Article Text

Abstract
Objective The Brazilian state of Paraná has suffered from COVID-19 effects, understanding predictors of increased mortality in health system interventions prevent hospitalisation of patients. We selected the best models to evaluate the association of death with demographic characteristics, symptoms and comorbidities based on three levels of clinical severity for COVID-19: non-hospitalised, hospitalised non-ICU ward and ICU ward.
Design Cross-sectional survey using binomial mixed models.
Setting COVID-19-positive cases diagnosed by reverse transcription–PCR of municipalities located in Paraná State.
Patients Cases of anonymous datasets of electronic medical records from 1 April 2020 to 31 December 2020.
Primary and secondary outcome measures The best prediction factors were chosen based on criteria after a stepwise analysis using multicollinearity measure, lower Akaike information criterion and goodness-of-fit χ2 tests from univariate to multivariate contexts.
Results Male sex was associated with increased mortality among non-hospitalised patients (OR 1.76, 95% CI 1.47 to 2.11) and non-ICU patients (OR 1.22, 95% CI 1.05 to 1.43) for symptoms and for comorbidities (OR 1.89, 95% CI 1.59 to 2.25, and OR 1.30, 95% CI 1.11 to 1.52, respectively). Higher mortality occurred in patients older than 35 years in non-hospitalised (for symptoms: OR 4.05, 95% CI 1.55 to 10.54; and for comorbidities: OR 3.00, 95% CI 1.24 to 7.27) and in hospitalised over 40 years (for symptoms: OR 2.72, 95% CI 1.08 to 6.87; and for comorbidities: OR 2.66, 95% CI 1.22 to 5.79). Dyspnoea was associated with increased mortality in non-hospitalised (OR 4.14, 95% CI 3.45 to 4.96), non-ICU (OR 2.41, 95% CI 2.04 to 2.84) and ICU (OR 1.38, 95% CI 1.10 to 1.72) patients. Neurological disorders (OR 2.16, 95% CI 1.35 to 3.46), neoplastic (OR 3.22, 95% CI 1.75 to 5.93) and kidney diseases (OR 2.13, 95% CI 1.36 to 3.35) showed the majority of increased mortality for ICU as well in the three levels of severity jointly with heart disease, diabetes and CPOD.
Conclusions These findings highlight the importance of the predictor’s assessment for the implementation of public healthcare policy in response to the COVID-19 pandemic, mainly to understand how non-pharmaceutical measures could mitigate the virus impact over the population.
- epidemiology
- public health
- diabetes & endocrinology
- kidney & urinary tract disorders
- COVID-19
- cardiac epidemiology
Data availability statement
Data are available upon request from authors.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- epidemiology
- public health
- diabetes & endocrinology
- kidney & urinary tract disorders
- COVID-19
- cardiac epidemiology
Strengths and limitations of this study
The current study examined the predictors of mortality in symptoms due to COVID-19 disease and comorbidities in three levels of severity in context with reduced mitigation measures and without vaccination.
We built a detailed stepwise analysis to choose the best factors to predict mortality.
The missing data combined play a central role in decreasing sample size, creating some limitations in terms of exclusion to build the severity/medical intervention.
Introduction
Following the first confirmed case in Wuhan in late December 2019, SARS-CoV-2 spread rapidly into a global pandemic. In Brazil, COVID-19 was first reported in April 2020—approximately 2 months after the first confirmed COVID-19 case in China1—with the country’s first death registered on 17 March 2020.2 Brazil has since witnessed a massive increase in COVID-19 cases, having reached a total of 30 093 751 cases and 660 973 deaths (Painel coronavírus, https://covid.saude.gov.br/, accessed in April 2022).
As a very large country, Brazil’s experience of a dissimilar spread pace of COVID-19 may due to multifactorial differences such as sociodemographic index varying in a subnational regional context, SARS-CoV-2 lineage diversity and population genetic variance.3 The state of Paraná is located in South Brazil, composed of 11 million inhabitants. Its current population has a significant genetic contribution from European ancestral populations (ranging from 40% to 86% of the total) due to mass immigration of Eastern Europeans in the 18th and 19th centuries. The remainder of the region’s population comprises Africans (9%–40%) and Native Americans (4%–7%).4–6
The Brazilian public health system, better known as the Unified Health System (SUS), is the largest non-discriminatory government-run public healthcare system in the world by both numbers of beneficiaries/users and land area. However, its infrastructure is heterogeneous among geographical regions and subregions.
Notably, a year and a half after the onset of the pandemic, few studies have measured and reported the impact of the COVID-19 pandemic concerning such demographic characteristics, including clinical phenotypes and comorbidities. According to Martins-Filho et al, social and ethnic disparities may have influenced COVID-19-related deaths in Brazil with a higher relative risk of mortality from COVID-19 (1.50%–95.0% CI), such discrepancy was also observed in the southern region (1.54%–95.0% CI), which is located in the state of Paraná, the focus of this study.7
These findings show that ethnic disparities in Brazil are strongly associated with precarious environments and conditions of basic sanitation and housing. Therefore, they have important implications for the COVID-19 mortality rate. Furthermore, minority populations have a disproportionate burden of underlying comorbidities, including hypertension and diabetes, increasing the risk of hospitalisations.8
These studies are critical for a better understanding of varying infection and death rates observed in the state and across other populations. Thus, this study aimed to evaluate, from positive COVID-19 cases, if demographics traits (sex, age and Human Development Index (HDI)), disease symptoms and comorbidities are predictors of mortality for COVID-19 cases. Patients from two main sets of symptoms and commodities were selected based on levels of clinical severity (medical intervention) accessed on anonymous data—non-hospitalised considered as mild level, hospitalised in non-ICU wards as moderate level and hospitalised in ICU wards as severe level—in the period from April to the end of December 2020 in Paraná State, Brazil.
Methods
Patient and public involvement
No patient was involved. Only anonymous datasets of electronic medical records (EMRs) from the Public Health Department of Paraná State, Brazil, which is integrated into the public SUS, were evaluated, following the workflow shown in figure 1.

Flowchart of the study: epidemic landscape of COVID-19 in Paraná State, Brazil, 1 April–31 December 2020. ICU, intensive care unit.
All patients diagnosed with SARS-CoV-2 by reverse transcription–PCR (RT-PCR) in nasopharyngeal cells were included, totalling 204 243 individuals between 1 April 2020 and 31 December 2020, provided each case had a registered outcome. Registers were available from public and private institutions—including inpatient and outpatient care clinical settings—covering all cases of COVID-19 notified in healthcare units in Paraná State.
The symptoms and comorbidities were selected in accordance with the WHO technical guidance for COVID-19 (https://www.cebm.net/COVID-19/covid-19-signs-and-symptoms-tracker). The datasets based on EMRs, excluding missing data, were filtered, extracted and preprocessed using customised Python Scripts with Pandas.6 This analysis resulted in the identification of 101 280 cases with at least one symptom and 102 963 cases with at least one comorbidity (visualised by Methods section of the online supplemental material).9–13
Both datasets were further subgrouped according to clinical or medical intervention (partially overlapped) and over 25 years old, considering adults over 20 years old based on WHO designation (https://apps.who.int/adolescent/second-decade/section2/page1/recognizing-adolescence.html): (1) mild cases or non-hospitalised patients in primary attendance/emergency units, kept isolated at home or even those who were waiting for treatment; (2) moderate cases or isolated patients with COVID-19 in non-ICU wards; and (3) severe cases or patients in the ICU. The median time of hospitalisation was not available for inclusion in this analysis. The description of the categorical variables of the patients’ symptoms and comorbidities was expressed in IQRs and absolute numbers and proportions, respectively (online supplemental tables S1 and S2).
Supplemental material
Mortality was assessed by binomial logistic regression following the next steps described further. Categorical variables were selected based on univariate logistic regression models (glm function) evaluated by vif (multicollinearity function) and χ2 test (Wald test) from the regTermTest function from the survey package against the null model for all severity groups (non-hospitalised, non-ICU and ICU) (available on online supplemental tables S3–S8). Afterwards, to proceed to a multivariate context, a second step was a stepwise analysis using lower Akaike information criterion (AIC) and goodness of fit provided from χ2 tests from the drop1 function to choose robust covariates as fixed effects.10 In the third step, within a generalised mixed model, municipalities were included as random effect and implemented in the glmer function from lme4 to account for individuals who shared the same origin and health facility access and incorporated the temporal effect due to the differences between the municipalities at the beginning of the pandemic event. The complete models were adjusted after removing confounders and inclusion, exclusion with/without interaction tests by lower AIC, and goodness of fit provided from χ2 tests from the drop1 function; following these criteria, the symptoms and comorbidities when evaluated in the same set decreased the sample size and analysis power. The best models chosen were plotted in coefplots shown in the Results section, and univariate steps are shown in online supplemental tables S3–S8. All analyses were performed using R environment V.4.0.3.12
Results
The present study sampled information registered from April to December 2020 in the state of Paraná (figure 2A) for 101 280 symptomatic cases and 102 962 comorbidy cases diagnosed as positive for SARS-CoV-2 infection by RT-PCR, with outcomes classified as either recovery or death (descriptive data in online supplemental tables S1 and S2). The spread of SARS-CoV-2 in Paraná was slow during the first months of the pandemic (figure 2B,C). A similar distribution was observed for the 5909 individuals that passed away due to COVID-19 (figure 2D,E). The cases were widespread in the state but highly concentrated in the large urban centres. The first occurrences were recorded on 1 April (figure 3A) in the metropolitan region of the capital city, Curitiba, followed by other large cities (Londrina, Maringá and Cascavel) and Foz do Iguaçu, one of Brazil’s most popular tourist destinations, and most of them remained with open airports. The pandemic continued to spread rapidly throughout 2020 (figure 3B), especially in the third and fourth quarters of the year (figure 3C,D).

Geographical distribution of COVID-19 cases and deaths confirmed by reverse transcription–PCR testing in the state of Paraná. (A) Geographical location of Paraná State. (B) Proportion of cases in comparison with São Paulo. (C) Proportion of deaths from COVID-19 in São Paulo and Paraná State over the epidemiological weeks. (D) Positive cases of SARS-CoV-2 per 100 000 inhabitants. (E) Deaths from COVID-19 per 100 000 inhabitants.

Progression of the SARS-CoV-2 pandemic in the state of Paraná during the year 2020, over four time periods: (A,B) first and second quarters: April–June, (C) first–third quarters: April–September, (D) first–fourth quarters: April–December.
Among the symptoms group, 45.89% were male, with most belonging to the age ranges 25–30 (25.40%), 30–35 (12.90%), 30–35 (12.19%) and over 55 years (20.94%). The most common symptoms were cough (65.23%), headache (61.17%), myalgia (54.44%), sore throat (46.14%), fever (40.92%), anosmia (24.74%), fatigue (26.96 %), dyspnoea (20.76%) and diarrhoea (17.47%) (figure 3A). A total of 93 942 individuals were non-hospitalised, of which 0.59% died. Among the hospitalised individuals in non-ICU wards, 5252 cases (4.71%) received medical care in the hospital system, of which 20% died. Among the 2086 cases (1.84%) that were hospitalised in ICUs, 68.89% died (figure 4A and online supplemental table S1).
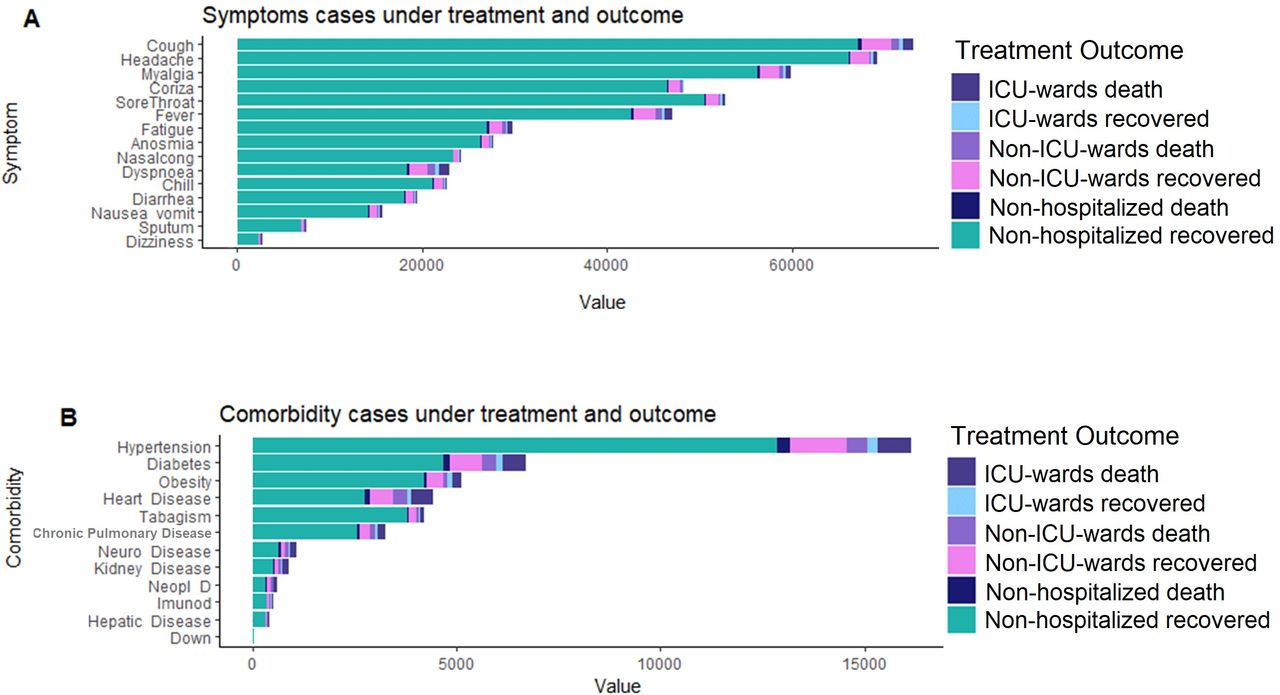
(A) Symptom and (B) comorbidity distributions in patients with COVID-19 in Paraná, Brazil, considering the three medical intervention groups and their respective outcomes (recoveries or deaths) among the studied groups. Down, Down syndrome; ICU, intensive care unit; Immunod, immunodeficiency; Neol_D, neoplastic disease; Neuro_Disease, neurological disease.
In the comorbidity group, 46% were male and the main age ranges were 25–30 (25.38%), 30–35 (12.92%), 30–35 (12.16%) and over 55 years (20.88%). The most frequent comorbidities were hypertension (15.62%), obesity (4.80%), diabetes (6.46%), heart disease (4.24%), chronic pulmonary disease (2.80%), and neuronal disease (0.98%) (figure 4B and online supplemental table S2). Of the patients presenting with at least one comorbidity, 95 352 were not hospitalised, of which 0.62% died. The number of patients hospitalised in non-ICU wards was 5484, of which 18.49% died. Among the 2126 cases that received intensive care, 69.84% died. The hospitalisation period for both groups was not available to be included in the analysis. In order to evaluate whether these demographics and clinical traits described previously are associated with death, we applied univariate models, χ2 tests, multicollinearity tests and multivariate models with fixed effects to choose the variables for the best fit for the generalised mixed model (online supplemental tables S3–S5). For all results from best-fit generalised mixed models, we interpreted municipalities as a random effect, in which the findings represent the impact of each categorical variable for every health intervention designed group considering inhabitants from the same regions.
During the period evaluated, 93 942 patients showed complete data with at least one symptom and considered mild cases had not been hospitalised. The best multivariate model for this dataset showed an increased mortality for men compared with women (OR 1.76, 95% CI 1.47 to 2.11). A higher mortality rate was found in individuals over 35 years old compared with young adults (25–30 age group), with the highest odds of death in the age ranges 35–40 (OR 4.05, 95% CI 1.55 to 10.54), 40–45 (OR 5.76, 95% CI 2.29 to 14.49), 45–50 (OR 13.09, 95% CI 5.59 to 30.64), 50–55 (OR 18.07, 95% CI 7.83 to 41.73) and over 55 (OR 88.12, 95% CI 40.33 to 192.54). The main clinical symptoms associated with increased mortality were fever (OR 1.57, 95% CI 1.31 to 1.88), dyspnoea (OR 4.14, 95% CI 3.45 to 4.96) and fatigue (OR 1.24, 95% CI 1.02 to 1.51), while headache (OR 0.48, 95% CI 0.39 to 0.58), myalgia (OR 0.71, 95% CI 0.59 to 0.86) and nasal congestion (OR 0.64, 95% CI 0.47 to 0.85) were associated with decreased mortality (table 1, online supplemental table S3 and figure 5A). Interestingly, HDI was not associated with the likelihood of death in this group in a multivariate context only in a univariate analysis.
Multivariate models based on the best prediction power analysis for factors associated with mortality in patients with COVID-19 with at least one or more symptoms in Paraná State

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Regression plot of best models for mortality predictors in symptoms and comorbidities. (A) Non-hospitalised patients in the symptoms group. (B) Non-ICU ward patients in the symptoms group. (C) ICU patients in the symptoms group. (D) Non-hospitalised patients in the comorbidities group. (E) Non-ICU ward patients in the comorbidities group. (F) ICU patients in the comorbidities group. In symptoms and comorbidities (S): presence. C_PulD, chronic obstructive pulmonary disease; HDI, Human Development Index; ICU, intensive care unit; M, male; Neol_D, neoplastic disease; Neuro_Disease, neurological disease.
For 5252 patients hospitalised in non-ICU wards, the variables in the best prediction model are available in table 1, and excluded variables are available in online supplemental table S4. Here, demographic traits also showed a relevant role in mortality by COVID-19. We estimated an increased odds of death for men (OR 1.22, 95% CI 1.05 to 1.43). Increasing odds of death were associated with the following age ranges: 40–45 (OR 2.72, 95% CI 1.08 to 6.87), 45–50 (OR 2.88, 95% CI 1.16 to 7.13), 50–55 (OR 3.68, 95% CI 1.52 to 8.90) and over 55 years (OR 14.96, 95% CI 6.50 to 34.44). Among the clinical symptoms, dyspnoea (OR 2.41, 95% CI 2.04 to 2.84) and dizziness (OR 1.91, 95% CI 1.38 to 2.65) presented the major increase in the OR of death. On the other hand, headache (OR 0.59, 95% CI 0.59 to 0.86), myalgia (OR 0.69, 95% CI 0.58 to 0.82) and sore throat (OR 0.71, 95% CI 0.59 to 0.86) were associated to decrease of mortality rate (table 1 and figure 5B).
The analysis of the cases of 2086 patients admitted to the ICUs, as for the other groups, showed that older age ranges were again associated with increased probability of death, as seen for the age groups 45–50 (OR 2.23, 95% CI 1.07 to 4.66), 50–55 (OR 3.11, 95% CI 1.51 to 6.40) and over 55 years (OR 5.11, 95% CI 2.69 to 9.69). In addition, dyspnoea increased the odds of death (OR 1.38, 95% CI 1.10 to 1.72), while myalgia (OR 0.73, 95% CI 0.58 to 0.91) and headache (OR 0.72, 95% CI 0.57 to 0.91) were associated with lower mortality. Sex did not appear to influence the probability of death in this level of severity (table 1, online supplemental table S5 and figure 5C).
For 102 963 patients with at least one comorbidity to determine whether the mortality was associated with disease, we test each variable (disease or previous condition) to include or exclude for the complete model, performing univariate models, χ2 tests, multicollinearity tests and multivariate models with fixed effects to choose the best fit for the generalised mixed logistic regression model for each complete dataset (online supplemental tables S6–S8). We also tested the interaction between these diseases in cases that the individual has both concomitantly (about 0.07% of cases); however, in any case, we did not find significant interaction. In 95 353 patients non-hospitalised, male individuals showed an increased OR of death (OR 1.89, 95% CI 1.59 to 2.25), while higher odds of death was observed for the age ranges 35–40 (OR 3.01, 95% CI 1.24 to 7.27), 40–45 (OR 5.81, 95% CI 2.63 to 12.98), 45–50 (OR 10.81, 95% CI 5.08 to 22.92), 50–55 (OR 15.46, 95% CI 7.43 to 32.25) and over 55 years (OR 65.79, 95% CI 33.23 to 130.24). HDI was associated with low mortality (OR 0.03, 95% CI 0.001 to 0.38), which indicates a small detection of socioeconomic factors. Increased mortality was observed for the most common comorbidities: obesity (OR 2.18, 95% CI 1.67 to 2.85), diabetes (OR 1.84, 95% CI 1.49 to 2.26), heart disease (OR 2.33, 95% CI 1.86 to 2.91], chronic obstructive pulmonary disease (OR 1.65, 95% CI 1.19 to 2.29), neurological disorders (OR 2.59, 95% CI 1.75 to 3.84) and kidney disease (OR 2.22, 95% CI 1.39 to 3.82) (table 2 and figure 5D).
Multivariate models based on the best prediction power analysis for factors associated with mortality in patients with COVID-19 with at least one or more comorbidities in Paraná State
In a total of 5484 patients hospitalised at non-ICU wards included as a comorbidities data, in the best model men showed the highest recorded mortality (OR 1.30, 95% CI 1.11 to 1.52). In comparison to younger individuals, comorbidities in older patients increased the risk of death, specifically in over 45–50 years (OR 2.66, 95% CI 1.22 to 5.79), 50–55 years (OR 2.85, 95% CI 1.33 to 6.10) and over 55 years (OR 11.65, 95% CI 5.80 to 23.41). The comorbidities associated with higher odds of death in the COVID-19 cases were diabetes (OR 1.42, 95% CI 1.19 to 1.71), heart disease (OR 1.87, 95% CI 1.54 to 2.26), chronic pulmonary disease (OR 2.20, 95% CI 1.70 to 2.85), neurological disease (OR 3.19, 95% CI 2.44 to 4.71), neoplastic disease (OR 3.19, 95% CI 2.15 to 4.71), immunodeficiency (OR 1.97, 95% CI 1.13 to 3.43) and kidney disease (OR 2.39, 95% CI 1.60 to 3.56) (table 2, online supplemental table S7 and figure 5E). Finally, from 2126 patients with comorbidities admitted to the ICU, individuals over 60 years showed increased risk of death: 50–55 years (OR 4.42, 95% CI 2.26 to 8.66) and over 55 years (OR 4.42, 95% CI 2.26 to 8.66). Comorbidities such as diabetes (OR 1.66, 95% CI 1.32 to 2.11), heart disease (OR 2.11, 95% CI 1.63 to 2.73), neurological disorders (OR 2.16, 95% CI 1.35 to 3.46), chronic obstructive pulmonary disease (OR 1.48, 95% CI 1.04 to 2.12), neoplastic disease (OR 3.22, 95% CI 1.75 to 5.93) and kidney disease (OR 2.13, 95% CI 1.36 to 3.35) were found correlated with higher odds of death (table 2, online supplemental table S8 and figure 5F).
Discussion
In this study, we found demographic traits, symptoms and comorbidities as mortality predictors in COVID-19 cases in three medical intervention groups (severity); specifically, ICU level, considered a severe level, showed the most frequency of mortality.14 The spread of COVID-19 in Paraná occurred at a slower pace and peaked later than that in other Brazilian regions. Several factors could account for this delay in Paraná, such as the early implementation of decree restrictions in 16 March addressing an international public health emergency from COVID-19 (https://www.coronavirus.pr.gov.br/Campanha/Pagina/TRANSPARENCIA-Enfrentamento-ao-Coronavirus-Legislacao). Measures also adopted in São Paulo state (https://www.saopaulo.sp.gov.br/coronavirus/quarentena/). Federal law in 6 February 2020 establishes measures for COVID-19, without air travel restrictions (http://www.planalto.gov.br/CCIVIL_03/_Ato2019-2022/2020/Lei/L13979.htm). The Parana hospital care networks are specifically concentrated in regions with high-density populations, such as the East macroregion, where the most cases have risen, and indeed it reached 575 beds in the ICU and 786 beds in the non-ICU in 2020 (https://www.saude.pr.gov.br/Pagina/Regionais-de-Saude).
Although the SARS-CoV-2 infection rate is similar in women and men, male sex is associated with increased severity in COVID-19 in the majority of worldwide COVID-19 reports, including the ones from Brazil, Korea, UK and USA.15–22 However, none of these studies reported results for non-hospitalised patients. We found that among non-hospitalised symptom and comorbidity patients, as well as symptom patients in non-ICU wards, the odds of death were higher for men, although no difference in odds of death was observed between the sexes of patients admitted to the ICU.
The probability of death was also higher among older individuals in this study, which can be associated with the prevalence of chronic diseases that contribute to adverse symptoms and COVID-19 progression.23 24 Age-stratified predictors revealed an association with odds of death for adults over 35 years and a strong association for adults over 50 years old of both symptoms and comorbidities in non-hospitalised, non-ICU groups and ICU groups. Our findings, however, differ from data of most other countries, which usually evidence strong odds of death only associated with age over 65 years.25 26 In China and European countries, ages above 65 years were found as a strong death predictor.17 27 It may be explained by higher activity of the innate and proinflammatory immune response, and lower activity of the adaptive immune response in older men may explain their increased risk, despite the similarity of the immune epigenomic signatures between elderly men and women.28
In addition to the demographic predictors discussed previously, we also assessed the association of clinical characteristics with odds of death across degrees of disease severity. About 0.52% of non-hospitalised symptom patients deceased, compared with 19.7% of non-ICU ward patients and 68.63% ICU-ward patients, suggesting the severity of disease.16 29 30 The frequency of these symptoms varied according to the severity of the disease. The most common symptoms of the study were cough, headache, myalgia, sore throat and fever, followed by fatigue, chills, nasal congestion and dyspnoea. Fever, dyspnoea and fatigue were associated with higher odds of death in non-hospitalised and dizziness–dyspnoea in non-ICU, but only the last one increased the odds of death in ICU patients.
In an independent patient cohort of 56 patients with moderate to severe infection (33 admitted to the ICU) from Curitiba, the capital city of Paraná, the most common symptoms observed were cough, fever and dyspnoea, the latter being the most common symptom of the patients who died.17
SARS-CoV-2 infection can trigger and aggravate previous clinical problems in patients.1 The presence of cardiovascular pathologies in COVID-19 has been associated with both increased prevalence and mortality risk.24 A review reported several works that point to cardiac diseases as a predictor for hospitalisation and mortality, once during the COVID-19 infection could trigger mechanisms to a progression for cardiac damages.31 In fact, unspecified cardiovascular-related deaths increased in patients with COVID-19 in six Brazilian capitals with the highest COVID-19 death tolls, after 6 months of the pandemic. In our study, hypertension and heart disease corresponded to almost 18% of the comorbidities previously diagnosed in the study population, which is similar to findings from other studies around the world.
In addition to cardiovascular diseases, obesity is also reported as a strong risk factors for COVID-19. In our study, obesity showed the highest OR of death in non-hospitalised and ICU patients. Another striking predictor for COVID-19 deaths in this study was heart disease, diabetes, kidney disease, neurological diseases and cancer observed for non-hospitalised, non-ICU ward and ICU ward patients. Meta-analytical findings and epidemiological studies have ranked it among the leading comorbidities in individuals hospitalised with COVID-19.32 Multiple studies address the consequences of neurological precondition that may potentiate adverse effects from SARS-CoV-2, such as encephalopathy, critical illness neuropathy, critical illness myopathy and anosmia, which also can be reported as long term.33 Multisystemic illnesses could have played a relevant role in these deaths, considering that obesity augments the risk of inflammation and cardiovascular and metabolic diseases, while cancer is directly linked with immunosuppression, and neurological and kidney diseases are far more prevalent among older individuals.19 20 32
As seen in previous studies,21 the death rate differed drastically between non-hospitalised patients (0.55%), patients admitted to non-ICU wards (18%) and patients admitted to ICU wards (69.67%). After age as a predictor for severity, social factors are been related to increased risk of hospitalisation in indigenous, Asian and mixed populations, as well the authors suggest minority communities were exposed to high rates of infection due to social unequal conditions, which consequently led to hospitalisation.34
Nevertheless, death in critically ill patients was mostly related to dyspnoea and the aforementioned comorbidities. Our findings, identified in both groups of hospitalised patients, are in alignment with those of other studies, reinforcing the role of advanced age, gender and the comorbidities discussed previously in the adverse evolution of the disease.22 23 35 36 Martins-Filho et al reported that comorbidities including renal injury, and cardiovascular disease were independently associated with death among hospitalised patients with COVID-19. Gallo Marin et al37 in a review study highlights that COVID-19 hospitalised patients in USA, age older than 55 and male sex were associated with severity, as well as cardiovascular disease, chronic kidney disease, chronic lung diseases, diabetes mellitus, hypertension, immunosuppression and obesity. The same study reports Mexican patients with at least one comorbidity, such as a metabolic disorder, could have an increased risk of severe COVID-19-related diseases.37
Our comprehensive analysis was based on robust data collected from a period of almost one year, including carefully annotated and daily updated information. In addition, this study was unique in its inclusion of variables related to demographic characteristics, allowing for a better understanding of COVID-19 according to the social structure of the population in the distinct medical interventions (hospitalised and non-hospitalised patients). Nevertheless, limitations were encountered including incomplete and/or missing data patients’ for patients with COVID-19 due to ineffective filling database in the admission of cases for testing and health attendance system. For instance, the severity of symptoms and comorbidities was not available for further purposes. Including ethnicity as mentioned before has played a critical role in response to SARs-CoV-2; in the accessed database, it was incompletely filled in the most cases excluding the possibility to test if this variable was associated with mortality.
In conclusion, our major findings in the state of Paraná highlight the association of increases in the odds of death with over 35 years, male sex, dyspnoea, diabetes, heart disease, neurological disorders, chronic obstructive pulmonary disease, neoplastic disease, kidney disease, in all the intervention settings (non-hospitalised, non-ICU, and ICU-ward patients). These results provide a valuable source of information that can be translated into additional epidemiological COVID-19 studies and in well-annotated patient cohorts from distinct regions in Brazil and/or worldwide. They can also contribute to the management of public healthcare policies (such as staff training, treatment predictor and vaccination) in communities that are facing the continued spread of the COVID-19 pandemic with reduced mitigation measures, as in Paraná State and Brazil in general.
Data availability statement
Data are available upon request from authors.
Ethics statements
Patient consent for publication
Ethics approval
This study received the ethical approval number CAAE 39108020.0.0000.0107, registered on the Plataforma Brasil–Comissão Nacional de Ética em Pesquisa database (https://plataformabrasil.saude.gov.br).
Acknowledgments
The authors thank the Public Health Department of Paraná State, Brazil, for providing access to COVID-19 case data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
EGG-B and CEB contributed equally.
Contributors ECG-B and CEB contributed to the conception, design of the work and data acquisition, data curation, formal analysis, interpretation of data, draft of the manuscript, and review and editing. WAS, DLAF and MLP-E contributed to the conception, interpretation of data, manuscript draft, and review and editing. ABWB, LRC, CP and FFT contributed to data interpretation, manuscript draft, and review and editing. JPT, FACF, GWW, LCL, LEDF, IMdO, EC, LED and ANCS contributed to the manuscript’s draft and review and editing. All authors approved the final version to be published and accepts the full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This work was supported by Araucária Foundation–FAAP-PR, State Secretariat of Science, Technology and Higher Education– SETI–PR (grant number TC35/2020). ABWB was supported by scholarship CNPq-314288/2018-0.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.