Article Text

Abstract
Introduction Irritable bowel syndrome (IBS) has high rates of psychiatric comorbidity, and impairs health-related quality of life (HRQL). Cognitive–behavioural therapy (CBT) is an effective treatment for IBS, but access to treatment remains low. Our proposed solution is a CBT-based smartphone app, Zemedy.
Methods and analysis This randomised controlled trial of Zemedy (V.2.0) uses an education and relaxation training active control app meant to simulate treatment as usual. A target N of 300 participants complete baseline questionnaires and consent at screening, and are then allocated to either the immediate treatment (Zemedy) or the active control. Treatment lasts 8 weeks, after which both groups complete the same battery used at baseline, and the control group is crossed over to Zemedy. After another 8 weeks, the crossed-over participants will be surveyed once more. Follow-up questionnaires are administered at 3, 6 and 12 months post-treatment. Primary outcomes include gastrointestinal symptom severity and HRQL. Clinically significant change will be defined as post-treatment scores falling within 2 SD of the healthy mean. Analysis will include intent-to-treat between-groups comparisons, controlling for baseline symptom severity, as well as moderation and mediation analyses. We hypothesise that the Zemedy app will outperform the active control app in reducing IBS symptom severity and improving HRQL.
Ethics and dissemination This study was approved by the Institutional Review Board at the University of Pennsylvania. Results will provide essential information on the efficacy and acceptability of an app-based CBT treatment for IBS. The data gathered may help establish the Zemedy app as an empirically supported intervention for IBS and will assist funding bodies in deciding whether to invest in its further development and dissemination. The results will be disseminated to patients with IBS via the media and the company website, to healthcare professionals via professional training (e.g. webinars and grand rounds talks) and to researchers via conferences and publications.
Trial registration number NCT04665271 (https://clinicaltrials.gov/ct2/show/NCT04665271).
- functional bowel disorders
- mental health
- adult psychiatry
- anxiety disorders
- depression & mood disorders
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The study is a randomised controlled trial (RCT) with high ecological validity.
The study design includes an active control condition, which is more robust than the waitlist control used in the RCT for Zemedy V.1.0, and is an important strength, since irritable bowel syndrome has a relatively high placebo response rate.
This study does not control for medication use or other therapeutic interventions patients may pursue.
Inclusion criteria do not include physician confirmation of diagnosis; however, users of self-help apps are not required to provide proof of diagnosis.
Background
Irritable bowel syndrome (IBS) is a chronic disorder of central–enteric (gut–brain) interaction. According to the non-profit Rome Foundation diagnostic criteria,1 it is characterised by recurrent abdominal pain that occurs at least four times per month (or about 1 day per week) over at least 3 months. The pain must be associated with two or more of the following: it must be related to defecation and/or be associated with changes in the frequency and/or form of bowel movements. There are several subtypes, including constipation predominant, diarrhoea predominant, mixed bowel habits and unclassified. IBS that meets strict Rome IV diagnostic criteria is quite prevalent (up to 6%–7% of the population in the USA)1 but self-reported IBS that does not meet strict criteria is highly prevalent (17%–18%) and results in equal disability, health-related quality of life (HRQL) impairment, healthcare utilisation and even greater absence from work.2 Thus, IBS is a serious public health challenge.
Patients with IBS who are actively seeking treatment show extremely high rates of psychiatric comorbidity, with up to 90% meeting criteria for a disorder such as major depression, an anxiety disorder, post-traumatic stress disorder and/or a health anxiety-related disorder such as obsessive compulsive disorder.3 4 IBS also causes significant social and occupational impairment, and can lead to substantial reductions in HRQL.5 Patients with IBS typically develop visceral hypersensitivity, which maintains a cycle of awareness of and hypervigilance towards gastrointestinal (GI) sensations and exacerbates the experience of pain.6 Visceral hypersensitivity is highly correlated with anxiety about GI sensations,7 and the anxiety and hypervigilance about GI sensations in turn exacerbate the hypersensitivity.8
Patients with IBS often exhibit significant anxiety about GI symptoms, and that anxiety is a better predictor of impaired HRQL than symptom severity per se.9 Many patients with IBS start catastrophising about their symptoms, and about the social and occupational implications of their symptoms. Catastrophising is associated with impaired HRQL in and of itself,10 but can also lead to the development of maladaptive coping strategies.5 Maladaptive coping can include significant avoidance that can easily meet criteria for agoraphobia,11 especially in patients who are terrified of the possibility of faecal incontinence. Given the significant conceptual and comorbidity overlap with panic, agoraphobia, social anxiety, illness anxiety, depression and trauma, it is not surprising that IBS responds quite well to cognitive–behavioural therapy (CBT). Indeed, CBT has been shown to be an efficacious treatment for IBS in multiple clinical trials,12 13 and should be considered an empirically supported treatment for IBS. Specifically, CBT reduces GI symptom severity and improves HRQL.14 15 CBT typically includes psychoeducation about the brain–gut axis, relaxation training,16 cognitive therapy to target and reframe GI catastrophising,17 exposure therapy to reduce avoidance of GI sensations, food and situations in which the person fears experiencing GI sensations or being too far away from a convenient, available restroom18 and reducing visceral hypersensitivity.14 Changes in GI-specific cognitions and reductions in GI-specific anxiety have been shown to mediate the impact of CBT on both HRQL and GI symptom severity.19
While CBT is an effective treatment for IBS, it is unfortunately difficult for many patients to get access to it. There are relatively few clinicians trained in GI-specific CBT,5 and the cost of treatment, which typically must be paid for out of pocket, can be prohibitive. This is especially problematic given the economic burdens living with IBS often imposes.20 Thus, in order to disseminate CBT for IBS more broadly, we must develop a less expensive, more accessible mode of treatment delivery. Several low intensity versions of CBT for IBS (eg, with limited or distant therapist involvement such as via email) have been tested17 21 22 and typically obtain robust effect sizes. Patients treated with web-based and telephone-based CBT improve more than those given treatment as usual (eg,23 24). Several treatment manuals and self-help books are available that outline or deliver IBS-specific CBT, and one in particular25 was found to be efficacious as a standalone self-help treatment in a randomised controlled trial (RCT).26
In today’s digitised world, many consumers readily turn to mobile health apps. Mobile apps have multiple advantages, including low cost, accessibility and convenience for the user. The Zemedy app was developed to deliver CBT for IBS directly to users with no direct therapist or clinician interaction required. V.1.0 of the app was tested in an RCT against a waitlist control.27 Primary outcome measures included both GI symptom severity and HRQL. Secondary outcome measures included GI-specific catastrophising, visceral anxiety, fear of food and depression. App users showed both statistically and clinically significant improvement on both primary and secondary outcome measures, yielding a number needed to treat of 2. Gains were generally maintained at 3 months post-treatment. Moreover, the impact of treatment on HRQL was mediated by reductions in catastrophising and visceral anxiety.
Despite these promising results, there were several significant limitations to the app itself and to the study. Uptake of the app was modest, with few users availing themselves of all of the app’s modules. Although users rated the informational content of the app highly, they were less satisfied with the structure and flow of the app and its overall usability. In addition to these concerns, the study design used a waitlist control, which is not a particularly robust control, given the high placebo response rate in IBS.28
The current study is designed to address all of these concerns. V.2.0 of the Zemedy app was modified to be significantly more engaging. It has better flow, fewer modules, and more entertaining animations, videos and patient stories. Our hope is that the user uptake and user ratings will be significantly improved compared with Zemedy V.1.0. Second, this study uses a stronger control group, and will compare Zemedy with a sham app consisting of publicly available educational information (eg, National Health Service (NHS) treatment guidelines for IBS, and information from various online sources such as WebMD and the Mayo Clinic website) and links to a number of different relaxation videos. The purpose of this study is to test the acceptability and efficacy of an updated digital health app (Zemedy V.2.0) that provides CBT-based treatment for IBS. We hypothesise that Zemedy will prove to be more effective in treating IBS symptom severity and improving quality of life for IBS sufferers than the active control app.
Methods
Novel app description
Zemedy V.2.0 is a smartphone application designed by Bold Health (a UK-based company) in collaboration with the first author. The app treats IBS through modules guided by the principles of CBT specifically for IBS, as well as some gut-based hypnotherapy and psychoeducation on IBS. A chatbot guides users through the six modules of the app and the app automatically tracks progress, but users work through the modules at their own pace.
Module 1, called ‘Living with IBS and how CBT can help’, is devoted to psychoeducation about IBS and why CBT is an effective treatment. It includes engaging animations illustrating the connection between the central and enteric nervous system and why stress can exacerbate GI symptoms, as well as animated ‘patients’ who tell their stories of success with CBT. Psychoeducation is crucial to get patients to ‘buy in’ to psychosocial approaches to managing IBS.
Module 2, ‘Activity and IBS’, focuses on exercise and how physical activity can help manage the symptoms of IBS. It includes motivational interviewing (MI) style exercises to help users overcome reluctance to exercise. MI reduces resistance to behaviour change by validating people’s concerns about the challenges of behaviour change (eg, exercise is effortful and uncomfortable), encouraging people to think about their values and goals, and about the costs and benefits of both engaging in a behaviour and not engaging in a behaviour. The module also includes links to instructional videos for specific yoga poses, and more animated patient stories to encourage physical activity and model successful management of IBS with exercise.
Module 3, ‘Managing Thoughts and Worries’, focuses on the basic cognitive model of stress management, including identifying negative automatic thoughts and catastrophic beliefs and using cognitive restructuring to view situations more objectively and realistically. It also applies the cognitive model to specific thoughts and fears about GI symptoms that are common to many patients with IBS. These are basic cognitive therapy skills that are the central component of effective stress management.
Module 4, ‘Managing Avoidance’, focuses on exposure therapy and behavioural experiments to help the user reduce maladaptive avoidance and get back to living their life fully. Patients are encouraged to set up graded exposure exercises for themselves involving any situations (or sensations) that they have been avoiding, including transportation, public venues, and situations involving food and eating. Exposure therapy and reductions in experiential avoidance are crucial components of every effective psychosocial intervention for IBS.
Module 5, ‘Diet & IBS’, focuses on the connection between diet and GI symptoms, but strongly encourages users to reduce their fear of food and start eating a more healthful, balanced and less restrictive diet. Research has shown that fear of food contributes significantly to reductions in HRQL in IBS. The module encourages gradual reintroduction of avoided foods, but no explicit nutritional advice is given.
Module 6, ‘Putting it All Together’, is the final module of the app, which summarises the content of the previous five modules and explains how to use this information in daily life to manage GI sensations and help prevent relapse.
Users are encouraged to apply these strategies to their daily lives even after they have finished going through the app itself. Participants are meant to complete one module per week, leaving the last 2 weeks of the protocol to continue working on the skills they learnt.
In addition to the six modules that serve as the core of the CBT-guided treatment within the Zemedy app, there are also ‘tools’, which are mainly CBT based, but also involve mindfulness, attention training and relaxation exercises that users can use at any time. Some of these tools are unlocked as users progress through the core modules. The ability to unlock new features is a standard approach to ‘gamifying’ apps and is typically expected to enhance engagement. It is possible, however, that users will find this frustrating. We will seek user feedback on this issue at the end of the trial. Additionally, the app includes a ‘flare module’ which users can access at any point during this intervention to address immediate GI discomfort or anxiety.
Education and relaxation training app description
The education and relaxation training app is a rudimentary app meant to act similarly to treatment as usual. This app consists of six modules, of which participants are meant to complete one per week, leaving the last 2 weeks to continue working on the lifestyle changes that some of the modules encourage.
Module 1 includes information from publicly available websites (eg, Mayo Clinic, Cleveland Clinic, UK National Health Service (NHS) and National Institute for Health and Care Excellence (NICE) Guidelines) about the presumed aetiology of IBS and what symptoms are necessary for a diagnosis. It also discusses the various IBS subtypes (IBS-C, IBS-D and IBS-M).
Module 2 contains a list of possible over-the-counter medications and supplements to address IBS symptoms, such as laxatives, anti-diarrhoeals, peppermint oil and probiotics.
Module 3 discusses the impact of lifestyle on IBS. For example, it explains that stress can make IBS worse (without elucidating the underlying mechanisms), and contains links to relaxation training videos for participants to use.
Modules 4 and 5 both discuss diet. Module 4 encourages participants to keep a food diary to see which foods potentially trigger flare-ups in their IBS. Module 5 explains some potential dietary changes that participants can make, such as following the low FODMAP diet and restricting caffeine and alcohol intake. The low FODMAP diet is an evidence-based intervention for IBS and is a common recommendation given to patients with IBS by both nutritionists and gastroenterologists.29 Food diaries and exclusion diets are actually contraindicated in CBT for IBS, because they work via opposing mechanisms. Nevertheless, restrictive diets are empirically supported, are the most common approach recommended by gastroenterologists and are quite efficacious at reducing distressing GI symptoms.30 Module 6 discusses the importance of exercise (again without actually elucidating the underlying biological mechanisms by which exercise can reduce IBS symptoms), and encourages logging exercise, without any attempt to include MI interventions or to help users overcome reluctance to exercise. In sum, the sham app includes standard, treatment-as-usual information and advice that patients with IBS would often be exposed to in other formats, but does not include any of the specific education or treatment strategies that the CBT approach uses and that are central to the Zemedy app.
In sum, the control app contains a good deal of informative text and a number of links to engaging relaxation videos. IBS has a relatively high placebo response rate, and we hope the control app will be both credible and somewhat engaging.
Study design
Because there is considerable overlap between the basic design and materials of this study and the published study of Zemedy V.1.0,27 there is also considerable overlap between the two papers in the description of the basic methods, materials and data analysis plan. Rather than referring readers to the prior paper, some of that text is reproduced here.
This study is a randomised, superiority, non-blinded, crossover trial with an active control group. The study is running from 1 March 2021 to an estimated completion date of 28 May 2023. Participants are recruited from the USA, and study personnel are based at the University of Pennsylvania’s Department of Psychology but because both recruitment, assessment and the treatment itself are all remote, there is no physical location for the study.
Accrual
Participants will be recruited for the trial through IBS-specific social media sites, as well as clinical trial listings at clinicaltrials.gov and iffgd.org (the International Foundation for Gastrointestinal Disorders). Most participants came to the original Zemedy study through Facebook, Twitter and Reddit, so we anticipate that most of our participants for this second study will come from those sites as well. Notices and posts about the study on those sites include a link to a secure Qualtrics survey that contains the consent form and the baseline questionnaires.
Consent
All participants complete informed consent online prior to completing baseline questionnaires. The consent form explains the study, including information about random assignment and the compensation for completing study questionnaires at several follow-up time points. The consent form includes the information that participants will be compensated with $20 in Amazon credit after each round of follow-up questionnaire completion.
Inclusion and exclusion criteria
Inclusion criteria consist of being 18 years of age or older, and participant self-report of having been previously diagnosed by a physician with IBS and/or meeting Rome IV criteria1 by self-report on a standardised questionnaire covering the Rome IV criteria, which will allow for subcategorisation of diarrhoea predominant, constipation predominant, mixed or unspecified IBS. If participants report having been diagnosed with IBS by a physician, but do not currently meet strict Rome IV diagnostic criteria on the questionnaire, they are still allowed in the trial. Many patients with refractory IBS were diagnosed under the old Rome III criteria and the only criterion they fail to meet currently is frequency of abdominal pain. In addition, many patients who fail to meet strict diagnostic criteria still self-report experiencing IBS symptoms that result in equal distress and disability, and even greater work impairment.2 Thus, our inclusion criteria ensure that our sample will reflect the population of interest—people who believe they have IBS, having been told so by a physician and/or who meet strict Rome IV criteria, who are unhappy with their health status and are interested in trying a self-help app. Baseline questionnaire responses are reviewed by the study coordinator to ensure that inclusion criteria are met before participants are enrolled and randomised.
Exclusion criteria consist of having another comorbid GI disorder, such as coeliac disease or an inflammatory bowel disease. Current or lifetime eating disorders were not evaluated or excluded. Many patients with IBS will meet criteria for fear-based Avoidant Restrictive Food Intake Disorder (ARFID), but the CBT protocol actually addresses fear and avoidance of food. Exclusion criteria also include severe depression and/or suicidal ideation—defined as a positive endorsement at the level of 2 or 3 on the suicide item (item 9) of the Beck Depression Inventory (BDI-II). If a potential participant meets exclusion criteria on the basis of severe depression, the first author (a licensed clinical psychologist) contacts them to conduct a risk assessment and offers referral (if appropriate) to local resources. They are also given immediate access to the Zemedy app, if they are interested, but are not enrolled in the trial. Finally, current pregnancy is also an exclusion criterion.
Power analysis
Our goal is to recruit 300 participants. Most internet trials have an attrition rate approaching 50%,31 which would leave us with 150 participants in the study total (75 per group). CBT for IBS typically yields large effect sizes, and the effect sizes of Zemedy V.1.0 on the primary outcome measures of GI symptom severity and HRQL were quite large (d=1.02 and d=1.25, respectively). Assuming a modest effect of the control app of approximately d=0.30, then a final N of 150 will give us 90% power at p<0.05 to detect a difference between groups.
Randomisation
Participants who meet the inclusion criteria will be allocated to one of two conditions using the coin toss feature of random.org. The allocation sequence is concealed to participants until they are enrolled and assigned to the intervention.
Blinding
Because of the nature of the trial (immediate treatment vs active control group), neither participants nor research coordinators are blinded to condition. All outcome data are self-report, thus, blinding of evaluators is neither possible nor necessary. This means that participants are aware of their group allocation upon randomisation.
Intervention and assessments
All potential participants complete the baseline questionnaires as part of the screening process prior to enrolment and randomisation. Upon allocation, those in the immediate treatment group will be given the link to access the Zemedy app and encouraged to download it and begin working through the modules immediately. The active control group will be given access to the education and relaxation training app upon allocation. Both groups work through their respective apps at their own pace during the following 8 weeks. Four weeks after baseline, participants in both groups will be emailed to encourage them to continue using their respective app, and to let them know that they will be receiving the follow-up questionnaires in 4 weeks.
Eight weeks after allocation, all participants will be emailed with a second questionnaire battery which includes all the same measures as at baseline. Participants in the immediate treatment group will also complete the Mobile Application Rating Scale (uMARS) for the purposes of quality improvement and product development. All participants who complete 8-week questionnaires will be compensated $20 in Amazon credit. The compensation is intended to incentivise participants to complete the questionnaires, and has no bearing on their actual use of the app. Upon completion of the follow-up questionnaires, participants in the active control condition will then be crossed over to the Zemedy app.
After having access to the Zemedy app for 8 weeks, participants in the active control group will be emailed a third battery of questionnaires which is identical to the battery received by the treatment group after 8 weeks of app usage—it includes the same measures as the baseline battery and the uMARS. They will be compensated with a further $20 gift credit upon completion of the post-treatment questionnaires.
While we hope that compensation will reduce attrition from the study at follow-up assessments, we still anticipate an attrition rate of at least 50%, which is typical for behavioural health studies using online recruitment and low intensity, distance interventions.(figure 1)

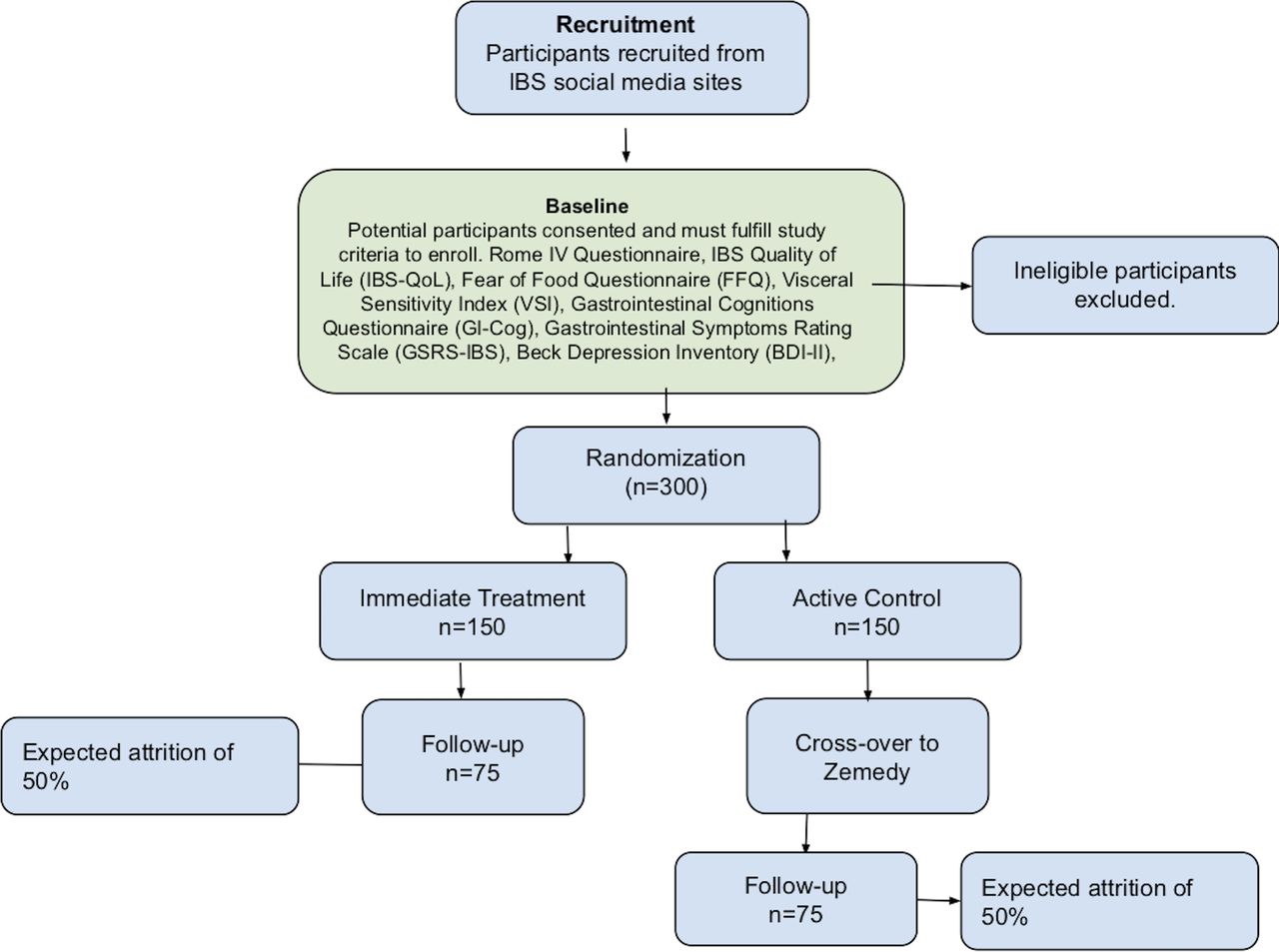{kind=link}
CONSORT diagram. CONSORT, Consolidated Standards of Reporting Trials; IBS, irritable bowel syndrome.
Measures
Baseline screening measure
Modified Rome IV Questionnaire
We used a questionnaire to determine whether participants met current Rome IV diagnostic criteria for IBS. Our questionnaire was based on the Rome IV IBS-specific Questionnaire, which is a validated self-report scale that covers the diagnostic criteria for IBS. It has been found to have acceptable sensitivity and high specificity as well as good test–retest reliability.1 Our measure is shorter (10 items) and uses slightly different numerical scales, but still covers all the primary diagnostic criteria for IBS.
Primary outcome measures
IBS Quality of Life
The IBS Quality of Life (IBS-QOL)32 is a 34-item, self-report measure specific to IBS-related HRQL. It is rated on a 5-point Likert scale ranging from 1 (not at all) to 5 (extremely). It is designed to assess the impact of IBS on quality of life. The IBS-QOL has high internal consistency (Cronbach’s α=0.95), high reproducibility (intraclass correlation coefficient (ICC)=0.86) and good construct validity. Qualitative score ranges are 0–31 (minimal or mild), 32–66 (moderate) and 67–100 (severe impairment). The mean IBS-QOL score for healthy controls is 5 (SD 11), leading to a cut-off point of 27 to fall within 2 SD of the healthy mean.
Gastrointestinal Symptom Rating Scale-IBS
The Gastrointestinal Symptom Rating Scale-IBS (GSRS-IBS) contains 13 self-report items rated on a 6-point Likert scale33 ranging from 0 (no discomfort at all) to 6 (very severe discomfort). Total scores range from 0 to 78. The GSRS-IBS has five subscales, including abdominal pain, bloating, constipation, diarrhoea and satiety. Each dimension has demonstrated high internal consistency of Cronbach’s α ranging from 0.74 (pain) to 0.85 (satiety). Furthermore, the GSRS- IBS has demonstrated both high test–retest reliability, with intraclass correlations among the factors ranging from 0.55 (pain) to 0.70 (bloating), as well as high construct validity.33 The GSRS has been used as a primary outcome measure in a number of recent RCTs of IBS treatments (eg,21) and the Rome Foundation reports that it is shorter and more user-friendly than the IBS Severity Scoring System.34 Qualitative score ranges are 0–20 (minimal or mild), 21–39 (moderate) and 40–78 (severe). The mean GSRS score for healthy controls is 12 (SD 11), leading to a cut-off point of 34 to fall within 2 SD of the healthy mean.
Secondary measures
Fear of Food Questionnaire
The Fear of Food Questionnaire35 is an 18-item, self-report questionnaire that measures fear, avoidance of food, and life interference and loss of pleasure from eating. Items are rated on a Likert scale ranging from 0 (not at all) to 5 (absolutely). It has excellent internal consistency reliability with Cronbach’s α=0.96 and strong 2-week test–retest reliability at r=0.93, p<0.001.35 It also shows good criterion and known-groups validity. Qualitative score ranges are 0–15 (minimal), 16–30 (mild), 31–45 (moderate) and 46–90 (severe).
Visceral Sensitivity Index
The Visceral Sensitivity Index (VSI)8 36 is a unidimensional, 15-item scale that measures GI symptom-specific anxiety. Items are rated on a Likert scale ranging from 0 (strongly disagree) to 5 (strongly agree). It has high internal consistency (α=0.93) and a mean inter-item correlation of 0.47.37 It has good criterion, construct and predictive validity.36 Qualitative score ranges are 0–10 (minimal or mild), 11–30 (moderate) and 31–75 (severe).
Gastrointestinal Cognitions Questionnaire
The Gastrointestinal Cognitions Questionnaire (GI-Cog) consists of 16 self-report items that are rated on a 5-point Likert scale, ranging from 0 (hardly) to 4 (very much). Individual items are summed, and total scores range from 0 to 64. The questionnaire consists of three subscales, the pain/life interference subscale (eg, ‘When I feel my GI symptoms acting up, I’m afraid the pain will be excruciating and intolerable’), the social anxiety subscale (eg, ‘If I have to get up and leave an event, meeting or social gathering to go to the bathroom, people will think there’s something wrong with me’), and the disgust sensitivity subscale (eg, ‘The thought of faecal incontinence is terrifying. If it happened, it would be awful’). The GI-Cog has been shown to have excellent internal consistency (α=0.92) and test–retest reliability (r=0.87, p=0.001).37 Qualitative score ranges are 0–19 (minimal or mild), 20–39 (moderate) and 40–64 (severe).
Beck Depression Inventory
The BDI-II consists of 21 self-report items, each on a 4-point scale ranging from 0 to 3 (0 being not at all, and 3 meaning extreme); therefore, scores can range from 0 to 63. It is scored by adding the severity ratings of each item. A score greater than 20 indicates moderate depression. It has been found to have good internal consistency and test–retest reliability.38 Qualitative score ranges are 0–13 (minimal), 14–20 (mild), 21–30 (moderate) and 31–63 (severe).
Work Productivity and Activity Impairment plus Classroom Impairment Questionnaire: IBS
The Work Productivity and Activity Impairment is a standard measure of the economic, occupational and/or educational impact of a disease or disability.39 It has been adapted for a number of specific conditions, including IBS. Questions cover missed hours of work or school due to IBS, and participant rated impact on productivity (at work or in school) and daily activities. The measure has good construct validity and adequate reproducibility.39
Quality improvement and product development measure
Mobile Application Rating Scale
The uMARS is an end-user version of the Mobile Application Rating Scale which is a 26-item measure including four objective quality subscales (engagement, functionality, aesthetics and information quality), one subjective quality subscale, a six-item perceived impact subscale and a space to provide feedback.40 The uMARS is used to obtain user feedback on the quality of mobile apps during the development and testing process. The uMARS has been shown to have excellent internal consistency (Cronbach’s α=0.90), and high internal consistencies of its subscales (engagement α=0.80; functionality α=0.70; aesthetics α=0.71; information α=0.78 and satisfaction α=0.78).41 Test–retest reliability of the uMARS was found to be good with an average ICC of 0.68.41 It is not a clinical outcome measure, but will be used to inform future product development.
Data analysis
Univariate general linear models in SPSS V.25 will be used to examine between-group effects at post-treatment (8 weeks), controlling for baseline levels of the dependent variable. Paired sample t-tests will be used to examine within-group change over their treatment phase for each group and maintenance of gains from post-treatment to 3-month follow-up, as well as at 6-month and 12-month follow-up. The robustness of these analyses will be examined in an intent-to-treat sensitivity analysis by using multiple imputation. Regression models will then be fitted as in the primary analysis, and pooled estimates of the treatment effect calculated. Three sets of imputed datasets will be created, one for each follow-up data point, baseline measures included in each.
Change in visceral anxiety, catastrophising (as measured by the GI-Cog) and fear of food (calculated as change from baseline to 8 weeks) will be explored as possible mediators of GI symptoms and quality of life at 8 weeks. Regression analysis with estimates of indirect effects will be calculated using a percentile bootstrap estimation approach with 5000 samples implemented with the PROCESS macro V.3.5.42 Both direct and indirect effects will be reported. The direct effect quantifies the estimated difference in the dependent variable (GI symptoms or quality of life) between two cases that are equal on the mediator but differ by one unit on treatment assignment, that is, Zemedy versus the control app group. The indirect effect quantifies how much two cases, one assigned to immediate treatment, the other to waitlist, are estimated to differ on the dependent variables (GI symptoms or quality of life) as a result of treatments’ influence on the mediator, which in turn influences the dependent variable. Two sets of models will be fitted, the first testing the mediator variables separately with simple mediator models, the second fitting a parallel mediator model where the three mediators will be tested simultaneously. The baseline level of the dependent variable will be included as a covariate in all mediation models.
Finally, baseline symptom severity, depression and IBS subtype will be examined as potential moderators of treatment efficacy.
Patient and public involvement
There was no direct patient or public involvement in the design of this research. However, the first author has an active clinical practice in which they work with many patients with IBS, and patient feedback and clinical experience inform the development of Zemedy. There was also patient feedback from the RCT of V.1.0 of Zemedy that guided many of the updates to the app to make it more engaging and user-friendly.
Ethics and dissemination
This study was approved by the Institutional Review Board of the University of Pennsylvania. Participants who endorse suicidal ideation will be contacted by the PI who will offer a risk assessment and referrals to local in-person providers. The active control app recommends certain approaches (such as restrictive diets) that are contraindicated in CBT, but are widely used management strategies for IBS. After the completion of this study, we hope and expect to find that Zemedy outperforms the educational and relaxation app in improving HRQL and GI symptom severity. We also hope to see that Zemedy V.2.0 is rated more highly than V.1.0 in user engagement, functionality, aesthetics and information quality. We plan to submit the resulting paper to a high-impact peer-reviewed journal. De-identified data will be made available in a data repository.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors MH—conceptualisation, methodology, designing intervention, resources, writing (original draft and revisions) and supervision. AD—conceptualisation, methodology, designing control intervention, writing, project administration, software, investigation, participant recruitment and data curation. SI—methodology, designing control intervention, project administration, software, investigation and data curation. BW—designing control intervention and participant recruitment.
Funding This work was supported by Bold Health. Bold Health also designed and provided tech support to the app itself, and provided some data regarding compliance and utilisation of the app.
Competing interests MH serves as a scientific consultant to Bold Health and accepts a modest (less than $5000 per annum) consulting fee. She has no ownership interest in the company.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.