Article Text

Abstract
Objective To compare real-world effectiveness and safety of direct oral anticoagulants (DOACs) in patients with nonvalvular atrial fibrillation (AFib) for prevention of stroke.
Study design and setting A comparative cohort study in UK general practice data from The Health Improvement Network database.
Participants and interventions Before matching, 5655 patients ≥18 years with nonvalvular AFib who initiated at least one DOAC between 1 July 2014 and 31 December 2020 were included. DOACs of interest included apixaban, rivaroxaban, edoxaban and dabigatran, with the primary comparison between apixaban and rivaroxaban. Initiators of DOACs were defined as new users with no record of prescription for any DOAC during 12 months before index date.
Primary and secondary outcome measures The primary outcome was stroke (ischaemic or haemorrhagic). Secondary outcomes included the occurrence of all-cause mortality, myocardial infarction (MI), transient ischaemic attacks (TIA), major bleeding events and a composite angina/MI/stroke (AMS) endpoint.
Results Compared with rivaroxaban, patients initiating apixaban showed similar rates of stroke (HR: 0.93; 95% CI 0.64 to 1.34), all-cause mortality (HR: 1.03; 95% CI 0.87 to 1.22), MI (HR: 0.95; 95% CI 0.54 to 1.68), TIA (HR: 1.03; 95% CI 0.61 to 1.72) and AMS (HR: 0.96; 95% CI 0.72 to 1.27). Apixaban initiators showed lower rates of major bleeding events (HR: 0.60; 95% CI 0.47 to 0.75).
Conclusions Among patients with nonvalvular AFib, apixaban was as effective as rivaroxaban in reducing rate of stroke and safer in terms of major bleeding episodes. This head-to-head comparison supports conclusions drawn from indirect comparisons of DOAC trials against warfarin and demonstrates the potential for real-world evidence to fill evidence gaps and reduce uncertainty in both health technology assessment decision-making and clinical guideline development.
- cardiology
- health policy
- primary care
- stroke medicine
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study performed head-to-head comparisons of direct oral anticoagulants rather than relying on indirect comparisons of trials with different designs.
This study used routinely collected data from electronic health records within a nationally representative UK database with good data recording and follow-up time.
Treatment assignment was not randomised; however, after propensity score matching, treatment groups were similar across 40 measured demographic and clinical characteristics, suggesting comparability between exposure groups.
Robustness of primary findings via propensity score matching was contextualised by use of alternative balancing approaches in sensitivity analyses, including propensity score weighting and high dimensional propensity score matching.
We did not link to secondary data for stroke outcome ascertainment but reporting of stroke and other conditions in the general practice record is incentivised by the Quality and Outcomes Framework.
Introduction
In the UK, atrial fibrillation (AFib) affects 1.4 million patients,1 and between 0.9% and 1.6% of the UK’s National Health Service spending is attributable to AFib, predominantly from hospitalisations.2 The condition is associated with significant complications, including stroke—nonvalvular AFib increases an individual’s risk of stroke by five times,3 and between 20% and 30% of stroke cases are attributed to AFib.4
Anticoagulants, including vitamin K antagonists (VKAs) and direct oral anticoagulants (DOACs), are highly effective in the prevention and treatment of thromboembolic events associated with AFib. Nevertheless, VKAs like warfarin require frequent coagulation monitoring due to their narrow therapeutic index and have multiple drug and food interactions. Alternatively, DOACs inhibit coagulation via direct and specific binding to active sites of thrombin (eg, dabigatran) or factor Xa (eg, apixaban, rivaroxaban and edoxaban) of the coagulation pathway. Compared with VKAs, DOACs have a wider therapeutic index, which permits use in fixed doses without coagulation monitoring, and relatively limited drug and food interactions. DOACs are the preferred anti-coagulants for patients with nonvalvular AFib in the UK.5 The safety and efficacy of DOACs compared with VKAs for stroke prevention in patients with AFib have been established in randomised clinical trials (RCTs).6 7 However, head-to-head RCTs of DOACs (eg, apixaban vs rivaroxaban) are not available, and relative safety and efficacy findings are based on indirect comparisons from network meta-analyses (NMA).7–9
Agencies, like the National Institute for Health and Care Excellence (NICE), evaluate the comparative effectiveness and cost-effectiveness of therapies to inform both reimbursement decisions and clinical guidelines. Between March 2012 and September 2015, NICE separately assessed and recommended four DOACs for stroke prevention in AFib: dabigatran, rivaroxaban, apixaban and edoxaban. Because no direct comparisons of DOACs were available, NICE’s decision-making, which impacts patient health and clinical practice was based on RCTs of DOACs compared with warfarin and indirect comparisons to other DOACs. A NMA of indirect comparisons ranked rivaroxaban as the best DOAC for reducing myocardial infarction (MI) and all-cause mortality, while apixaban was ranked best for minimising the risk of bleeding and dabigatran was ranked best for reducing the rate of stroke.5 However, the NMA rankings had probabilities that varied from 60% to 80% and most of the head-to-head ORs approached the null and/or had wide confidence intervals leading NICE to interpret the findings with caution. NICE noted heterogeneity among the trials on which the indirect comparisons were based, which limited the ability to differentiate between DOACs’ effectiveness. These uncertainties were reflected in NICE’s Atrial fibrillation: diagnosis and management guideline5 where NICE decided to not recommend one DOAC over the others, but instead emphasised treatment should be personalised based on the patients’ needs and preference.
Comparative effectiveness analysis in real-world data (RWD) has emerged as a potential strategy for supplementing clinical trials and for generating evidence on the effectiveness of products after launch.10 There is a growing body of literature that has duplicated AFib RCT results in RWD,11 12 which increases confidence in RWD studies that directly compare DOACs in RWD. However, there is heterogeneity in the results of RWE studies that directly compare DOACs. For example, a Scottish study in AFib patients found no differences between DOACs for stroke prevention.13 These findings align with a French and Danish RWE study in nonvalvular AFib patients14 15 but differ from a US-based study of Medicare patients with AFib, which found an increased risk of stroke for rivaroxaban patients compared with apixaban patients.16 All-cause mortality findings are also mixed, with one study finding no difference between apixaban compared with rivaroxaban14 and others finding increased mortality with rivaroxaban compared with apixaban13 16 and dabigatran.15 Only the French and Danish studies restricted to nonvalvular AFib14 15 and the US-based study16 was in patients >65 years old. Thus, it is unclear how generalisable these findings are to patients with nonvalvular AFib in the UK.
The objective of this study was to evaluate the comparative effectiveness and safety of the DOACs available in the UK (apixaban, rivaroxaban, edoxaban and dabigatran) through direct comparisons among adults with nonvalvular AFib at risk for stroke in the UK.
Methods
Study design and objectives
We conducted an RWD cohort study to compare the rate of stroke among patients with nonvalvular AFib initiating DOACs, specifically, apixaban, rivaroxaban, edoxaban and dabigatran. Following the steps outlined by Gatto et al17, we articulated the research question, conceptualised the underlying hypothetical target trial,18 identified a fit-for-purpose data source, and posted the final protocol publicly on the EU PASS Register of the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (EUPAS45073) prior to implementing the study.
Data source
This study used anonymised patient data from The Health Improvement Network (THIN) Database (A Cegedim Proprietary Database). The THIN Database is a primary care research database containing anonymised electronic health record data from around 850 UK general practices using the VISION clinical system (since 1994) and contains records for around 20 million patients. The THIN database has been well described, and the quality of data collection has been documented in multiple studies.19 20 THIN has also been shown to be representative of the UK population with respect to demographics, major condition prevalence and mortality rates.21
Study population and treatment
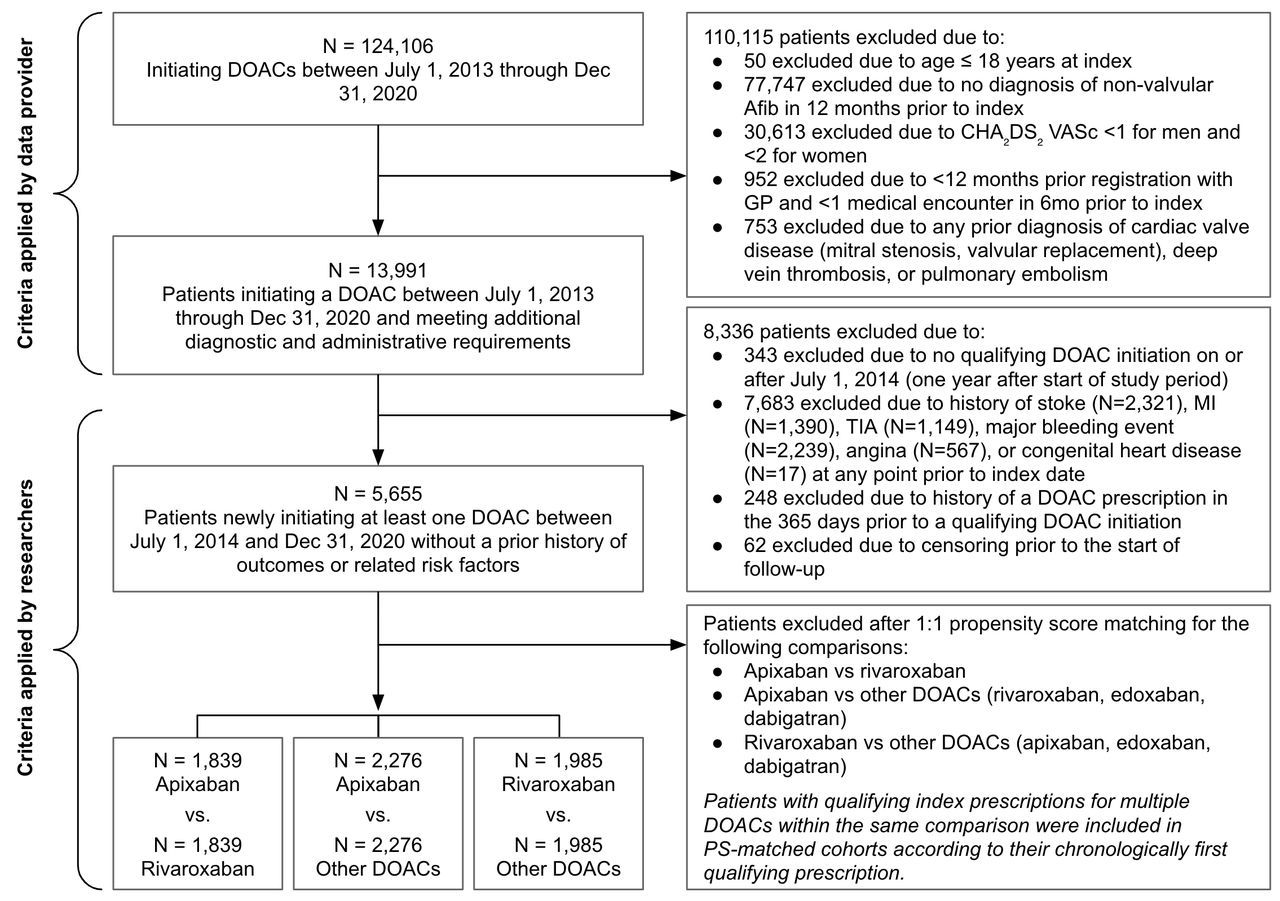
We identified adults (≥18 years) with nonvalvular AFib newly initiating apixaban, rivaroxaban, edoxaban or dabigatran (with a 365-day washout for any prior DOAC use) between July 2014 and December 2020 (figure 1). Index date was assigned as the date of first qualifying treatment initiation. Patients were required to have at least one medical encounter in the 180 days prior to study index date, be at risk of stroke (general practitioner (GP) assessed CHA₂DS₂ VASc >1 for men and >2 for women), have no recorded history of study outcomes and have no prior diagnosis of cardiac valve disease, deep vein thrombosis, pulmonary embolism, angina or congenital heart disease. History of congenital heart disease was an exclusion criterion because it is linked to valvular heart disease. Exposures of interest were defined by corresponding Anatomical Therapeutic Chemical (ATC) codes (online supplemental figure 1; online supplemental files 1 and 2).
Supplemental material
Supplemental material
Supplemental material

Study population for completed comparisons. DOACs, direct oral anticoagulants; GP, general practitioner; MI, myocardial infarction; PS, propensity score; TIA, transient ischaemic attack.
The primary comparison of interest was apixaban initiators versus rivaroxaban initiators, the two most commonly prescribed DOACs in the UK.22 Additional comparisons considered and completed are detailed in table 1. Patients with qualifying DOAC prescriptions from both medications or medication groups being compared (<0.5% of patients with qualifying prescriptions) were indexed according to the chronologically first qualifying prescription.
Head-to-head comparisons considered and completed
In the primary comparison, subgroup analyses were conducted by age group (<75 years vs ≥75 years), by CHA2DS2 VASc score (0–1, 2–3, ≥4), by gender, and among patients with vs without each of the following: concomitant aspirin use, prior warfarin use, diabetes mellitus and heart failure.
Outcomes
The primary outcome was stroke (ischaemic or haemorrhagic). Secondary outcomes included all-cause mortality, MI, transient ischaemic attacks (TIA), major bleeding events and a composite of angina/MI/stroke (AMS). Major bleeding was defined as a composite of major intracranial (including haemorrhagic stroke), gastrointestinal and urogenital bleeds. Study outcomes were defined by corresponding Read Medical Codes and mapped International Classification of Disease, 10th version (ICD-10) diagnosis codes at the primary care setting (online supplemental files 1 and 2).
Covariates
Covariates included in the propensity score (PS) model (described below) included age, gender, CHA2DS2 VASc score,23 year of treatment initiation and history of a number of diagnoses and treatments (see list in table 2). CHA₂DS₂ VASc score was estimated using patient history (online supplemental file 2) because the GP-assessed CHA₂DS₂ VASc was not available at time of analysis due to data availability constraints. All covariates were determined based on the literature and clinical knowledge regarding their relationship to the primary and secondary outcomes of interest.
Baseline characteristics of patients with nonvalvular atrial fibrillation newly initiating a DOAC, before and after propensity score matching
Medication use was identified by ATC codes and assessed in the 12 months prior to and including the index date. Comorbidities were identified by Read Medical Codes and mapped ICD-10 diagnosis codes and were assessed over all available data prior to and including index date. Patient demographics were measured on the index date. High missingness (34%–98% missing; online supplemental table 1) in diagnostic assessments meant that we dropped some covariates that we planned to include in the PS models. This included marital status, cigarettes per day, alcohol glasses per day, body mass index, hemoglobin A1c (HbA1c), international normalised ratio, glomerular filtration rate and creatinine clearance as measures of renal function. Remaining covariates were assessed dichotomously based on the presence or absence of diagnostic or medication codes in the patient history. Patients were assumed to have had a diagnosis or prescription of the relevant code(s) was found among their records. Otherwise, it is assumed that the patient did not experience the event or was not prescribed the medication, thus resulting in no missing data for these variables. Additional dichotomous characteristics considered for inclusion in the PS model (eg, sepsis) capturing few (<1%) exposed or unexposed patients were not included in analytic models. See online supplemental file 2 for definitions of all covariates included in PS models.
Supplemental material
The 1-year baseline period specified in the study protocol (EUPAS45073) for capture of baseline comorbidities was expanded to all prior available data after an observed under-capture of comorbid conditions (eg, hypertension) in baseline using the 1-year baseline period. Results corresponding to the protocol-specified 1-year baseline are reported in online supplemental tables 2 and 3.
PS matching
We used PS matching between exposure groups using 1:1 nearest neighbour matching without replacement (± a calliper of 0.01 of the PS). The PS model included a priori selected covariates assessed prior to treatment index, accounting for over-fitting, positivity violations and covariate instability.24
Diagnostic phase
In order to progress to the inferential analysis phase, each primary and secondary comparison had to pass a series of diagnostic checks (masked to treatment specific outcomes) including: positivity of variables, baseline confounder balance (an absolute standardised difference (ASD) ≤ 0.1),25 sufficient population-level persistence on treatment (median persistence at least 1 year), and confirmation that models were not overfit (≥12 exposed patients per covariate). Adequacy of sample size was also assessed, but insufficient sample size per pre-specified power requirements did not preclude estimation,26 as long as each PS matched comparator group had at least 500 patients. Comparisons passing all diagnostic criteria included apixaban versus rivaroxaban, apixaban versus other DOACs (rivaroxaban, edoxaban, dabigatran) and rivaroxaban versus other DOACs (apixaban, edoxaban, dabigatran).
Pre-specified inferential analysis
In the inferential phase, we executed Cox proportional hazards regression models to estimate HR and 95% CI after PS matching in the overall cohort and within each subgroup of interest. The incidence of stroke and secondary outcomes were assessed for the primary comparison of apixaban vs rivaroxaban. Incidence of stroke was compared for all secondary comparisons. Patients were followed in an ‘intention to treat’ (ITT) approach starting from the day after their index date. In analyses of stroke, MI, TIA, major bleeding events and AMS, patients were followed until the end of the study period (December 2020) or the first occurrence of the outcome, death or date of last contact with GP. In the analysis of all-cause mortality, follow-up was extended beyond the date of last contact to the date of a death if the death occurred within 90 days of a patient’s last contact in order to capture deaths reported after a patient’s last contact with their GP. Secondary analysis of the primary outcome in the apixaban versus rivaroxaban comparison included an ‘as-treated’ approach where in addition to the ITT censoring criteria, patients were censored on termination of exposure, crossover of exposure group, or addition of another DOAC. The exposure termination date was defined as the end of the last continuous prescription (allowing for up to 30-day gaps between end of previous and start of next prescription) plus a 30-day risk window.
Pre-specified sensitivity analysis
To evaluate the robustness of our findings, high-dimensional PS (HdPS) analysis was used to estimate the association between treatment with DOACs and the primary and secondary outcomes. The HdPS approach is a seven-step algorithm that empirically identifies a pool of covariates from different data dimensions (eg, diagnoses, procedures, medications) based on their prevalence and then selects a subset of the covariates for inclusion in a PS model based on their potential to bias the exposure-outcome association.27
Post-hoc analysis
Additional post-hoc analyses were conducted to further contextualise the study findings. Glaucoma, a condition not impacted by DOAC use, was assessed as a negative control outcome to assess the possibility of residual confounding after PS matching.28 Inverse probability of treatment weighting (IPTW) and standardised mortality ratio weighting (SMR) methods were used to evaluate potential treatment effect heterogeneity in estimates of effect for primary and secondary outcomes and the robustness of results.29 Primary analysis findings were additionally assessed by gender.
All data analyses were conducted using Aetion Evidence Platform V.4.45 (2021), software for RWD analysis. Aetion, Inc. https://www.aetion.com.
Patient and public involvement
There was no patient or public involvement in this study, including development of the research questions, selection of outcome measures, study design, conduct or dissemination of findings.
Results
Out of a total of 5655 patients with new use of at least one DOAC before PS matching (figure 1), 2801 initiated apixaban, 2221 initiated rivaroxaban, 398 initiated edoxaban and 261 initiated dabigatran and met the criteria for inclusion (table 2).
Primary comparison: apixaban versus rivaroxaban
A total of 2221 rivaroxaban and 2801 apixaban patients were eligible for inclusion in PS-matched groups. Before PS matching, the apixaban group was more likely to initiate treatment after 2017 and more likely to be woman compared with rivaroxaban patients (table 2). After 1:1 PS matching, 1839 patients with apixaban and 1839 patients with rivaroxaban were identified (figure 1). Differences in covariate prevalence were minimal, with ASD below 0.1 for all characteristics (table 2). Due to sample size constraints, stratified analyses by dosage were not completed; dosages of index prescriptions are reported in online supplemental table 1. Median follow-up time in the ITT analysis was 845 days [IQR 340, 1368] in the apixaban group and 779 days [322, 1284] in the rivaroxaban group (online supplemental table 4). In the ‘as-treated’ approach, median follow-up time was shorter compared with ITT and longer in apixaban compared with rivaroxaban (506 days vs 412 days). Rivaroxaban patients were more likely to be censored for switching to another DOAC compared with apixaban patients (online supplemental table 4).
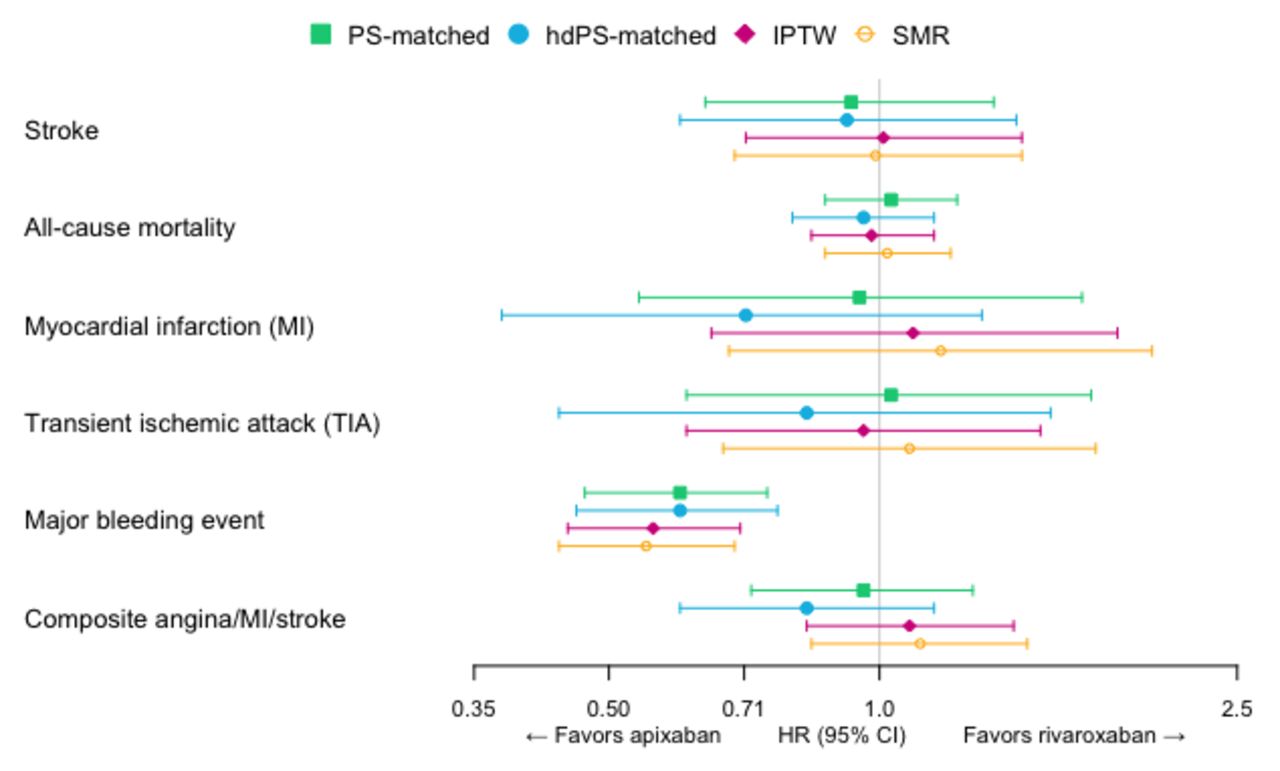
In the ITT analysis, the rate of stroke per 1000 person-years was 12.47 in the apixaban group and 13.48 in the rivaroxaban group (table 3). Compared with rivaroxaban, patients initiating apixaban showed similar rates of stroke (HR: 0.93; 95% CI 0.64 to 1.34; table 3, figure 2). Rates of secondary outcomes were also similar between apixaban versus rivaroxaban initiators: all-cause mortality (HR: 1.03; 95% CI 0.87 to 1.22), MI (HR: 0.95; 95% CI 0.54 to 1.68), TIA (HR: 1.03; 95% CI 0.61 to 1.72) and AMS (HR: 0.96; 95% CI0.72 to 1.27). Apixaban initiators showed lower rates of major bleeding events (HR: 0.60; 95% CI 0.47 to 0.75; table 3, figure 2). In secondary as-treated analysis, apixaban and rivaroxaban were similarly equivalent with respect to rates of stroke (HR: 0.95; 95% CI 0.59, 1.55; table 4).
HR of stroke and secondary outcomes among patients with nonvalvular atrial fibrillation newly initiating DOACs after propensity score matching: primary analyses
HR of stroke and secondary outcomes among patients with nonvalvular atrial fibrillation newly initiating apixaban versus rivaroxaban after propensity score matching: sensitivity analyses
{kind=link}
{kind=link}
Hazard ratios of stroke and secondary outcomes, apixaban versus rivaroxaban, intent to treat analyses. PS model accounts for age, gender, CHA2DS2 VASc score, year of treatment initiation and the following diagnoses and treatments in baseline: non-major bleeding events, anaemia, diabetes, hypertension, heart failure, osteoporosis/hip fracture, malignant neoplasm, acute kidney injury, chronic kidney disease, asthma/chronic obstructive pulmonary disease, dementia, aspirin, antiplatelets other than aspirin, warfarin, antianemic preparations, non-steroidal anti-inflammatory drugs (NSAIDs), opioids, selective serotonic reuptake inhibitors (SSRIs), antidepressants other than SSRIs, antiepileptics, antipsychotics, benzodiazepines, lipid lowering drugs, insulin, antihyperglycemics other than insulins, antihypertensives, antiarrhythmics, nitrates cardiac vasodilators, cardiac stimulants, gastrointestinal protective agents, bisphosphonates and other agents affecting bone structure, systemic corticosteroids, antineoplastics, systemic antibiotics, systemic antivirals, vaccines/immunoglobulins Patients were followed until occurrence of outcome, death, end of patient registration, or end of study period (December 2020). HdPS, high dimensional propensity score; IPTW, inverse probability of treatment weighting; PS, propensity score; SMR, standardised mortality ratio weighting.
In subgroup analyses, effects on stroke varied by concomitant aspirin use, history of warfarin use, and CHA2DS2 VASc score, though there was limited power to detect statistically significant differences (table 3). In HdPS-matched analyses of stroke and secondary outcomes, results were generally similar or trended toward lower outcome rates among patients with apixaban relative to PS-matched results (table 4, figure 2). Findings were also similar in post-hoc IPTW and SMR weighted analyses of primary and secondary outcomes (table 4, figure 2).
In ITT analysis of glaucoma as a negative control outcome, PS-matched and HdPS-matched rates of glaucoma were higher among patients with apixaban, though confidence intervals included the null (PS-matched: HR, 95% CI 1.22, 0.76 to 1.97; HdPS-matched: 1.48, 0.84 to 2.64).
Secondary comparison: apixaban versus other DOACs
After PS matching, 2276 patients with apixaban and 2276 patients with DOACs other than apixaban (rivaroxaban, edoxaban or dabigatran) were included (figure 1). Treatment groups were balanced after PS-matching, defined as ASD below 0.1 for all characteristics (table 2). Median follow-up time was longer in the apixaban group (median (IQR) 742 days [298, 1,259]) compared with the other DOACs group (681 days [296, 1170]) (online supplemental table 4). Similar rates of stroke were observed between groups (HR: 0.90; 95% CI 0.64 to 1.27; table 3).
Secondary comparison: rivaroxaban versus other DOACs
After PS matching, 1985 patients with rivaroxaban and 1985 patients with DOACs other than rivaroxaban (apixaban, edoxaban, dabigatran) were included (figure 1). Treatment groups were balanced after PS-matching, defined as ASD below 0.1 for all characteristics (table 2). Median follow-up time was shorter in the rivaroxaban group (median (IQR) 784 days [318, 1296]) compared with the DOACs other than rivaroxaban (828 days [343, 1399])(online supplemental table 4). There was no difference in rate of stroke between groups (HR: 0.96; 95% CI 0.67 to 1.36; table 3).
Discussion
Among patients with nonvalvular AFib, apixaban was as effective as rivaroxaban in reducing the rate of stroke, all-cause mortality, MI, TIA and AMS, and was safer in terms of major bleeding episodes. Because there was heterogeneity across prior study results, our results align with some but not all prior research. The Scottish, Danish, and French studies also found similar effectiveness between apixaban and rivaroxaban,13–15 while the US study found apixaban to be more effective.16 Our effectiveness findings are also consistent with the indirect comparison of apixaban and rivaroxaban in the NMA used in NICE’s 2021 clinical guidelines.5 Prior research has consistently found apixaban to be safer in terms of major bleeding.5 13 14 16 Some prior research found similar equivalencies with respect to all-cause mortality,5 14 while others have found increased risk of all-cause mortality for rivaroxaban compared with apixaban.13 16 In the secondary comparisons, the rate of stroke was similar between apixaban and other DOACs and rivaroxaban and other DOACs. These secondary comparisons offer an increase in referent group sample size with the inclusion of patients with edoxaban and dabigatran, noting that referent groups primarily comprised patients with rivaroxaban or apixaban. Apixaban and rivaroxaban were initiated more often than dabigatran and edoxaban, which is consistent with prescribing patterns in the UK30 and aligns with the selection of the primary and secondary comparisons in the study. Because dabigatran and edoxaban were seldom used and sample sizes were small, head-to-head comparisons including these DOACs were not performed.
While RCTs demonstrate that DOACs are non-inferior to warfarin for stroke prevention in patients with nonvalvular AFib,31–34 there is a lack of RCT head-to-head comparisons of individual DOACs. This uncertainty can make reimbursement, clinical decision-making and clinical guideline development challenging. NICE recently updated its AFib clinical guidelines,5 relying on a NMA and indirect comparisons of individual DOACs for evidence on their comparative effectiveness and safety. This study addresses a known evidence gap and adds to the clinical evidence base from RCTs and NMAs to directly compare DOACs for stroke prevention in patients with nonvalvular AFib in the UK. This additional evidence can help agencies like NICE contextualise the comparative effects of rivaroxaban and apixaban and inform its clinical decision-making.
This study has several strengths. The THIN data contain general practice records for over 20 million patient records in the UK and are likely reflective of typical patterns of treatment and care in the UK. Prescribing data are comprehensive and complete and are captured prospectively before outcome events. Nevertheless, this study is subject to several limitations. We did not link to secondary care data for stroke outcome ascertainment. However, stroke is included as part of the Quality and Outcomes Framework,35 where general practices are incentivised to comprehensively document instances of stroke occurring in other care settings within patients’ medical record. THIN data have been used and validated in published literature to evaluate AFib and stroke.19 36–39 We were not sufficiently powered for any of the comparisons according to the protocol power guidelines. However, an underpowered study still provides valuable information on clinical outcomes. Indeed, Hernan argues that observational causal inference studies, which place little burden on patients, should proceed even if underpowered so that the evidence can be combined with that from other studies through meta-analysis.26 For the evaluation of economic outcomes, that is, through a cost-effectiveness analysis, uncertainty in input parameter values is propagated through the use of probabilistic sensitivity analysis and thus properly reflected in the outputs. Our analysis of glaucoma as a negative control outcome indicates the possibility of residual confounding, with ITT estimates showing a higher rate of glaucoma for apixaban relative to rivaroxaban. Despite possible residual confounding resulting in bias away from the null, we still observed null findings across primary and sensitivity analyses in our primary outcome, stroke. As with the primary analysis, sample size was also a limitation of these sensitivity analyses.
THIN data contain records of prescriptions written, but it is not known whether medications were dispensed or taken. However, most patients initiating apixaban (80.9%) and rivaroxaban (76.8%) had a second prescription within 30 days of the end of their index prescription and the proportion of days covered in the follow-up period was high in both groups (mean 88.1% apixaban and mean 83.4% rivaroxaban), providing evidence that medications were being taken and refilled. Due to data availability constraints, in our analyses, we estimated patient CHA₂DS₂ VASc scores using patient history, which may deviate from a GP assessment-based score. However, 99.7% of female patients and 99.8% of male patients had patient history-estimated CHA₂DS₂ VASc scores, which aligned with the GP assessment-based score cutoffs imposed by the data vendor (≥2 and ≥1, respectively).
This study showed that among patients with nonvalvular AFib, apixaban was as effective as rivaroxaban in reducing rate of stroke and safer in terms of bleeding adverse events. This study demonstrates that comparative effectiveness RWE studies have the potential to fill evidence gaps and reduce uncertainty in HTA decision-making and clinical guideline development.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
The study concept was approved by the THIN Scientific Review Committee on 6 July 2021. Protocol number 21-013.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it was published online. The year has been changed from "2022" to "2021" in the Ethics statement.
Contributors AJ, SK, SR, SD, PJ and NG contributed to the conception and design of the study. AJ was responsible for the acquisition of the data. LG, AA, AP and PG carried out data analysis. AJ, LG, AA, AP and NG interpreted the results. AJ and LG drafted the manuscript. SK, SR, SD, MS, LK, AA, AP, PG, PJ and NG offered critical revisions and gave final sign off on the manuscript. AJ acted as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AJ, LG, AA, AP and NG are employed by and have ownership stake and/or hold stock options in Aetion. Inc. NG holds stock in Pfizer Inc. SK, SR, SD, MS, LK and PJ are employees of the National Institute for Health and Care Excellence. PJ is on the board of the GetReal Institute, which receives grants from Innovative Medicines and Horizon Europe.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.