Article Text

Abstract
Objectives It remains unclear whether vitamin D status is related to cancer risk. We examined this relationship using laboratory, administrative and survey data.
Design Retrospective cohort study.
Setting All care settings within Calgary, Alberta, Canada and surrounding rural communities.
Participants Patients tested for serum 25-hydroxyvitamin D from 2009 to 2013 without a past cancer diagnosis but with an ECG and body mass index ±3 months from testing were included. Age, sex, mean hours of daylight during month of testing were linked to census dissemination area-level indicators of socioeconomic status measured in 2011.
Primary and secondary outcome measures Hospital discharge diagnoses for any cancer, major cancer (colorectal, breast, lung, prostate, skin) and other cancers >3 months from testing from 2009 to 2016. Cox proportional hazard models were used to examine associations with incident cancer after adjusting for potential confounders. Interactions were tested using multiplicative terms.
Results Among 72 171 patients, there were 3439 cancer diagnoses over a median of 5.9 years. After adjustment, increasing quartile of serum 25-OH vitamin D was significantly associated with an increased risk of any cancer and major cancer, however this was completely driven by an increased risk of skin cancer (Q4 vs Q1: HR=2.56, 95% CI 1.70 to 3.86, p for linear trend <0.01). This association was strengthened among individuals residing in communities with higher proportions of non-citizens, recent immigrants, visible (non-white) minorities and those not speaking an official Canadian language (English or French) at home.
Conclusions Higher vitamin D status was associated with a greater risk of skin cancer in a large community population under investigation for cardiovascular disease. This association was likely due to sun exposure and may be modified by community variation in vitamin D supplementation.
- epidemiology
- clinical chemistry
- statistics & research methods
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We assembled a large retrospective cohort study of community patients by linking patient laboratory, national survey and hospital administrative data during a time of high public and medical interest in vitamin D deficiency, and a commensurately high testing rate at our laboratory for serum 25-hydroxyvitamin D.
Linkage allowed us to control for body mass index, a confounder of 25-hydroxyvitamin D-chronic disease relationships and to explore variation in associations according to community-level socioeconomic factors correlated with vitamin D supplement use.
As our study was restricted to patients who had received an ECG, it may not be generalisable to all patients.
Introduction
Vitamin D deficiency is defined as a serum 25-OH (hydroxy) vitamin D concentration <50 nmol/L,1 2 which causes reduced absorption of dietary calcium and phosphate and increases the risk of rickets in children and osteomalacia in adults.1 Conversely, vitamin D toxicity is generally regarded to occur above 250 nmol/L—when symptoms of hypercalcaemia begin to occur.3
Vitamin D deficiency is relatively common—especially in Northern latitudes where people experience less intense solar radiation, spend more time indoors due to cold and experience prolonged periods of darkness during winter.4 In Canada, 33% of residents may be vitamin D deficient.5 As such, there remains significant interest in whether vitamin D deficiency is related to many common diseases—particularly cancer.
Meta-analysis of prospective cohort studies suggest that vitamin D deficiency is associated with an increased risk of multiple types of cancer, including all cancers,6 colorectal cancer,7 bladder cancer8 head and neck cancer,9 liver cancer10 and also death due to cancer.11 These associations have been explained by in vitro and in vivo effects of the active form of vitamin D (1,25 OH2 (dihydroxy) vitamin D), which promotes cellular differentiation, decreases cancer cell growth, stimulates cell death (apoptosis) and reduces angiogenesis.12 However, associations may also be explained by the presence of confounding factors that are associated with vitamin D deficiency and a higher risk of cancer.
For example, adiposity is a sink for and diluent of serum 25-hydroxyvitamin D13 as well as a risk factor for several types of cancer.14 As such, adjustment for some measure of adiposity (eg, body mass index (BMI)) is generally recognised as essential to control for bias in epidemiological studies of serum 25-hydroxyvitamin D concentration and cancer risk.1 Interestingly, low socioeconomic status (SES), while also a strong a risk factor for vitamin D deficiency15 and cancer,16 is infrequently controlled for—probably because it is uncommonly measured in epidemiological studies.
Historic uncertainty in the validity of epidemiological findings have thus lead the Institute of Medicine in the USA to indicate that evidence of a relationship between vitamin D status and non-skeletal chronic disease does not meet criteria for establishing cause-and-effect.1 However, vitamin D status could still be a useful and convenient cancer risk marker if its association with cancer risk is independent of other commonly measured factors and is observed in a large population of free-living individuals.
Our objectives were therefore to (i) examine the relationship between serum 25-hydroxyvitamin D (the major circulating form of vitamin D) and risk of cancer in a large community-based population, (ii) adjust for important confounders such as adiposity and SES and (iii) test whether associations are modified by these and other factors.
Materials and methods
Patient and public involvement statement
Due to the design of the study and because we did not collect the primary data, we did not involve patients or the public in the design, conduct or reporting of our research.
Population, primary exposure variable and covariates
We used the Cerner (Kansas City, Missouri, USA) Millennium laboratory information system (LIS) to identify those who had a serum 25-hydroxyvitamin D result with a test date from 8 December 2009 to 1 April 2013. This database contained all laboratory results on patients tested in Calgary, Alberta, Canada (population ~1.4 million) as well as surrounding rural communities. During the time of this study, 25-hydroxyvitamin D testing was available to any ordering physician for any reason—and high test volumes (~16 000/month) reflected a strong public and medical interest in vitamin D deficiency. For these patients, we retained data only for those who had an ECG because these patients had a self-reported height and weight entered into the LIS to calculate BMI (weight in kg/(height in m)2). We then extracted age, sex and the provincial healthcare number to link to hospital administrative outcome data and postal codes. As vitamin D status is related to sun exposure, we also calculated mean hours of daylight during month of 25-hydroxyvitamin D testing for each person based on publicly available data.17 This was done so that we could adjust for short-term variation in 25-hydroxyvitamin D related to seasonal changes in sun exposure at the time of testing. All serum 25-hydroxyvitamin D tests were performed on the DiaSorin (Saluggia, Italy) Liaison total 25-hydroxyvitamin D automated immunoassay platform, which predominantly detects 25-hydroxyvitamin D3.18 The performance of this assay was validated using guidelines from the Clinical Laboratory Standards Institute (Annapolis Junction, Maryland, USA). Total imprecision was approximately 7%, and results from external proficiency survey samples from the Vitamin D External Quality Assessment Scheme all fell within total allowable error intervals from peer group means (<20 nmol/L: ±5 nmol/L; ≥20 nmol/L: ±15 nmol/L).
Census dissemination area (CDA)-level SES covariates were obtained from the 2011 Canadian National Household Survey after postal code to CDA conversion. We extracted proportion of CDA residents who were (i) Canadian citizens, (ii) recent immigrants, (iii) visible (non-white) minorities, (iv) those speaking languages other than English and French (official languages of Canada) at home, (v) those having postsecondary education, (vi) those currently employed and the CDA (vii) median household income.
Outcomes
In-hospital discharge diagnosis and dates were obtained from the Discharge Abstract Database and National Ambulatory Care Reporting System via Alberta Health Services. Incident cancers were defined as the first and most responsible (primary) diagnosis of any cancer (International Classification of Diseases, Tenth Revision codes: C00.x-C97.x), if the patient was discharged alive or died in hospital. We further subdivided ‘any cancer’ into ‘major cancer’19 (breast (C50.x), colorectal (C18.x-C21.x), lung (C33.x-C34.x), prostate (C61.x) and skin (melanoma: C43.x, non-melanoma: C44.x, C46.x),20 specific cancers (breast, colorectal, lung, prostate and skin) and ‘other cancer’—defined as ‘any cancer’ other than ‘major cancer’. At the time of analysis, outcome data were available until 31 December 2016.
Data cleaning
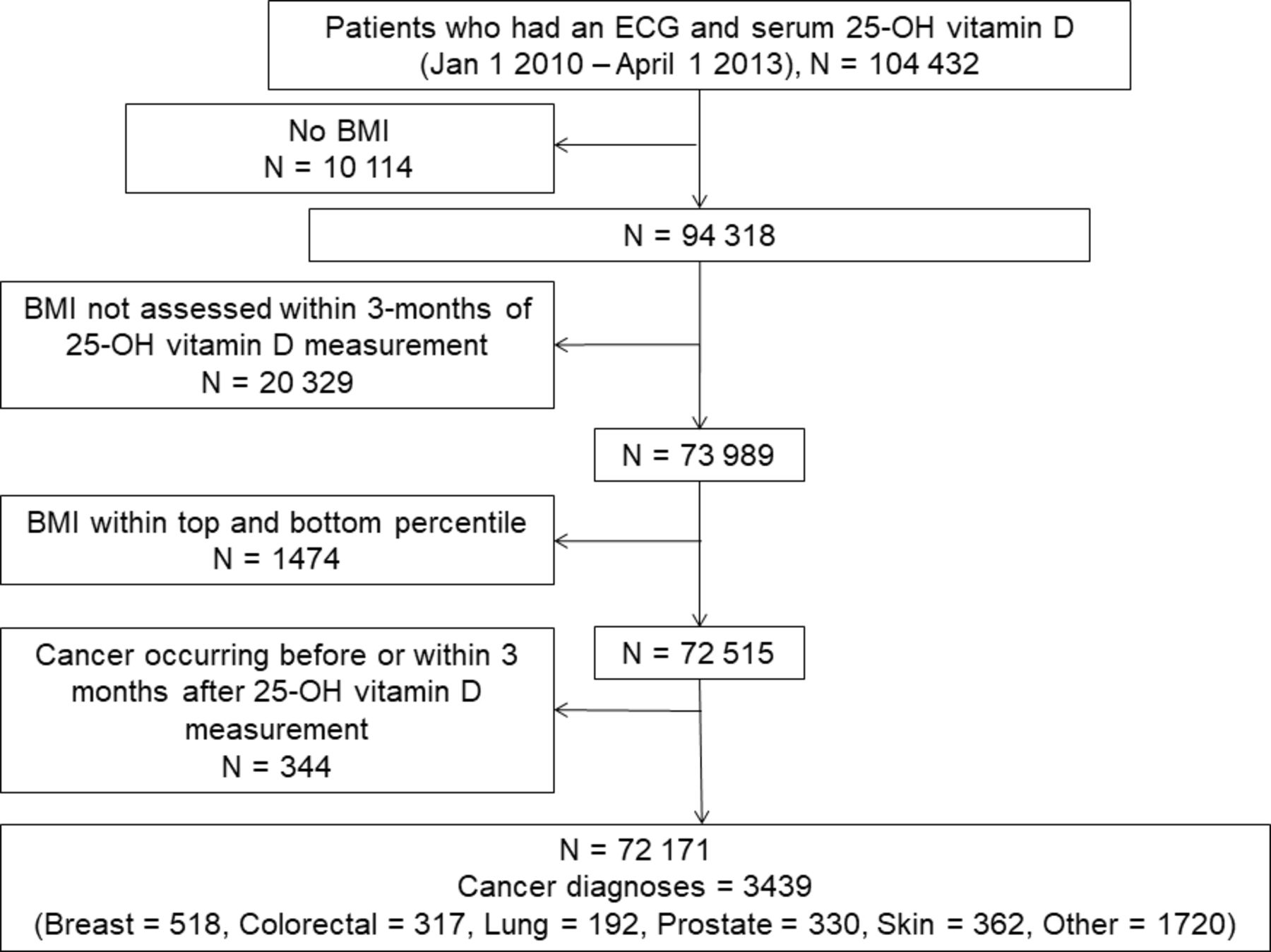
We kept only the first measurement of 25-hydroxyvitamin D to capture historic vitamin D status—which is more likely associated with cancer risk than vitamin D status after supplementation in response to an earlier diagnosis of deficiency. Patients were removed if BMI was measured beyond ±3 months from 25-hydroxyvitamin D testing or was within the top and bottom percentiles. Patients with cancer occurring before or within 3 months of 25-hydroxyvitamin D testing were eliminated to establish temporality and to reduce impact of behaviour changes or treatment (including supplementation) in response to subclinical or previous disease. The cohort design is shown in figure 1.

Cohort design. Serum 25-hydroxyvitamin D measurements were made between 2009 and 2013. Census dissemination area-level socioeconomic status covariates were measured in 2011. BMI, body mass index.
Statistical analysis
Patient characteristics were tabulated according to quartiles of serum 25-hydroxyvitamin D concentration. Linear trends for individual-level data were evaluated using linear and logistic regression. Linear trends for CDA-level SES covariates were evaluated using Poisson regression accounting for clustering of patients by CDA, and variance was calculated using a sandwich estimator.
The relationship between serum 25-hydroxyvitamin D quartile and incident cancer was evaluated using Cox proportional hazard models, with time from 25-hydroxyvitamin D testing to date of cancer diagnosis or censoring (26 December 2016) as follow-up time. For analyses of major and specific cancers, including ‘other’ cancer, those without the outcome of interest also included those without a diagnosis of any other cancer. We adjusted for age, sex, BMI, mean hours of daylight during month of testing and CDA-level SES covariates in different models. Models adjusted for CDA-level SES covariates accounted for clustering of patients by CDA, and variance was calculated using a sandwich estimator. Because we examined eight separate cancer outcomes, a Bonferroni correction (0.05/8) was applied to reduce the nominal significance threshold of p<0.05 to p<0.00625 in order to minimise type I error. We tested the proportional hazards assumption for each variable by inserting time-dependent covariates (eg, 25-hydroxyvitamin D quartile×log(time)) into models. If time-dependent covariates reached nominal significance, they were included in all outcome analyses for a given model.21
For 25-hydroxyvitamin D-cancer associations that reached the Bonferroni-corrected threshold of significance, we explored possible interactions with all covariates using multiplicative terms in Cox models, and evaluated them using the nominal significance threshold. For convenience, associations were stratified by the median value of these covariates. Finally, we performed a sensitivity analysis where we excluded participants with a 25-OH vitamin D concentration of 100 nmol/L or greater, as these individuals may be more likely to be taking vitamin D supplements.22
All data analysis was performed using Statistical Analysis Software (SAS V.9.4).
Results
After exclusions (figure 2), there were 72 171 patients for analysis and 3439 cancer diagnoses (major=1719; breast=518, colorectal=317, lung=192, prostate=330 and skin=362 (melanoma=58, non-melanoma=304); other=1720) over a median of 5.9 years of follow-up. Cancer diagnoses occurred after a median of 3.0 years. There were 2849 CDAs. Approximately 31% of patients were vitamin D deficient (ie, serum 25-hydroxyvitamin D <50 nmol/L).
{kind=link}
{kind=link}
Patient exclusions leading to analysis cohort. BMI, body mass index.
Mean age and daylight hours during month of testing significantly increased with serum 25-hydroxyvitamin D quartile whereas proportion of men and mean BMI significantly decreased. We also found that serum 25-hydroxyvitamin D was lowest when tested in the winter (median=61 nmol/L) versus the summer (median=69 nmol/L). Among CDA-level SES covariates, mean proportions of Canadian citizens, those with postsecondary education, employed individuals and the median total household income significantly increased with 25-hydroxyvitamin D quartile whereas the mean proportion of recent immigrants, visible minorities and those using non-official languages at home significantly decreased (table 1). The proportion of all cancer cases increased significantly across 25-hydroxyvitamin D quartile (table 1; p for trends <0.001).
Patient characteristics by quartile of serum 25-hydroxyvitamin D
Three Cox proportional hazards models were used to further evaluate the association of 25-hydroxyvitamin D and cancer risk: model 1: adjusted for age, model 2: model 1 adjusted for sex, BMI, mean daylight hours during month of testing and model 3: model 2 adjusted for CDA-level SES covariates. Vitamin D quartile met the assumption of proportional hazards (ie, no significant interaction with time) in every model, however several covariates did not and were therefore modelled using time-dependent covariates in each model.
After adjusting for age, associations with any cancer, major cancer, breast cancer and skin cancer exceeded the threshold for Bonferroni significance (table 2; p for trend <0.00625). Further adjustment for sex, BMI, mean daily hours of daylight during month of testing resulted in the association with breast cancer becoming non-significant at the Bonferroni threshold (table 2). Additional adjustment for CDA-level SES covariates resulted in only any cancer, major cancer and skin cancer remaining significant at the Bonferroni threshold. Importantly, the association with major cancer was no longer significant after removing cases of skin cancer (p for trend=0.15), confirming that this association was driven by the association with skin cancer, which was the strongest observed. Compared with the bottom quartile of serum 25-hydroxyvitamin D, participants in the top quartile had a 2.56X greater risk of skin cancer after adjusting for covariates. Analysis by type of skin cancer yielded a similar association for non-melanoma, but the association for melanoma was not significant at either threshold of significance—perhaps due to a small number of melanomas in our study(n=58; results not shown).
Cox proportional hazard regression of serum 25-hydroxyvitamin D quartile and risk of cancer
We observed four nominally significant interactions between 25-hydroxyvitamin D quartile and CDA-level SES covariates on skin cancer risk (table 3). For an increase in the CDA-level proportion of non-citizens, recent immigrants, visible (non-white) minorities and those not speaking official languages (English or French) at home, the individual-level association between 25-hydroxyvitamin D and skin cancer risk was stronger.
Association of serum 25-hydroxyvitamin D quartile with risk of skin cancer stratified by median values of CDA covariates
Removal of 11 154 participants with 25-hydroxyvitamin D concentrations of at least 100 nmol/L deleted large numbers of cancer cases from the fourth quartile of serum 25-hydroxyvitamin vitamin D (any cancer: −66%, major cancer: −66%, breast cancer: −59%, colorectal cancer: −70%, lung cancer: −74%, prostate cancer: −67%, skin cancer: −66%, other cancer: −66%). While this did not change our overall findings, associations with any and major cancer were no longer significant at the Bonferroni threshold, and associations with prostate and other cancer were no longer borderline-significant or significant at the nominal threshold. Only the association with skin cancer remained significant at the Bonferroni threshold, and was in fact strengthened (HR per quartile change 1.33; 95% CI 1.17 to 1.50; p for trend <0.001). Repeating the sensitivity analysis using serum 25-hydroxyvitamin D as a continuous variable yielded identical results.
Discussion
In a community population of patients under investigation for cardiovascular disease, higher serum 25-hydroxyvitamin D was associated with an increased risk of developing skin cancer. This association became stronger as the CDA-level proportion of non-citizens, recent immigrants, visible (non-white) minorities and those not speaking official (English or French) languages at home increased. Associations with prostate and other cancers were weak and may have been due to chance.
Vitamin D (vitamin D2+vitamin D3), which can be synthesised in the skin (vitamin D3) from 7-dehydrocholesterol and ultraviolet (UV) radiation or obtained through diet (vitamin D2 or D3), undergoes two hydroxylations to the biologically active 1,25-dihydroxyvitamin D (D2+D3; calcitriol).23 1,25-Dihydroxyvitamin D binds to vitamin D receptors on target tissues, causing increased update of calcium and phosphate from the small intestine, and increased calcium mobilisation from bone via enhanced osteoclast activity.23 However, 25-hydroxyvitamin D (D2+D3) reflects an individual’s true vitamin D status from both endogenous and exogenous sources because of its long half-life (approximately 2–3 weeks vs 4–6 hours for 1,25-dihydroxyvitamin D), its high concentration (1000 times greater than 1,25-dihydroxyvitamin D) and its resistance to metabolic changes.23
In animal experiments, 1,25 dihydroxyvitamin D has important cellular effects that may decrease the risk of cancer or slow its progression.12 These have been cited as evidence that associations between serum 25-hydroxyvitamin D and cancer risk identified in epidemiological studies represent causal relationships. However, epidemiological studies are susceptible to unmeasured or residual confounding by factors associated with vitamin D deficiency and increased cancer risk (eg, adiposity, low SES). They are also susceptible to reverse causality, particularly because low serum 25-hydroxyvitamin D may in part be a marker of ill health.24 25 This could cause individuals with subclinical cancer or other conditions to become vitamin D deficient. As genetic variants that modestly reduce 25-hydroxyvitamin D are, for the most part, not associated with an increased risk of cancer in Mendelian randomisation studies,26–28 this tends to support this hypothesis. However, in randomised controlled trials, vitamin D supplementation slightly reduces cancer mortality.29 30 For example in the Vitamin D and Omega-3 Trial (VITAL), 2000 IU/day supplementation of vitamin D3 significantly reduced the risk of metastatic or fatal cancer compared with placebo, and this effect was stronger among individuals who had a normal BMI (ie, <25 kg/m2).31 Taken together, while the relationship between vitamin D status and cancer incidence may in part be due to confounding and reverse causality, vitamin D status may be causally related to mortality risk from cancer.
There is a well-established relationship between vitamin D status and sun exposure.32 For example, serum 25-hydroxyvitamin D concentration may rise above 100 nmol/L among individuals who perform extended outdoor activity in the central USA.33 However, this concentration is difficult to achieve without supplementation in locations where daylight hours are shorter (eg, at higher latitude) and sunlight is weaker (eg, at lower elevation).22 Sun exposure is also the most important risk factor for melanoma and non-melanoma skin cancer—particularly among individuals with a light skin tone.34 This is because UV radiation in sunlight induces the synthesis of vitamin D in skin, and damages its DNA without adequate protection by melanin.35 As expected, higher serum 25-hydroxyvitamin D concentration was associated with a higher risk of skin cancer in a recent meta-analyses of prospective cohort studies.36 And while results from Mendelian randomisation studies suggest that this is not a causal relationship,37 38 serum 25-hydroxyvitamin D concentration may still be useful as a skin cancer risk marker because its concentration is related to sun exposure.
In our study, we found a positive association between serum 25-hydroxyvitamin D and risk of skin cancer, which was consistent over time but stronger among individuals who resided in CDAs with a higher proportion of non-citizens, recent immigrants, visible minorities and those who did not speak an official language at home. This may be because individuals living in these communities are less likely to take vitamin D supplements,39 40 which would make their serum 25-hydroxyvitamin D concentration more representative of sun exposure than supplementation—resulting in a stronger overall association with skin cancer risk. Interestingly, removal of individuals with 25-OH vitamin D concentrations of 100 nmol/L or greater strengthened the association with skin cancer—which suggests we may have indeed removed individuals who were more likely to be taking vitamin D supplements. In a study of non-lactating women, daily oral supplementation of 5000 IU/day for 1 month raised serum 25-hydroxyvitamin D above 100 nmol/L.41
This study has some strengths. First, we used available secondary data to assemble a large retrospective cohort of community patients while making several restrictions and exclusions to minimise bias. Second, while this population included only patients who received an ECG, any patients who had a 25-hydroxyvitamin D measurement were eligible for inclusion. During the testing period, our laboratories experienced a very high volume of serum 25-hydroxyvitamin D testing—likely because of substantial interest in vitamin D at the time. Third, we adjusted for several potentially important confounders, including mean daylight hours during month of testing, BMI and community-level measures of SES and examined variation in the association between serum 25-hydroxyvitamin D and cancer risk according to them.
This study also has some limitations. First, as it was based on secondary data, we had a limited number of variables and no control over when they were measured. Importantly, we could not tell if patients had taken vitamin D supplements. Supplementation elevates serum 25-hydroxyvitamin D in individuals who are vitamin D deficient, including those who are deficient because of low sun exposure and who are therefore at low risk for skin cancer. Including these individuals in our study would weaken the strong and biologically plausible relationship we and others have observed between sun exposure, serum 25-hydroxyvitamin D concentration and skin cancer risk. As such, we may have underestimated the true association in our study—especially since we observed variation in this association according to community-level factors related to supplement use, and a strengthening of this association after removing patients with a serum 25-hydroxyvitamin D concentration of 100 nmol/L or greater. We also included only a single measure of serum 25-hydroxyvitamin D for patients in our study. However, even a single measure may be useful in representing usual status due to its moderate intra-individual variation (Spearman’s R, intraclass correlation coefficient=~0.6) over similar time periods as our study.42 Using the first measure may also better represent historic vitamin D status which is more likely to be associated with cancer risk than recent changes from supplementation in response to a diagnosis of deficiency. Interestingly, we found no change in our associations according to elapsed time between 25-hydroxyvitamin D testing and cancer diagnosis—which suggests our single measure may have adequately estimated usual vitamin D status. Second, as our study was observational, we could not determine whether the 25-hydroxyvitamin D-cancer relationship was causal. However, this was not an objective of our study nor was it even achievable. Third, while we did not include participants without a BMI and ECG, we felt obtaining BMI was critical for reducing bias—even if it was based on self-report. We keep only participants who had BMI measured within a short period of time (±3 months) from 25-hydroxyvitamin D measurement to maximise its relevance to 25-hydroxyvitamin D concentration. However, because ECGs are used to identify the presence of cardiovascular disease, our population may be at an elevated risk for both cardiovascular disease and cancer because many of the risk factors for cardiovascular disease are also risk factors for cancer (eg, poor diet).43
Conclusion
Higher vitamin D status was associated with a greater risk of skin cancer in a large community population under investigation for cardiovascular disease. This association is likely due to sun exposure and may be modified by community variation in supplementation rates.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the University of Calgary Conjoint Health Review Ethics Board (Ethics ID 25065). Research in this article was carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki).
References
Footnotes
Twitter @ldekoning
Contributors LdeK, JY and CN designed the study. LdeK acquired the data. JY, YD and LdeK conducted the statistical analysis. LdeK, JY, YD and CN interpreted the data. LdeK and JY drafted the manuscript. JY, YD, CN and LdeK critically revised and approved the final version of the manuscript. LdeK supervised the project, obtained funding and acts as the guarantor.
Funding This work was partially supported by funding from the MSI foundation of Alberta (grant #871) to LdeK, and summer studentship awards to JY from Calgary Laboratory Services and the University of Calgary.
Disclaimer All funding sources had no role in this work.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.