Article Text

Abstract
Introduction Hiccup is a common disease that not only occurred on adults but also on infants, which can severely do harm to patients’ physical and psychological health. Metoclopramide has been reported to have effects on intractable hiccup. However, there is a limited evidence that describes the efficacy and safety of metoclopramide in the treatment of intractable hiccup. The aim of this article is to obtain evidence on the effectiveness and safety of metoclopramide in treating patients with intractable hiccup.
Methods and analysis We will search the following databases, including PubMed, Cochrane Library, Embase, Web of Science, CBM, Wan-fang, VIP database, CNKI and MEDLINE from their inception to 11 November 2021. All the randomised controlled trials associated with metoclopramide in treating intractable hiccup will be included. Articles screened, selected and extracted will be performed by two researchers independently. The risk of bias will be assessed by using the Cochrane Collaboration. We will carry out the meta-analysis by using RevMan V.5.4 software.
PROSPERO registration number CRD42021293000.
- INTERNAL MEDICINE
- GASTROENTEROLOGY
- OTOLARYNGOLOGY
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We will strictly follow systematic review and meta-analysis guidelines to minimise bias.
The quality of the publications included in this review are likely to influence the final results.
This article will search English and Chinese literature, which will be an updated and more comprehensive review compared with what has been published previously.
The many aetiologies of hiccup and wide-ranging comorbidities may contribute to highly heterogeneity of the response to metoclopramide.
Introduction
Hiccup, also known as singultus, originates from Latin. It means the act of holding one’s breath while crying.1 Hiccup is a common physiological phenomenon that almost occurs on everyone.2 Most patients with acute hiccup are self-limited, and rare patients will persist a few days, a few months or even a few years. Based on their duration, it can be classified into persistent hiccup and intractable hiccup. Hiccup lasting more than 48 hours is called persistent hiccup while lasting more than a month is called intractable hiccup.3 Intractable hiccup can lead to a significant deterioration in quality of life, with common situation such as insomnia, poor appetite or fatigue. More importantly, intractable hiccup may be a potential signal of some diseases.4
Hiccup is caused by spasmodic contraction of the diaphragm and intercostal muscles.5 It is widely believed that intractable hiccup involves a reflex centre or peripheral reflector, but lack of clear anatomical evidence.6 Over 100 causes may trigger hiccup, which can be roughly divided into the following categories7 8: (1)gastrointestinal diseases: peptic ulcer, stomach spasm, gastro-oesophageal reflux; (2) malignant tumours: lung cancer, stomach cancer, oesophageal cancer, brain tumour; (3) chest diseases: pleurisy, pleural effusion, pneumonia, myocardial infarction; (4) mental stimulation: afraid, excessive anxiety or excitement; (5) drugs: anti-infective drugs (penicillin), corticosteroids (dexamethasone), chemotherapy drugs (cisplatin) and benzodiazepines (diazepam); (6) electrolyte disorder: low sodium, low calcium. Irritation and distention of the stomach are the most common causes of hiccup, such as overeating, eating spicy food and drinking plentiful carbonated drinks.9
In the past, chlorpromazine was priority medication in treating hiccup, which was the only drug approved by the US Food and Drug Administration.10 Due to the adverse effects, it is not recommended as a first-line drug now.11 At present, many agents have been reported to be helpful in treating intractable hiccup, such as metoclopramide, baclofen and gabapentin. Alternate therapies such as acupuncture and hypnosis are also used to treat intractable hiccup. Surgery may be an option in the case of other treatments been failed. Although currently numerous therapies have been proposed, unfortunately the treatment of intractable hiccup still remains challenging.1 12
Metoclopramide is used to treat gastrointestinal diseases.13 It is reported that metoclopramide can be effective on relieving the symptom of intractable hiccup which caused by stroke, cancer, migraine, gastrointestinal diseases and so on.14 15 This may bring hope to patients with intractable hiccup.16 Due to a lack of big data studies, it has not reached a consensus. Systematic evaluation and meta-analysis will be conducted to provide evidence for metoclopramide in the treatment of intractable hiccup.
Objective
This study is to assess the efficacy and safety of metoclopramide in treating patients with intractable hiccup.
Methods
Registration
The protocol in this study was consistent with the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 statement.17 The PRISMA-P is shown in online supplemental appendix 1.
Supplemental material
Patients and public involved
In this review study, patients and the public will not be directly involved.
Study selection inclusion/exclusion criteria
Types of patients
Patients with hiccup lasting longer than 1 month without self-remission, regardless of age, race, nationality or gender.
Types of studies
All randomised controlled clinical trials published concerning metoclopramide in treating intractable hiccup will be included. Literature studies, animal studies, case reports, dissertations and quasi-randomized control trials (RCTs) will be excluded.
Types of inventions
The experimental group is principally treated with oral or injected metoclopramide, which could be combined with other drugs therapy. The control group is treated with placebo, baclofen, gabapentin or other western medicines.
Types of outcome measures
The primary outcomes include severity of intractable hiccup, frequency of hiccup, increase in hiccup-free periods and effective rate. The secondary outcomes include adverse events, dosage forms of metoclopramide, the therapeutic and toxic dose of metoclopramide.
Search strategy
PubMed, Cochrane Library, Embase, Web of Science, Wan-fang, VIP, CNKI, CBM database and MDELINE will be searched. Randomised controlled studies from their inception to 11 November 2021 will be retrieved. The complete search strategy from PubMed is shown in box 1. And the whole database search strategy provided in online supplemental appendix 2.
Supplemental material
Search strategy in PubMed database
Search items
Metoclopramide.Mesh.
Metaclopramide.ti.ab.
Maxolon.ti.ab.
Rimetin.ti.ab.
Metoclopramide Hydrochloride.ti.ab.
Hydrochloride, Metoclopramide.ti.ab.
Metoclopramide Monohydrochloride.ti.ab.
Monohydrochloride, Metoclopramide.ti.ab.
Metoclopramide Monohydrochloride, Monohydrate.ti.ab.
Primperan.ti.ab.
Reglan.ti.ab.
Cerucal.ti.ab.
Metoclopramide Dihydrochloride.ti.ab.
Dihydrochloride, Metoclopramide.ti.ab.
1 or 2–14.
Hiccup.Mesh.
Hiccups.ti.ab.
Hiccough.ti.ab.
Hiccoughs.ti.ab.
singultus.ti.ab.
16 or 17–20.
Randomized controlled trial. Mesh.
Controlled clinical trial.ti.ab.
Randomized.ti.ab.
Randomly.ti.ab.
Trial.ti.ab.
22 or 23–26.
15 and 21 and 27.
Data acquisition
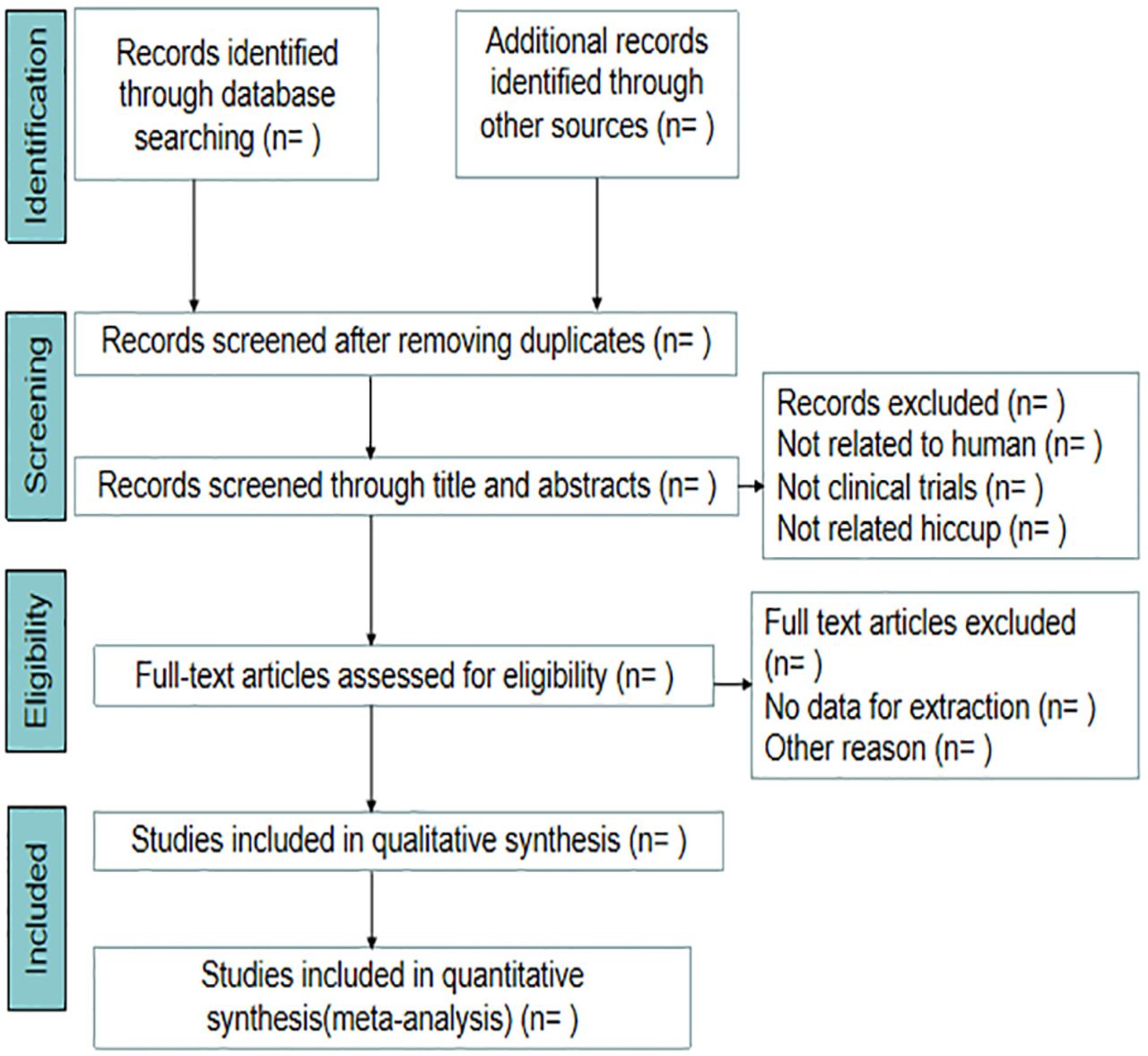
The electronically retrieved articles will be imported into EndNote X9.1 after deleting duplicates. First, two evaluators (LW and TC) will independently screen abstract and title based on the inclusion criteria and exclusion criteria. Then two evaluators will review the full text and determine whether to include the article. The excluding studies will be recorded the reasons. Any disagreement between two evaluators will be resolved by discussion. If a consensus still cannot be reached in the end, it will be decided by a third researcher (BW). The flow diagram of screening the selecting studies is shown in figure 1.
{kind=link}
Flow diagram of the study selection process.
Data extraction and management
Relevant information will be extracted by two evaluators (BZ and CZ) using Excel 2019 software. And we will obtain data from the article including literature source, year and month of publication, sample size, name of first author, country of origin, intervening measure, participant characteristic, aetiologies of hiccup, severity of intractable hiccup, hiccup-free period, frequency of hiccup, adverse event, dose and dosage form of metoclopramide and duration of follow-up. If the data of the literature are incomplete or not clear, we will contact the corresponding author to obtain further information.
Data synthesis and analysis
We will tabulate the vital information such as methods, results, aetiologies of hiccup and adverse events. When there are more than five studies, RevMan V.5.4 will be used to analyse data. Otherwise, we will implement a systematic narrative synthesis following accepted guidelines. The same interventions and outcomes will be combined to estimate efficacy and safety of metoclopramide in treating patients with intractable hiccup by using a meta-analysis. Dichotomous data will be expressed by OR, RR (risk ratio) or 95% CI while continuous variables will be expressed by SMD and 95% CI. In the absence of heterogeneity, we will pool effect size with 95% CI fixed effects model. If there is significant heterogeneity (I2>50%), a random effects model will be used.
Subgroup analysis and sensitivity analysis
If there is significant heterogeneity among publication, subgroup analysis about the aetiologies of hiccup will be performed to identify the possible source of heterogeneity. We will reduce sensitivity by reanalysing the data and excluding low-quality research.
Bias assessment
The risk of bias will be assessed by the three investigators (LW, BZ, YG) using the Cochrane Collaboration, which will be classified into three levels of unclear risk, high risk and low risk. The three levels are evaluated by studying allocation concealment, blinding, randomisation, selective outcome reporting, incomplete data and other biases.
Heterogeneity assessment
Heterogeneity comes from clinical heterogeneity, statistical heterogeneity and methodological heterogeneity. When the sample is small, I2 statistic will be selected for heterogeneity assessment. I2 is 75%, 50% and 25% representing large, medium and small heterogeneity, respectively. The value of I2 is greater, the heterogeneity will be greater. It is generally believed that I2 no more than 50% can be accepted.
Grading the quality of evidence
According to heterogeneity, risk of bias, accuracy, indirectness and publication bias, the level of evidence for the study will be rated as high, medium, low and very low.
Ethics and dissemination
It does not require ethical approval. The final results will be presented at relevant conferences or disseminated in peer-reviewed journals.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors DW designed this protocol and registered in the PROSPERO database. LW and TC will select the articles after reading. BZ and CZ will extract data independently. Any differences should be determined after discussion with the third reviewer BW to ensure that no errors occur during the review process. DW and YG revised the final manuscript. All authors have read and approved the publication of the protocol.
Funding This work was supported by National Major New Drug Project of Ministry of Science and Technology (No. 2018ZX09721004-009).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.