Article Text

Abstract
Objectives We aimed to describe access to food and symptoms of depression among patients with chronic diseases or their caregivers, and assess associated factors during the COVID-19 lockdown in rural Rwanda.
Design A cross-sectional study.
Setting and participants A stratified random sampling technique was used to recruit 220 patients enrolled in the HIV, non-communicable diseases, mental health, paediatric development clinic and oncology programmes in three rural districts of Rwanda.
Outcome measures Telephone-based interviews were conducted to collect data on the number of daily meals before and during the COVID-19, and depression was assessed using the Patient Health Questionnaire-9. We used logistic regression analysis to investigate factors associated with households reporting a reduction in daily meals and with the survey respondent reporting symptoms of depression.
Results Of the participants, 19.1% reported a reduction in daily number of meals for either adults or children in their households during lockdown and 24.6% had depression. Reporting a reduction in daily meals was associated with the district of residence and estimated household’s monthly income. Self-reported depression was significantly associated with negative experiences during lockdown, including reporting feeling depressed or fear (AOR 4.82; 95% CI 2.08 to 11.21), loneliness (AOR 4.33; 95% CI 1.32 to 14.13), reduction in daily meals (AOR 4.15; 95% CI 1.56 to 11.00) and lack of access to healthcare (OR 3.29; 95% CI 1.32 to 8.23).
Conclusions Our findings suggest that significant reduction in access to food affected rural Rwandans with chronic diseases during COVID-19 lockdown, and the lockdown effect varied by household’s pre-pandemic level of vulnerability to food insecurity. Reduction in household meals, as well as other self-reported effects of the lockdown, were associated with worse psychological status of survey respondents. Economic and food support should be considered by governments and non-governmental organisations to protect those most vulnerable including patients with chronic diseases against the effects of pandemics and their associated containment measures.
- COVID-19
- public health
- mental health
Data availability statement
Data are available upon reasonable request. Data are not publicly available, but access may be obtained from the authors upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The Patient Health Questionnaire-9, a standard nine questions tool previously validated in the Rwandan population, was used to measure the outcome variable of the level of depression among patients with chronic diseases or their caregivers.
We measured access to food in the household using self-reported data on the number of daily meals for children and adults in normal circumstances and that was eaten during the COVID-19 lockdown (on the day prior to the survey date).
Reporting on the number of daily meals in normal circumstances was not defined in terms of time, which might have reduced data accuracy on daily meal consumption before COVID-19.
Data were self-reported and collected via telephone, which might have made it vulnerable to social desirability bias.
Due to the nature of a cross-sectional study design, we could not establish a link between experiences during the COVID-19 lockdown and the level of depression or between socioeconomic status indicators and changes in meal frequency.
Introduction
In response to the COVID-19 pandemic, many countries have adopted lockdowns as a strategy to curb the spread of the virus. While lockdowns have proven to be an effective strategy to contain the spread of COVID-19 and reduce transmission,1 2 they have also negatively impacted the overall physical, economic, mental, social and spiritual health of the people.3 Lockdowns have disrupted food supply chains both within and between countries, and the resulting income losses and threatened livelihoods have caused hunger and food insecurity.4–6 According to the United Nations (UN) data, between February and June 2020 alone, 45 million people became acutely food insecure, with most located in South and Southeast Asia (33 million) and sub-Saharan Africa (12 million).7 According to the World Food Programme,8 COVID-19 is expected to increase the number of acutely food insecure people in East Africa by 73%. In addition, the effects of the COVID-19-related lockdowns, including loss of jobs, loneliness and lack of access to routine care, have been reported to be associated with increased depression, anxiety and stress levels,9 10 while people living with other chronic health conditions are highly affected.11–13
Low-income households and households who rely on informal sources of income have been hit the hardest because they depend on daily wages for a living. In these households, strict lockdowns have created dual burdens of psychosocial and socioeconomic insecurity, especially among people experiencing a loss of livelihood.14 Even in the absence of the loss of livelihood, social isolation, interruptions of daily routines and reduction in leisure activities have been expected to negatively affect people’s mental well-being during lockdown.10 15 16 As the COVID-19 pandemic continues, countries need to balance policies centred around the need to stop the spread of COVID-19 with policies that mitigate the negative impacts of lockdown on food security, livelihoods and mental health (MH).17 18
In Rwanda, after the first COVID-19 case was confirmed on the 14 March 2020, a strict nationwide lockdown was enforced from 22 March 2020 to 3 May 2020. Subsequently, the restriction was partly relaxed in phases.19 During the lockdown period, travel between cities and districts was prohibited, non-essential shops and markets were closed, unnecessary movements outside of home were not permitted, all non-essential employees had to work from home and all borders were closed. Although the government of Rwanda implemented food provision programmes to vulnerable families to mitigate the negative effects of lockdown, the emergency food support was not adequate during the extended lockdown measures because it was provided during the first 2 weeks of lockdown and after that it was provided only on few occasions, leaving many vulnerable populations in need of emergency food support. However, the effects of Rwanda’s lockdown on vulnerable populations, including patients with chronic conditions, have not been previously studied. In 2020, the HIV/AIDS prevalence was estimated at 2.6% among adults aged 15–49 years in Rwanda.20 In addition, by 2017, approximately 27 000 patients with non-communicable diseases (NCDs) (including 70% hypertension, 19% type 2 diabetes, 5% chronic respiratory disease, 4% type 1 diabetes and 2% heart failure patients) were enrolled at 42 outpatient NCD clinics across Rwanda.21
Partners In Health/Inshuti Mu Buzima (PIH/IMB) is a non-governmental organisation that supports health system strengthening across three rural Rwanda districts. Between 23 April and 11 May 2020, PIH/IMB conducted a cross-sectional telephone survey among chronic care patients in order to better understand patient’s needs and experience during lockdown. In this paper, we describe self-reported access to food and symptoms of depression among patients with chronic diseases and their caregivers during the lockdown and assess factors associated with food insecurity and depression.
Methods
Study design and setting
Rwanda is administratively divided into four provinces (East, North, South and West) and the city of Kigali, with 30 districts under them. By June 2020, there were 8 national referral hospitals, 4 provincial hospitals, 37 district hospitals and 510 primary health centres associated with them in Rwanda.22 Each of the 30 districts had at least 1 district hospital. Burera district is located in the Northern province, while Kayonza and Kirehe districts are located in the eastern province. We conducted this cross-sectional study in the catchment areas for Rwinkwavu, Kirehe and Butaro district hospitals, in Kayonza, Kirehe and Burera districts, respectively. These public health facilities, which have been supported by PIH/IMB since 2005, supervise a total of 8, 16 and 19 primary health centres, respectively, and serve a population of about one million people.23 Over 24 500 patients with chronic conditions were actively followed through different chronic care programmes at these facilities at the time of the lockdown.
Study population
Patients were eligible for inclusion in the survey if they were enrolled in HIV, NCD, MH, paediatric development clinic (PDC) and oncology programmes at health facilities in the Rwinkwavu, Kirehe and Butaro catchment areas, being active patient defined by having a clinical appointment scheduled between April and June 2020, and had a phone number recorded in the electronic medical records (EMR) system. Primary caregivers were allowed to report on behalf of patients aged<18 years or patients who were too ill to respond to the survey questions.
Study sample
Eligibility criteria for this study were: being enrolled in one of the five chronic care programmes and an active patient with a clinical visit scheduled between March and June 2020; resident of Kayonza, Kirehe or Burera districts; and having a telephone number recorded in the EMR system. We stratified our eligible chronic care patient population by district and clinical programme and randomly selected patients from each stratum. The goal was to randomly select at least 48 patients in each stratum (16 patients from each district where applicable), for a total sample size of 240 so that program-specific estimates could be reported with 95% CIs and ±15% precision. Ultimately, 220 patients were recruited for this study, mainly due to a low proportion of patients with a valid telephone number recorded in the EMR system—full details on the sample flowchart can be found elsewhere.24
Data source and definition of key variables
Survey interviews were conducted during the lockdown between 23 April and 11 May 2020. These were computer-assisted telephone interviews administered using REDCap.25 26 They were conducted by six experienced data collectors. Data collectors called each sampled patient at least once on three separate days, and patients who could not be reached were replaced with another individual from the same district and clinical programme from the call list. In this analysis, we focused on describing access to food and symptoms of depression among survey participants and to assess associations between their socioeconomic characteristics, self-reported effects of the COVID-19 lockdown and food insecurity, and having symptoms of depression. Depression among survey respondents was assessed using the Patient Health Questionnaire-9 (PHQ-9), a standard nine questions tool which was previously translated in Kinyarwanda and validated in the Rwandan population in a study that involved epilepsy patients.27 The classification of the level of depression was determined based on the total PHQ-9 score, with participants classified as being not depressed (PHQ-9≤4) or having mild (5≤PHQ-9≤9), moderate (10≤PHQ-9≤14), moderately severe (15≤PHQ-9≤19) and severe depression (20≤PHQ-9), using standardised cut-offs.28 A PHQ-9 total score≥10 indicated ‘having symptoms of moderate-to-severe depression’. The survey also asked respondents to self-report on the number of daily meals for children and adults in their household in normal circumstances as well as the number of daily meals eaten on the day before the survey date (during the COVID-19 lockdown). Four survey questions were used to collect this information, respectively: (1) in normal circumstances, how many meals per day do adults get? (2) yesterday, how many meals did adults get? (3) in normal circumstances, how many meals do children get per day (children under age 5)? and (4) yesterday, how many meals did children get (children under age 5)? A ‘reduction in daily meals during lockdown’ was defined as the survey respondent reporting fewer meals per day for adults or children during the COVID-19 lockdown compared with usual.
The survey also included an open-ended question that allowed respondents to report on any life changes due to the COVID-19 lockdown. Respondents were asked ‘how have COVID-19 and the changes due to COVID-19 affected your life?’ with pre-defined response options including: (1) feeling depressed; (2) lack of food; (3) loss of income; and (4) lack of access to healthcare. For this type of question, interviewers were instructed not to read these response options, but to use ‘anything else’ as a probe for exhausting the respondent’s response, while the ‘other’ option was used to record any response that was not captured in the predefined categories. The ‘socioeconomic status’ of respondents was measured using the 2015 Rwandan Government’s Ubudehe categorisation of households—a four-level categorisation ranging from 1 (poorest) to 4 (richest).29 Category 1 included people who belong to families that do not own a house and struggle to afford basic needs, while category 3 included households that have members with a full-time job or farmers who can go beyond subsistence farming.
Other characteristics of respondents included patient’s ‘clinical programme’ (HIV, NCD, MH, PDC and oncology programmes). The NCD programme included patients with diabetes, asthma, hypertension and heart failure. The MH programme includes patients with epilepsy, depression and other MH disorders. The PDC programme provides clinical and nutritional follow-up to under-5 children who were discharged from hospital neonatology care units after being born preterm, with low birth weight and/or with hypoxic ischaemic encephalopathy. Oncology programme provides treatment and care for both paediatric and adult cancer patients. The patient’s ‘district of residence’ (Kayonza, Kirehe and Burera districts) and ‘respondent type’ (patient vs caregiver) were also reported as characteristics of survey respondents. The respondent’s ‘level of education’ was assessed in the survey using a multiple choice question with the following categories: (1) no formal education, (2) any primary, (3) any secondary, (4) any university and (5) other. The ‘livestock ownership’ was assessed using a (yes/no) question with a follow-up question to specify the type of livestock owned. The existing literature suggests an association between livestock ownership and household food security in Sub-Saharan Africa.30 Respondents were also asked to report on the estimated usual ‘household monthly income’ in Rwandan francs (RWF) with the following predefined response categories: (a) zero, (b)<30 000, (c) 30 000–49 000, (d) 50 000–100 000 and (e)>100 000, and source of income. The preidentified response options for the household’s ‘source of income’ included: (a) no income, (b) agriculture, (c) business, (d) monthly salary and (e) other.
Data analysis
We described patients, caregivers and households’ characteristics using frequencies and percentages for categorical variables and median and interquartile ranges (IQR) for continuous variables. We used Wilcoxon matched-pairs signed-ranks tests to compare the distributions of the number of daily meals before COVID-19 and during the COVID-19 lockdown. In the univariate analysis, Fisher’s exact and Wilcoxon ranksum tests were used to measure associations with outcomes for categorical and continuous data, respectively.
We used a multivariable logistic regression model built using backward stepwise to assess (a) socioeconomic characteristics associated with experiencing meal reduction in the household and (b) socioeconomic characteristics of survey respondents that predicted symptoms of moderate-to-severe depression. In both cases, our final model included all variables with a p value<0.20 so that our search for relationships and patterns in our data could be maximised. We also forced two variables into the final models regardless of their p values: type of survey respondent, which we hypothesised would impact the quality of data on food security, with caregivers being more accurate than patients, and patient’s clinical programme, as some of the clinical programmes normally provide food support to patients to complement their treatment. We also expected a differential risk of depression due to the study respondent being the patient or caregiver, as well as by the health condition/clinical programme. Finally, for each self-reported experience during the lockdown, we fit a model assessing the association between that experience and reporting symptoms of moderate-to-severe depression after adjusting for all variables identified in our previous model as socioeconomic predictors of depression. These variables were assumed to be potential confounders based on their association with the outcome. Wald tests were used to calculate p values for variables in the multivariable logistic regression models. All data were analysed in Stata V.15.1 (Stata Corp, College Station, Texas, USA).
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
In total, 220 respondents participated in the survey (table 1). In total, 68% of the respondents were patients themselves, while 70 (31.8%) respondents were caregivers. Patients were sampled from the NCD (n=50, 22.7%), HIV (n=49, 22.3%), PDC (n=47, 21.4%), MH (n=43, 19.6%) and oncology (n=31, 14.1%) programmes. Of 215 respondents with data on education, 48 (22.3%) did not attend any formal education, while 44 (20.5%) had a secondary or higher level of education. Self-reported experiences during lockdown included the loss of income (n=100, 45.4%), lack of food (n=81, 36.8%), feeling depressed or having fear of infection (n=51, 23.2%), lack of access to healthcare (n=32, 14.6%) and loneliness or lack of social events (n=19, 8.6%).
Socioeconomic characteristics of study participants and self-reported effects of the COVID-19 lockdown
In addition, the survey collected data on households’ characteristics for respondents. In total, 89% of households owned a house and the median household size was 5 members (IQR: 4–6 members). In total, 34% of survey participants reported no regular monthly income for their households, while 117 (53.2%) were from households that had a usual estimated monthly income less than 30 000 RWF (approximately US$30). The household’s income was exclusively from agriculture for 115 (52.3%) respondents, and 20.0% reported having no stable source of income in their households. In total, 36% reported having any livestock in their households, while 38 (17.3%) were in the poorest socioeconomic class (Ubudehe category 1).
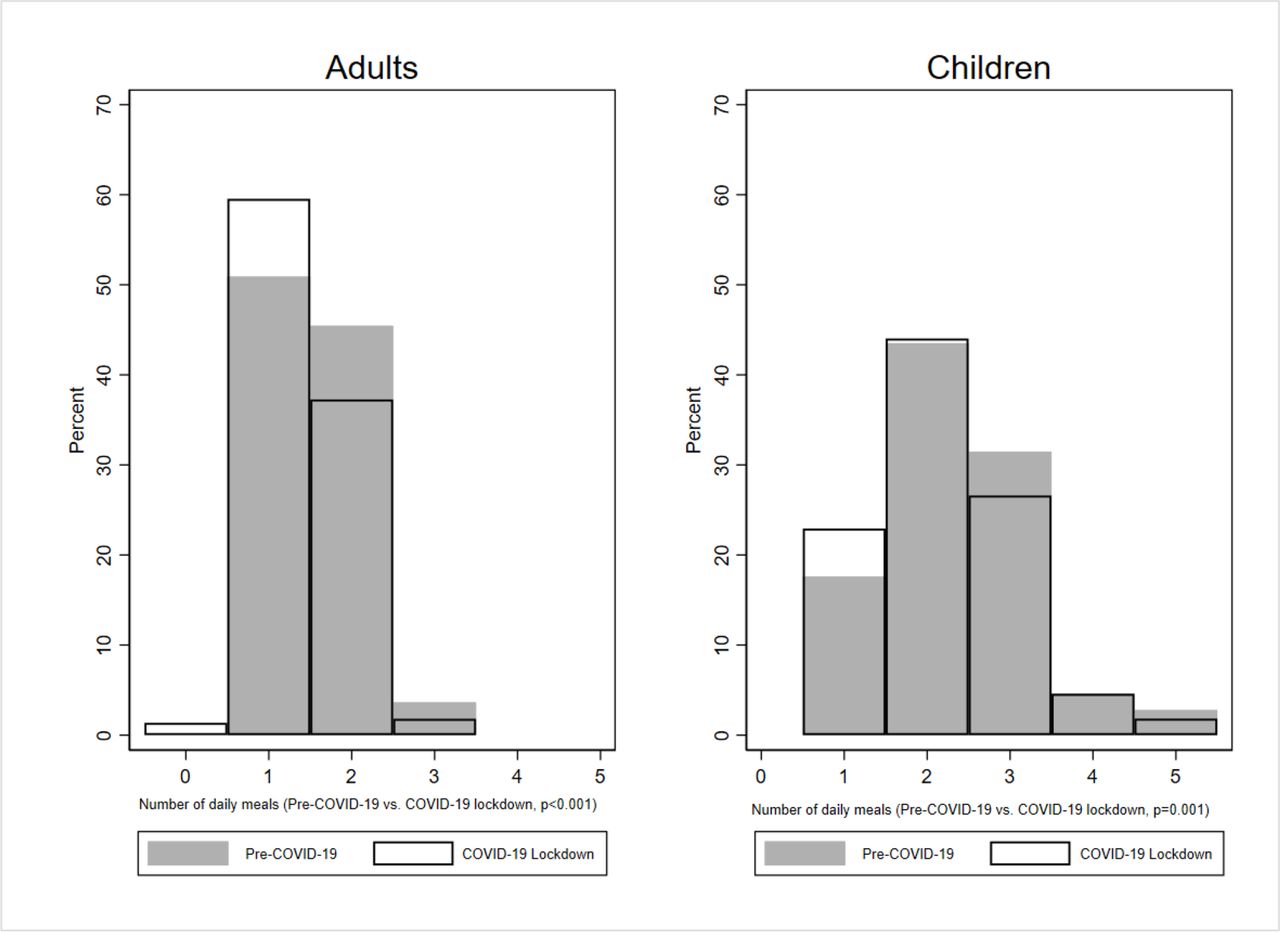
Overall, 19.1% of respondents reported a reduction in the daily number of meals for either adults or children in their households during lockdown (figure 1, table 2). The median number of meals consumed per day remained one meal (IQR: 1–2) for adults and two meals (IQR: 2–3) for children before and during the lockdown. However, there was a significant negative change in the distributions of the number of daily meals from pre-COVID-19 to during the COVID-19 lockdown for both adults (p<0.001) and children (p=0.001). Results from the adjusted logistic regression model indicate that reporting a reduction in the daily number of meals in the household varied significantly by district of residence and estimated household monthly income. Compared with survey participants from Kayonza district, the odds of reporting a reduction in the daily number of meals were reduced by 80% in Burera district (AOR 0.20; 95% CI 0.07 to 0.60) and by 63% in Kirehe district (AOR 0.37; 95% CI 0.15 to 0.86). The odds of reporting food reduction among households with<30 000 RWF monthly income being 2.53 times (AOR 2.53; 95% CI 1.05 to 6.08) higher compared with households with no stable income. The point estimate for a household monthly income≥30 000 RWF indicates lower odds of reporting food reduction (AOR 0.70; 95% CI 0.17 to 3.00); however, the confidence interval (CI) was not statistically significant. There was no evidence of association between experiencing a reduction in daily meals and other baseline household socioeconomic status indicators, including Ubudehe category, household size, estimated household monthly income, household source of income and the household having livestock.
Predictors of reporting a reduction in daily meals in the household during the COVID-19 lockdown
{kind=link}
Per cent distribution of households by number of daily meals for children and adults before and during COVID-19 as it was self-reported by patients or caregivers. Grey colour: Pre-COVID-19. White colour: During COVID-19 lockdown.
Overall, 54 (24.6%) participants (22.7% of patients with chronic diseases and 28.6% of their caregivers) had symptoms of moderate-to-severe depression (95% CI: 19.0% to 30.8%, table 3 and online supplemental table 1). Among the socioeconomic characteristics of the study participants, the identified predictors of depression included the district of residence, reporting having livestock in the household and household’s source of income. Compared with participants from Kayonza district, the odds of depression were 3.24 times higher (AOR 3.24; 95% CI 1.34 to 7.85) than for participants from Kirehe district and 12% lower for participants in Burera district (AOR 0.88; 95% CI 0.30 to 2.57). The report of having livestock in the household was significantly associated with a 61% reduction in the odds of depression (AOR 0.39; 95% CI 0.17 to 0.87). For the household’s source of income, the odds of depression among participants who reported no stable monthly income were 3.07 times higher (AOR 3.07; 95% CI 1.27 to 7.41) than participants who reported their household’s source of income as exclusively agriculture. However, not statistically significant, lower odds of depression were observed among participants who reported sources of income other than agriculture (AOR 0.98; 95% CI 0.39 to 2.50).
Supplemental material
Predictors of depression
For the association between negative experiences during the COVID-19 lockdown and having symptoms of moderate-to-severe depression, after adjusting for the type of survey respondent (patient or caregiver), patient’s clinical programme, district of residence, household size, having livestock in the household and household source of income, increased odds of depression were significantly associated with reporting feeling depressed or fear (AOR 4.82; 95% CI 2.08 to 11.21), reporting loneliness or lack of social gatherings (AOR 4.33; 95% CI 1.32 to 14.13), experiencing a reduction in household usual number of daily meals (AOR 4.15; 95% CI 1.56 to 11.00) and lack of access to healthcare (OR 3.29; 95% CI 1.32 to 8.23) (table 4). There was no statistically significant association between depression and reporting loss of income or lack of food during the lockdown.
Assessing the association between COVID-19 experiences and depression
Discussion
This study assessed the food insecurity and level of depression, and associated factors among patients with chronic diseases or their caregivers during the COVID-19 national lockdown in Rwanda. We found that almost one out of every five households included in our survey reported a reduction in daily meals during the COVID-19 lockdown. Similar findings have been reported in Bangladesh, where 15% of rural households have experienced a reduction of meal frequency during lockdown.14 The odds of reporting a decrease in daily meal consumption significantly varied by geographical location (district of residence), with lower odds of meal reduction being observed among survey respondents from Burera and Kirehe districts compared with Kayonza district. This finding is consistent with the Rwanda 2018 comprehensive food security and vulnerability analysis which indicates that even before the COVID-19 pandemic, Kayonza was already more vulnerable to food insecurity with 32.7% food insecure households compared with 29.7% and 22.6% food insecure households in Kirehe and Burera districts, respectively.29 Another identified significant predictor of reporting a reduction in the daily meal consumption during the lockdown is the estimated household’s monthly income, where households with a relatively medium monthly income were more likely to report a reduction of meal frequency during the COVID-19 lockdown compared with households with no income. Similar findings have been reported in South Africa, where COVID-19 related lockdowns affected middle income households more than lower income households because lower income houses receive significant government assistance, which persisted during the lockdown.5 Particularly, with this study population of chronic care patients, in a context with widespread food insecurity, adequate nutrition support would become an important predictor of improved clinical outcomes. For example, food insecurity predicts stunting and supplemental food packages are associated with better outcomes among HIV patients.31 32
A quarter of our survey respondents reported moderate-to-severe depression. As has been noted in other settings, our study found that being a caregiver for someone with a chronic condition, having cancer and having an NCD was associated with higher prevalence of depression.33 Even after adjusting for these variables, experiencing hardships during the lockdown, including experiencing a reduction in daily meals, loneliness, fear or lack of access to healthcare, was associated with increased odds of moderate-to-severe depression. Associations between lockdowns, food insecurity and poor MH have been observed elsewhere, including in Bangladesh.14 In the context of chronic care patients, the combination of depression and poor nutrition is particularly concerning because it can affect the management of chronic conditions through poor medication adherence.34 35 During COVID-19, evidence-based interventions for MH, such as the cognitive–behavioural therapy,17 18 could be adopted to support patients with chronic diseases in Rwanda. Access to vaccine could also positively affect the psychological status of these vulnerable people.
This survey highlights the importance of having a short-term plan for socioeconomic support of vulnerable populations, including chronic care patients during times of unexpected crisis. During early days of the COVID-19 pandemic, communities in many developing countries have expressed the urgent need for socioeconomic support from their governments, including food and direct cash support to vulnerable households as a response to the effects of the pandemic.36 As economic crises continue, these countries have to depend on emergency packages from the government, which might not be adequate to cushion them and their vulnerable population.36 37 Expansion of existing social and food support programmes can mitigate the risk of economic shocks in times of future crisis. However, our survey highlights that even chronic care patients who are economically stable in normal times can become vulnerable in times of crisis. Consequently, clinical programmes may need to explicitly target these patients for support to ensure proper management of their chronic conditions. In addition to preparing a short-term plan for acute crises, chronic care patients may benefit from longer-term economic support that uses a livelihood approach to create resilience before the next crisis. In contrast to short-term solutions such as cash transfers and food baskets, the livelihood model focuses on evolving thinking about the way the poor and vulnerable live their lives and the importance of policies and institutions in reducing poverty and inequality by moving vulnerable households towards economic stability.
This study has several limitations. First, data were collected via telephone and patients with active phone numbers likely had higher income than the average patient. However, in the context of a national lockdown, telephone surveys were the only way to reach patients. Moreover, the observed distribution of patients by socio-economic class known as ‘Ubudehe’ was similar to the national distribution.29 Second, self-reported data may be vulnerable to social desirability bias. However, patients were not promised financial or other forms of assistance for responding to the survey, and we therefore believe they did not have a strong incentive to provide wrong information. Third, the sample of this study exclusively included people living in rural settings and therefore our results may not reflect the impact of COVID-19 lockdown on food security and MH of patients with chronic diseases who were living in urban areas. A differential psychological impact of COVID-19 by the type of residence has been reported elsewhere.38 39 The change in daily meal consumption during the lockdown was measured by comparing the number of daily meals on the day before the survey during lockdown and normal circumstances before COVID-19—however, the latter was not defined in terms of time, which might have reduced the accuracy of reporting on daily meal consumption before COVID-19. Additionally, because this was a cross-sectional study, we cannot establish a temporal link between socioeconomic status indicators and changes in meal frequency or between experiences during lockdown and depression. However, most of our socioeconomic status indicators, including respondent education, Ubudehe category, household size and occupation, would not be expected to change during lockdown and likely reflect pre-lockdown conditions.
Conclusions
We observed that approximately one out of five households of patients with chronic conditions reported a reduction in daily meals during Rwanda’s COVID-19 lockdown and that 23% of patients with chronic diseases and 29% of their caregivers reported symptoms of moderate-to-severe depression during this time. Reporting daily meal reduction in the household among our study population during the pandemic significantly varied by the pre-existing level of vulnerability to food insecurity. Our findings also indicate a significant association between the negative COVID-19 experiences including lack of access to healthcare, meal reduction and lack of social events and loneliness and increased risk of depression among patients with chronic diseases and their caregivers. Economic, food and mental health support should be taken into consideration by governments and non-government organisations to support those most vulnerable including patients with chronic diseases to the effects of the COVID-19 pandemic and prepare for instantaneous interventions during future pandemics or crises in Rwanda and other resource-limited settings.
Data availability statement
Data are available upon reasonable request. Data are not publicly available, but access may be obtained from the authors upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by patients or their primary caregivers who were aged 18 years or older responded to the survey after providing verbal consent for their voluntary participation. In addition, this study received approval from the Partners In Health/Inshuti Mu Buzima (IMB) research committee and the Rwanda National Ethics Committee (RNEC) under the IMB clinical programs research umbrella protocols. (Mental health: 196/RNEC/2020; non-communicable disease: 910/RNEC/2019; HIV: 015/RNEC/2020; oncology: 805/RNEC/2019; and paediatric development clinic: 713/RNEC/2019.) Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We want to thank Partners In Health/Inshuti Mu Buzima that funded the data collection activities for this study. We are also grateful for the collaboration and patience of the patients and/or their caregivers across the five chronic care programmes who made time to respond to the survey questions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SU and AN designed the study, interpreted results and drafted the manuscript. AN verified the raw data set and conducted the analysis. AN is the guarantor for the data used for the analysis. DAB provided methodologic assistance on study design, oversaw statistical analysis and critically reviewed the manuscript. VKC and JMM designed the study, supported interpretation of results, analysis and critical reviews of the manuscript. SD, EM and EN contributed to results interpretation and manuscript revision. All authors have read and approved the final manuscript.
Funding Partners In Health/Inshuti Mu Buzima supported the data collection activities.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.