high-risk population of individuals with NOD.

UK Early Detection Initiative for Pancreatic Cancer (UK-EDI) Programme outline. NOD, new-onset diabetes mellitus; PDAC, pancreatic ductal adenocarcinoma; T2DM, type 2 diabetes mellitus; T3cDM, type 3c diabetes mellitus; WP, work package.
For pragmatic reasons, the UK-EDI study does not contain an imaging component. A similar trial underway in the USA, designed to improve detection of operable PDAC in individuals with NOD, includes an imaging arm.23 In that study, the Enriching New-onset Diabetes for Pancreatic Cancer (ENDPAC) algorithm risk stratifies individuals with NOD based on age and changes in both weight and diabetes parameters.23 Individuals with high ENDPAC scores are stratified to the intervention arm.
Eligibility criteria
Eligibility criteria and relevant definitions of the UK-EDI cohort are provided in table 1.
Eligibility criteria and relevant definitions of the UK-EDI cohort
Methods of participant identification
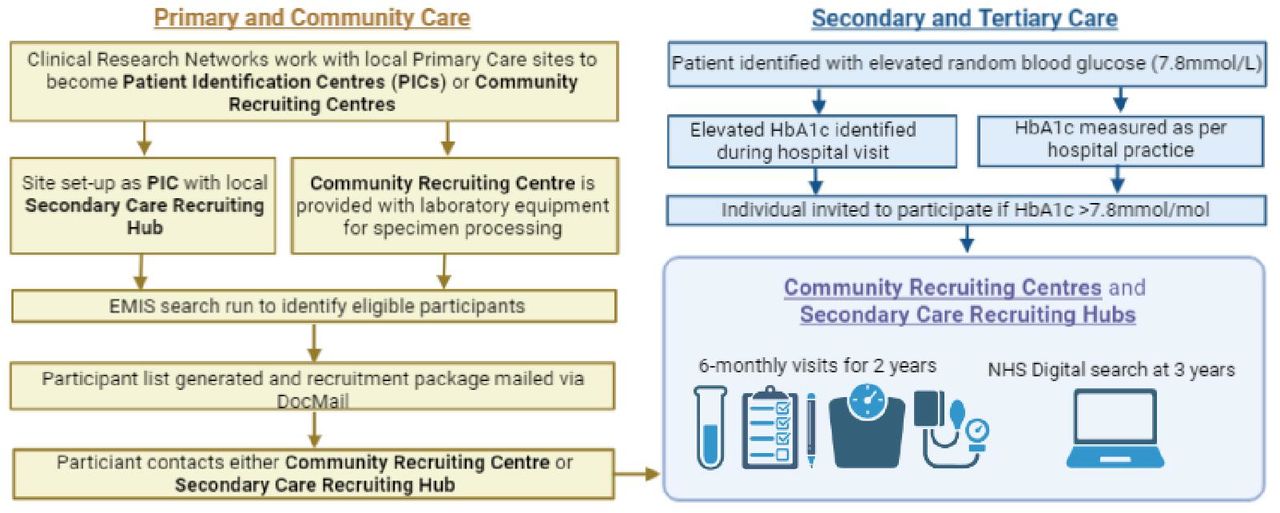
The UK-EDI Study will establish a nationwide cohort representative of the UK population with recruitment occurring across primary and secondary care settings, including specialist diabetes centres and primary care hubs. In an internal pilot study, we established pathways for identification of individuals with NOD from primary care, with recruitment in secondary care.24 In the UK-EDI study, participants will either be identified in primary care sites and recruited in the primary care setting or identified in primary care sites and recruited in a local secondary care recruiting hub. The use of electronic health records will facilitate 6 monthly identification of suitable participants in each setting. Participants may present directly to secondary care services as emergency presentations of NOD and those individuals will be recruited in secondary care. Participants may also be identified from specialist inpatient teams such as diabetes and endocrinology, hepatobiliary and pancreatic surgery, and gastroenterology. The screening framework is flexible to account for local organisation of services across the UK (figure 2).

{kind=link}
{kind=link}
Schematic of UK-EDI study recruitment and participant follow-up. EMIS, Egton Medical Information Systems (electronic healthcare record system); HbA1c, glycated haemoglobin; UK-EDI, UK Early Detection Initiative for Pancreatic Cancer.
Study timeline
Eligible individuals will be provided with a participant information sheet explaining the UK-EDI Study and will be given an opportunity to ask questions prior to signing an informed consent form. At the baseline visit, a full medical, drug and surgical history will be elicited, including demographic, social and anthropometric data. Participants will also be asked about a range of symptoms over the preceding 6–12-month period, which may indicate early signs of PDAC. Participants will be asked specifically about weight changes, including in the context of a weight management programme. Quality of life assessment will be via a health-related Quality of Life Questionnaire (EuroQol Research Foundation: EQ-5D-5L),25 and diabetes management will be captured via a Diabetes Self-Management Questionnaire (DSMQ).26 The DMSQ is an instrument which assesses diabetes self-care activities associated with glycaemic control. Blood samples will be taken for measurement of haemoglobin A1c (HbA1c) and research plasma and serum samples will be taken for biobanking according to GCP Laboratory standards to allow for translational research. Sites may also provide the results of other haematological and biochemical blood results including full blood count, liver function tests, urea and electrolytes, and lipid profiles, if these are being taken for routine diabetes care. Supplemental blood test results are not required for all participants.
Follow-up visits will be at 6, 12, 18 and 24 months after the baseline visit. Quality of Life, DSMQ and case report form data will be collected at baseline and each follow-up visit. At 36 months, there will be a search of NHS Digital to determine the number of events of PDAC diagnosis in the enrolled cohort.
Key clinical and translational characteristics, including timeframes, of the UK-EDI cohort are listed in table 2.
Eligibility criteria and relevant definitions of the UK-EDI cohort
Objectives
Primary
The primary objective is to recruit individuals to a bespoke standardised cohort of individuals aged 50 years or older with NOD (HbA1C ≥48 mmol/mol, (6.5%)) and no prior history of DM, ensuring the standardised collection and biobanking of samples while acquiring the molecular, epidemiological and demographic factors in order to advance the early detection of PDAC.
Secondary
The secondary objectives are to validate carbohydrate antigen 19-9 (CA19-9) and other novel markers already identified with potential to distinguish T3cDM (including PDAC related) from T2DM and to establish the economic impact of diagnosing PDAC early in individuals with NOD.
Exploratory
The opportunistic and exploratory objectives are to study molecular, epidemiological and demographic factors to further stratify risk of PDAC and to use the UK-EDI cohort for biomarker discovery.
Statistical methodology
Sample size
We aim to recruit 2500 patients with NOD aged 50 years and older, with a follow-up of 36 months. The target size of 2500 is pragmatic, based on costs and what is practically possible. It is anticipated that 0.8%–1% of the group will receive a diagnosis of PDAC in the 3-year follow-up time period.15
Thus, the UK-EDI cohort is expected to yield approximately 21–25 PDAC diagnoses (or 17–20 cases with 20% attrition). This study will provide data on the incidence of PDAC in individuals with NOD in the UK and will serve as the benchmark/reference point for future work.
Formal power calculations to determine associations between clinical/biological subgroups and the diagnosis of PDAC are difficult as it is not yet known what fraction of any subgroups will split the available patient population.
The UK-EDI cohort will contribute to larger international efforts aimed at determining the feasibility of detecting resectable PDAC in individuals over 50 years of age who are newly diagnosed with diabetes mellitus.23
Data analysis plan
The primary endpoint of interest is clinically diagnosed PDAC within 3 years of a new diagnosis of DM. The measurement of clinical characteristics, including glucose control (HbA1c) along with biological and epidemiological measures at five time points over the course of the cohort study, will help inform the incidence of PDAC in individuals with NOD in the UK.
Analysis of PDAC diagnosis will be performed using longitudinal methods, assessing the effect of biological and epidemiological markers while adjusting for relevant clinical characteristics.
Validation of biomarkers will include receiver operator characteristic curve analysis to determine biomarker performance characteristics. Further exploratory analysis will be carried out using multivariate techniques such as principal component and hierarchical cluster analyses in order to reduce the dimensionality of the data and identify naturally forming groups within the data, respectively.
Secondary analyses will focus on the time to detection of PDAC using a time-to-event approach. The probability of detecting PDAC will be calculated across subgroups using the method of Kaplan-Meier. Inclusion of biological and clinical characteristics will be incorporated using joint survival/longitudinal modelling techniques. Detailed information including clinical, epidemiological and biomarker data will be used to build a PDAC risk score, or validate emerging risk scores.
To assess the cost-effectiveness of early diagnosis of PDAC in individuals with NOD, the clinical pathway will be mapped and a literature review conducted to ensure that the model is populated with relevant current data. The study questionnaires will be used to update and calibrate models with data pertaining to PDAC cases versus controls. At the cohort level, a Markov model will be constructed to incorporate assumptions about what would happen to individuals if they were identified earlier. In addition, a discrete event simulation model will be developed to capture stochastic variations at the level of each individual. The impact of early diagnosis will be analysed using the updated Markov and simulation models. With respect to individuals detected earlier in a future screening protocol implemented in NOD, a key uncertainty is the stage of disease that would be diagnosed. A probabilistic sensitivity analysis, informed by the literature, will be conducted on a range of scenarios, including epidemiological, clinical and biomarker data.
Patient and public involvement statement
The Liverpool Pancreatic Patient and Public Involvement Group has contributed to the study conception and design and they have continued involvement in the management of this study. There are lay representatives on the Trial Steering Committee to ensure that the study remains both acceptable and relevant to patients.
Ethics and dissemination
Ethical approval
UK-EDI is approved by the UK Health Research Authority with favourable opinion granted by the London-West London and GTAC Research Ethics Committee on 14 February 2020. The details of this manuscript represent V.5 of the protocol approved on the 9 September 2021.
The study will be conducted in accordance with the Human Rights Act 1998, the Data Protection Act 2018, Freedom of Information Act 2000, the principles of GCP, the Declaration of Helsinki on biomedical research involving human volunteers (Hong Kong revision, 1989 and the 48th General Assembly, Somerset West, Republic of South Africa, October 1996, updated in October 2013) and the UK Policy Framework for Health and Social Care Research, where individuals agree to take part in the study, they will be informed of how data are recorded, collected, stored and processed, and that data may be transferred to other countries, in accordance with UK General Data Protection Regulations.
Data management considerations
Data Management will be through the Liverpool Clinical Trials Centre with delegated responsibilities for the University of Liverpool. The study has a dedicated Trial Manager, Data Manager and Trial Statistician and will be overseen by a Trial Management Committee and Trial Steering Committee. Data Management will be through the REDCap database and a dedicated Laboratory Information Management System (LIMS) within the GCP Laboratories at the University of Liverpool, linked by unique codes for each kit used at each time point from each patient, the code for which will be stored on REDCap and LIMS.
Dissemination plan
Study results will be disseminated through presentations at national and international symposia and publication in peer-reviewed, Open Access journals, where appropriate data will be made available via open-access repositories. We will work with charities, patient and public involvement groups and other relevant stakeholders to widely disseminate results and ensure that our findings are in an accessible format.
Ethics statements
Patient consent for publication
Acknowledgments
The authors are grateful for the support of all participants contributing to this study. Figures 1 and 2 were created with BioRender.com.
References
Footnotes
Twitter @UKEDI1
LO and MS contributed equally.
Contributors EC, LO, WG, CH, RVDM, LA, RT, TP, DP and PG conceived and designed the study. LO, MS and EC drafted this manuscript. RH, MS, EC, WG, RJJ, CH, WR and VC-G drafted the study protocol. RJ is responsible for statistical design and analysis. EC is chief investigator. All authors contributed to the final manuscript and agreed to all of the content of the submitted manuscript.
Funding This work is supported by Cancer Research UK, grant number C7690/A26881.
Competing interests EC, LO, WG, CH and PG are named as inventors on GB patent GBGB1806002.0; PCT/GB2019/050998, submitted by the University of Liverpool, that covers the measurement of adiponectin and IL-1Ra as a biomarker for early detection of pancreatic cancer.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.