Article Text

Abstract
Introduction Misuse of psychoactive medicines, especially prescription opioids, but also benzodiazepines, hypnotics and sedatives, has become a significant public health issue in some countries, especially in the USA, where it has been extensively documented, as well as in Canada and Australia. However, in the European Union (EU) published literature on the topic is scarce and heterogeneous regarding definitions, sources of data, tools and methods of analysis.
The aim of this scoping review is to map the key concepts on psychoactive medicines’ misuse and examine the existing body of evidence on this topic in the EU. Data on the possible consequences of medicines’ misuse—adverse drug reactions, poisonings, hospitalisations and deaths—will also be analysed.
Methods and analysis The scoping review will follow the framework of Arksey and O’Malley, further developed by Levac et al and the Joanna Briggs Institute. The search strategy, developed by the authors, includes querying three electronic databases—PubMed, Web of Science and Scopus—using keywords and the Medical Subject Headings, for evidence published in English, French, Spanish or Portuguese between 2011 and 2020. Additionally, articles from PubMed alerts and other sources will also be considered. The results of the scoping review will describe the currently available evidence regarding misuse of medicines at EU level.
Ethics and dissemination Since the scoping review methodology focuses on published data, this study does not require ethical approval. We will publish our findings in a peer-reviewed journal and plan to disseminate our work in conferences and scientific meetings.
Registration details This scoping review protocol is registered in the Open Science Framework (OSF; see https://osf.io/fzr9u) and has also been shared as a preprint in this free and open-source project management repository. It is available at https://doi.org/10.31219/osf.io/y3s4q.
- EPIDEMIOLOGY
- MENTAL HEALTH
- Substance misuse
- PUBLIC HEALTH
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Our scoping review will synthesise, in a systematic, rigorous and comprehensive manner, the available existing evidence on misuse of medicines in the European Union, providing the grounds for policy makers to take evidence-based decisions.
A limitation of this study is that the authors’ conservative approach to include the most frequently used definitions of misuse, in an effort to address the variability on terminology and the absence of a universally accepted definition of the concept of misuse of medicines, may lead to an excessive amount of data, posing challenges for feasibility within the project timelines.
Although the present scoping review uses three electronic databases and targeted search strings iteratively refined to increase the probability of retrieving as many relevant publications as possible, and has been supplemented with additional relevant articles from other sources, database selection may not have been sufficiently comprehensive (ie, searching other databases could have identified additional relevant studies).
The exclusion of grey literature from the search, or the fact that only articles of scientific journals and conference proceedings, published in English, French, Spanish or Portuguese, were considered eligible for inclusion, are also possible limitations of this study.
A quality assessment of the selected articles in the scoping review will not be performed, as this is beyond the aim of a scoping review.
Introduction
In countries like the USA, Canada and Australia, misuse of psychoactive medicines has become a significant public health issue.1 Opioid analgesics, sedatives, hypnotics and medicines used in opioid agonist treatment are reported to be the main type of medicines misused.2 Regarding opioids, Canada, Australia and especially the USA, have been experiencing an opioid epidemic,3 4 reflected in the significant morbidity and mortality in these countries currently associated with prescription opioid misuse, sometimes combined with benzodiazepines.5 6 In fact, analgesic opioid misuse in the USA is second only to marijuana use in all ages.2 Regarding sedatives, their long-term use, more common in the elderly and also in the female sex, can lead to adverse events (falls, road accidents and overdoses), tolerance, dependence and dose escalation.7
In the European Union (EU), misuse of psychoactive medicines such as opioid analgesics and other medicines acting in the central nervous system is a poorly understood issue, as published evidence is scarce. In addition, the knowledge obtained from the extensive research that is performed on the topic in the USA is difficult to transpose to the EU, due to the significant differences that are found between the two regions, namely in what concerns healthcare systems (private vs public funding), regulatory framework (differences in marketing practices of pharmaceutical companies) and prescribing practices (several prescribers vs one assistant physician). Last, but not least, the heterogeneity found between health systems in EU countries makes it even more difficult to adapt North American findings on medicines’ misuse to the EU as a whole.
There is great variability in the terminology used to describe the phenomenon of medicines’ misuse and abuse. In fact, the existing literature defines misuse in terms of prescription status (eg, any prescription-only medicine use that occurs without a prescription), reasons for use (eg, any intentional uses for intensification of effects of other psychoactive medicines or illegal drugs), ways of acquisition (eg, when the medication is obtained illegally from a dealer or on the internet, or through a relative or friend), the presence of symptoms of abuse or dependence,8 or non-medical use, which refers to the consumption of a medication that is not prescribed to a user or that is consumed in a manner not intended by the prescriber (eg, taking higher doses than prescribed, using non-approved routes of administration).9 10 Also related to misuse is the concept of doctor shopping, in which the patient consults several clinicians during the same period in order to obtain overlapping prescriptions from these different prescribers, ultimately resulting in the access to a daily dose of medication that is higher than that intended by each prescriber.11 The concept of abuse can also be defined as the persistent or sporadic, intentional excessive use of a medicinal product which is accompanied by harmful physical or psychological effects.12 According to this definition, abuse is a form of use of the substance that does not follow medical indications or prescribed dosing, meaning that abuse may be included in the definition of misuse. Given the fact that there is no universally accepted definition of misuse of medicines, in our review all situations where a medicinal product is intentionally and inappropriately used not in accordance with the terms of the marketing authorisation, including non-medical use, doctor shopping and abuse of medicinal products, will be considered forms of misuse.
Since the subject to be studied is a vast topic, with apparent knowledge gaps in the EU, the scoping review methodology was considered the most effective way to synthesise the body of evidence currently available. The objective of this scoping review, conducted in the frame of the PhD project MisuMedPT focusing on the misuse of psychoactive medicines and its morbi-mortality consequences in Portugal, is therefore to gain insight on this topic at EU level, identifying and summarising the available published evidence on misuse of medicinal products in this region of the globe.
To our knowledge, no scoping reviews on the topic of misuse of medicines have been published.
Methods and analysis
Original research articles, reviews and systematic reviews that are available from the queried databases, as well as articles from other specific sources, will be included.
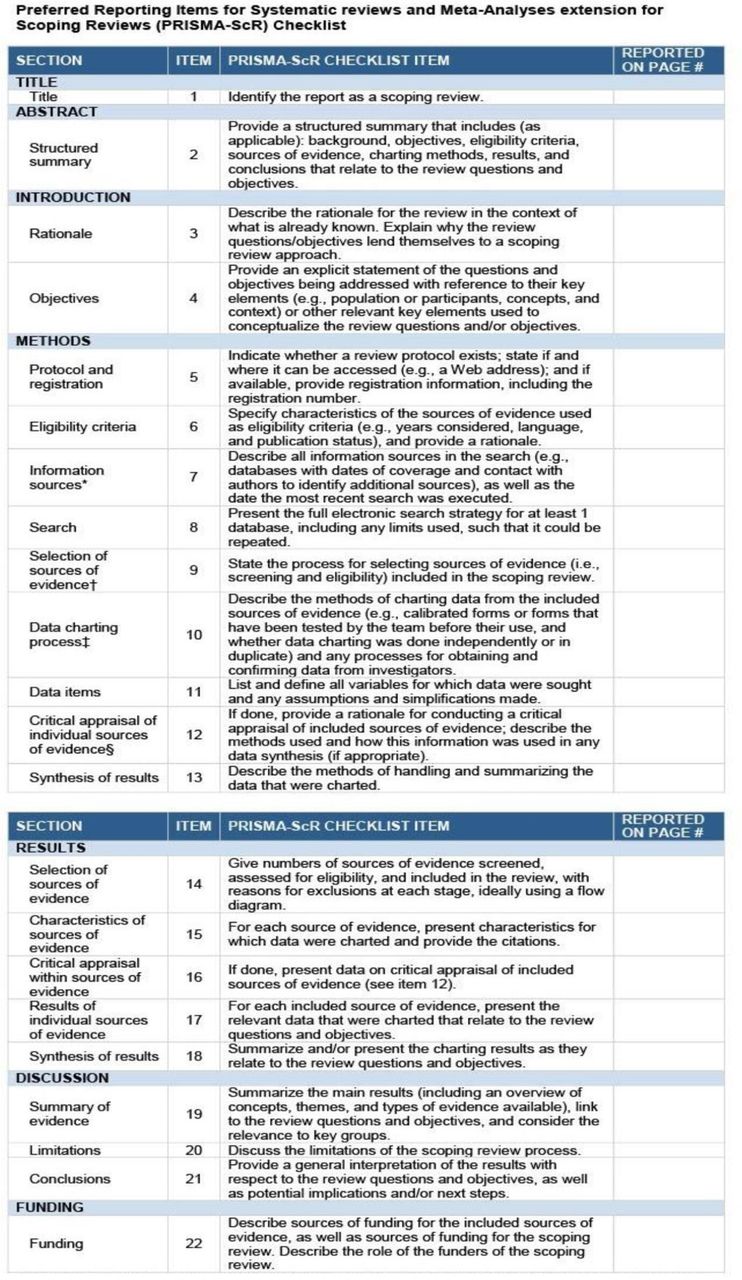
The scoping review will follow the framework created by Arksey and O’Malley,13 which has been further developed by Levac et al14 and the Joanna Briggs Institute.15 The review process will thus be organised in six stages: (1) defining the scope of the review; (2) identifying the research question; (3) identifying relevant studies; (4) study selection; (5) charting data; (6) collating, summarising and reporting results. The selection process will follow the recommendations in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist16 (figure 1) and will be mapped using a flow chart (figure 2) based on the PRISMA flow diagram for the scoping review process.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist. JBI = Joanna Briggs Institute; PRISMA-ScR = Preferred Reporting Items for Systematic reviews and Meta-Analysis extension for Scoping Reviews. * Where sources of evidence (see second footnote) are compiled from, such as bibliographic databases, social media platforms, and Web sites. † A more inclusive/heterogeneous term used to account for the different types of evidence or data sources (e.g., quantitative and/or qualitative research, expert opinion and policy documents) that may be eligible in a scoping review as opposed to only studies. This is not to be confused with information sources (see first footnote) ‡ The frameworks by Arksey and O’Malley (6) and Levac and colleagues (7) and the JBI guidance (4, 5) refer to the process of data extraction in a scoping review as data charting. § The process of systematically examining research evidence to assess its validity, results, and relevance before using it to inform a decision. This term is used for items 12 and 19 instead of “risk of bias” (which is more applicable to systematic reviews of interventions) to include and acknowledge the various sources of evidence that may be used in a scoping review (e.g., quantitative and/or qualitative research, expert opinion, and policy document). From: Tricco, et al.16

{kind=link}
{kind=link}
Flowchart for study selection.
Defining the scope of the review
For the purposes of our scoping review, we will consider misuse of medicines to be the intentional inappropriate use of a medicinal product not in accordance with the terms of its marketing authorisation, including non-medical use, doctor shopping and abuse. Our work will focus on the misuse of psychoactive medicines, that is, medicines containing substances with psychoactive effects, namely with sedative, hypnotic, anxiolytic, anticonvulsant, analgesic or antidepressant properties. Due to the differences within EU countries regarding the approval of medical marijuana for use in some medical conditions, we have decided to exclude cannabis-containing medicinal products from our scoping review. Because the available evidence on the topic in the EU is limited, with most research coming from the USA, Canada and Australia, we will be limiting our work to evidence reporting data from any country of the EU, including the UK.
Identifying the research question
The main research question is ‘What is known from the existing literature about the misuse of psychoactive medicines in the EU?’.
The research sub-questions are as follows:
What are the main psychoactive medicines/therapeutic classes misused?
What are the characteristics of individuals who misuse psychoactive medicines?
What are the main consequences associated with misuse of psychoactive medicines?
Identifying relevant studies
In order to define a search strategy capable of accurately identifying all relevant studies, an academic librarian was consulted and advised on the most appropriate Medical Subject Headings terms to consider for the search and how to adapt them to the different electronic databases used, taking into account the terms used to define medicines’ misuse. Online supplemental table 1 provides a list of the search terms used to query the databases.
Supplemental material
The search strings for each database were then finalised and recorded in online supplemental table 2 (Full search strategy recording table), and three electronic databases were searched: Web of Science, Scopus and PubMed. The searches were limited to evidence published between 2011 and 2020 in English, French, Spanish or Portuguese on misuse of medicines in the EU.
Supplemental material
During the conception phase of the MisuMedPT project, a considerable number of articles and reports, resulting from non-systematic searches or included in alerts originating from PubMed and from a scientific documentation centre, came to the authors’ knowledge and were analysed. Some of the evidence has been identified as possibly relevant for the purposes of this scoping review and, as such, was added to the initial list of abstracts to be reviewed (source classified as “other sources”).
The full list of studies retrieved was exported to Mendeley Reference Manager Application, where identification and exclusion of duplicates was performed.
Study selection
To help study selection, a flow diagram based on the PRISMA guidelines will be used (flow chart in figure 2).
Inclusion and exclusion criteria (online supplemental table 3) were based on the Population, Concept, Context and Type of evidence framework15:
Supplemental material
Population—eligible articles will include individuals, both genders, older than 15 years old.
Concept—eligible articles will include those focusing on misuse of psychoactive medicines and its possible consequences.
Context—studies published between 1 January 2011 and 31 December 2020 focusing on misuse of medicines in any country of the EU.
Types of evidence—eligible articles, written in English, Portuguese, French or Spanish, will include observational studies, letters to the editors, editorials, reports, all types of reviews and conference proceedings. Studies for which no abstract is available will be excluded, exception to be made for sources where an abstract is not expected to exist like reports, editorials or letters to the editors. Reports will be screened based on introduction and index.
Title and abstract screening, performed independently by two reviewers15 17 of the research team (primary and secondary authors) taking into account the inclusion and exclusion criteria, will be guided by the PRISMA framework. Prior to conducting the formal screening, a calibration exercise (pilot testing) will be performed on a random 5% sample18 in order to ensure reliability. The two reviewers will apply the eligibility criteria and select the abstracts independently, followed by discussion of inclusions and exclusions. Formal screening of all abstracts will start only after a percentage agreement of 75%15 is achieved, calculated by the percent agreement method.19 After ensuring that the content of the included abstracts is relevant to the aim of the study, reapplication of the eligibility criteria (online supplemental table 3) to the remaining abstracts will further refine study selection. We will document studies that are not selected for full text retrieval in a separate file. Before starting full text article screening, all the titles and abstracts for which a reviewer could not determine whether they are eligible for inclusion, will also be reviewed by the other team member.
For the final selected abstracts, the full article will be retrieved and screened; during this process, further refinement of the eligibility criteria may be needed. In order to ensure inter-rater reliability, a sample (ie, 10%) of the included full articles independently reviewed will then be compared. Disagreements about study eligibility of the sampled articles will be discussed between the two reviewers until consensus is reached or by arbitration of a third reviewer, if required, to ensure at least 75% agreement. We will also document studies that are not selected for full article final inclusion.
Charting data
All articles selected will be registered in a data chart form designed according to the Joanna Briggs Institute Manual for Evidence Synthesis (data chart draft in online supplemental table 4), using MS Office Excel 365. In this form, several details of each study will be registered, namely article name, authors and year of publication, publication type, country of origin of the data, keywords, aim, population, period covered, methods and key findings relevant to the review objective. The two reviewers will test the data chart draft on a sample of the included articles (ie, 10% of the final list of retrieved articles), in order to ensure that the chart draft is consistently applied by each reviewer. If necessary, the categories will be modified, and the data chart draft revised accordingly. Authors of the selected articles may be contacted to request missing or additional data, should essential questions arise. Once again, to ensure inter-rater reliability both reviewers’ independent data charts will be compared; any discrepancies will be iteratively discussed by the researchers to ensure consistency.
Supplemental material
Collating, summarising and reporting results
Analysis of the data collected will provide information on the body of evidence regarding misuse of medicines and its morbi-mortality consequences, compiling the apparently scarce and scattered evidence that has been published at EU level. In addition, the identification of knowledge gaps will inform on aspects that lack research, such as classes of psychoactive medicines still not addressed in the literature, or EU countries where no information on the topic has been made available. The extracted data, covering the breadth of existing evidence, will be presented in a tabular form in a manner that aligns with the objectives of this scoping review, with a narrative summary accompanying the charted results, using MS Office Excel and Word 365.
Ethics statements
Patient consent for publication
Acknowledgments
We wish to thank Susana Oliveira Henriques, Health Information Specialist from the University of Lisbon School of Medicine, for her relevant contribution to the searches performed in the selected databases.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors ACA and APM conceived the idea of the scoping review, developed the research questions and contributed significantly to the development of the methods. RJC and ACA defined together the search strategy and the eligibility criteria. RJC drafted the protocol manuscript and ACA contributed substantially to its drafting and editing. APM supervised the preparation of the protocol and the final protocol manuscript was critically reviewed by both APM and JG. All authors approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.