Article Text

Abstract
Introduction The aim of this prospective study is to evaluate the effects of combining topical airway anaesthesia with intravenous induction on haemodynamic variables during the induction period in patients undergoing cardiac surgery.
Methods and analysis This randomised, double-blind, controlled, parallel-group, superiority study from 1 March 2021 to 31 December 2021 will include 96 participants scheduled for cardiac surgery. Participants will be screened into three blocks (ASA II, ASA III, ASA IV) according to the American Society of Anesthesiologists (ASA) grade and then randomly allocated into two groups within the block in a 1:1 ratio. Concealment of allocation will be maintained using opaque, sealed envelopes generated by a nurse according to a computer-generated randomisation schedule. In addition to general intravenous anaesthetics, participants will receive supraglottic and subglottic topical anaesthesia. Changes in arterial blood pressure and heart rate in both groups will be recorded by an independent investigator at the start of anaesthesia induction until the skin incision. If vasopressors are used during this period, the frequency, dosage and types of vasopressors will be recorded. The incidence and severity of participants’ postoperative hoarseness and sore throat will also be assessed.
Ethics and dissemination This study was approved by the Ethics Committee of Qianfoshan Hospital of Shandong Province (registration number: YXLL-KY-2021(003)). The results will be disseminated through a peer-reviewed publication and in conferences or congresses.
Trial registration number NCT04744480.
- anaesthesia in cardiology
- hypertension
- adult anaesthesia
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This randomised controlled trial provides rigorous means to investigate the effectiveness and safety of different induction strategies on haemodynamic stability in patients undergoing cardiac surgery during the induction period and thereafter.
This is an adequately powered and double-blinded study on cardiac surgery that provides much-needed evidence on the clinical effectiveness of the anaesthesia induction strategy.
All experienced anaesthesiologists in the hospital are involved in the study and the procedures for topical anaesthesia or intravenous induction will be performed using a single system; therefore, the results of this study are independent of the operators involved.
The trial will be conducted at a single centre, which may limit the generalisability of findings.
Patients who cannot be evaluated for sore throat and hoarseness due to delayed postoperative extubation may miss follow-up.
Introduction
Anaesthesia induction in patients undergoing cardiac surgery is challenging because the circulatory system is often less tolerant to fluctuations. Patients often experience hypertension and tachycardia, and the incidence of arrhythmia is high. Endotracheal intubation can increase the concentration of catecholamines in the blood by stimulating the sympathetic nervous system, resulting in severe haemodynamic changes.1 2 Conventionally, anaesthesia is induced in cardiac surgery by decreasing the stress response during endotracheal intubation using a large dose of opioids. However, the anaesthetic phase is typically characterised by minimal stimulation immediately after tracheal intubation. Large doses of anaesthetics might be one of the causes of persistent and recurrent hypotension in patients after tracheal intubation. Approximately one-third of intraoperative hypotension occurs between the induction of anaesthesia and the surgical incision.3 4 During this period, persistent and recurrent hypotension increases the difficulty of anaesthesia management; the use of inappropriate vasoactive drugs or differences in patients’ sensitivity to vasoactive drugs cause unstable haemodynamics. Haemodynamic fluctuations may lead to disastrous events. Therefore, the ideal anaesthesia induction strategy for patients undergoing cardiac surgery is not only to provide adequate depth of anaesthesia during endotracheal intubation, but also to stabilise haemodynamics after tracheal intubation.
Topical anaesthesia of the upper airways, including the oropharyngeal and subglottic tracheal mucosa, is crucial to providing adequate comfort to the patient throughout the procedure in awake tracheal intubation.5
Topical anaesthetic is widely used to inhibit intubation.6 Previous studies have shown that topical airway anaesthesia can provide excellent supraglottic and subglottic local anaesthetic effects and can significantly reduce the dosage of intravenous anaesthetics.2 Studies have shown that the combined use of local anaesthetics and low-dose opioids can enhance the effects of local anaesthetics.7 Another study showed that tetracaine is a potent local anaesthetic that prevents high blood pressure and tachycardia and reduces postoperative agitation in the recovery room.8 Application of tetracaine can effectively blunt the cough reflex and provide topical anaesthesia for procedures requiring mucosal anaesthesia, such as bronchoscopy and endotracheal intubation. Traditionally, the standard of care at our institution for topical anaesthesia of the oropharyngeal mucosa involves oropharyngeal 2% lidocaine sprays using a vapouriser while local anaesthesia of the subglottic tracheal mucosa is provided by 1% tetracaine through intratracheal injection.9
To our knowledge, the addition of topical airway anaesthesia to conventional anaesthesia induction for haemodynamic stability in adult patients undergoing cardiac surgery during the induction period has rarely been reported.
Therefore, it is intriguing to explore whether the addition of topical airway anaesthesia to conventional induction techniques could effectively decrease the stress response to endotracheal intubation and avoid hypotension due to vasodilation and circulatory depression during the induction period in patients undergoing cardiac surgery.
Hypothesis and objective
We have hypothesised that, compared with conventional intravenous anaesthesia induction, the addition of topical airway anaesthesia to conventional induction techniques can decrease the stress response during endotracheal intubation and reduce haemodynamic instability from anaesthesia induction to the beginning of surgery. The aim of this study is to explore whether the addition of topical airway anaesthesia to conventional induction techniques will reduce the incidence of hypertension and hypotension during the induction period in patients undergoing cardiac surgery.
Methods and analysis
Study design
This is a randomised, double-blind, prospective, controlled, superiority study, with three blocks, and two-arm, parallel group with 1:1 allocation ratio. This study was approved by the Ethics Committee of Qianfoshan Hospital of Shandong Province (registration number: YXLL-KY-2021(003)).
This study protocol was in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) statement. The SPIRIT checklist is provided in online supplemental table 1.
Supplemental material
Study setting
This study will be performed at the Shandong Provincial Qianfoshan Hospital (The First Affiliated Hospital of Shandong First Medical University), located in Jinan City, Shandong Province.
Patient and public involvement
Patients or the public were not involved in the development and implementation of the research design, recruitment for the study and outcome measures.
Participants
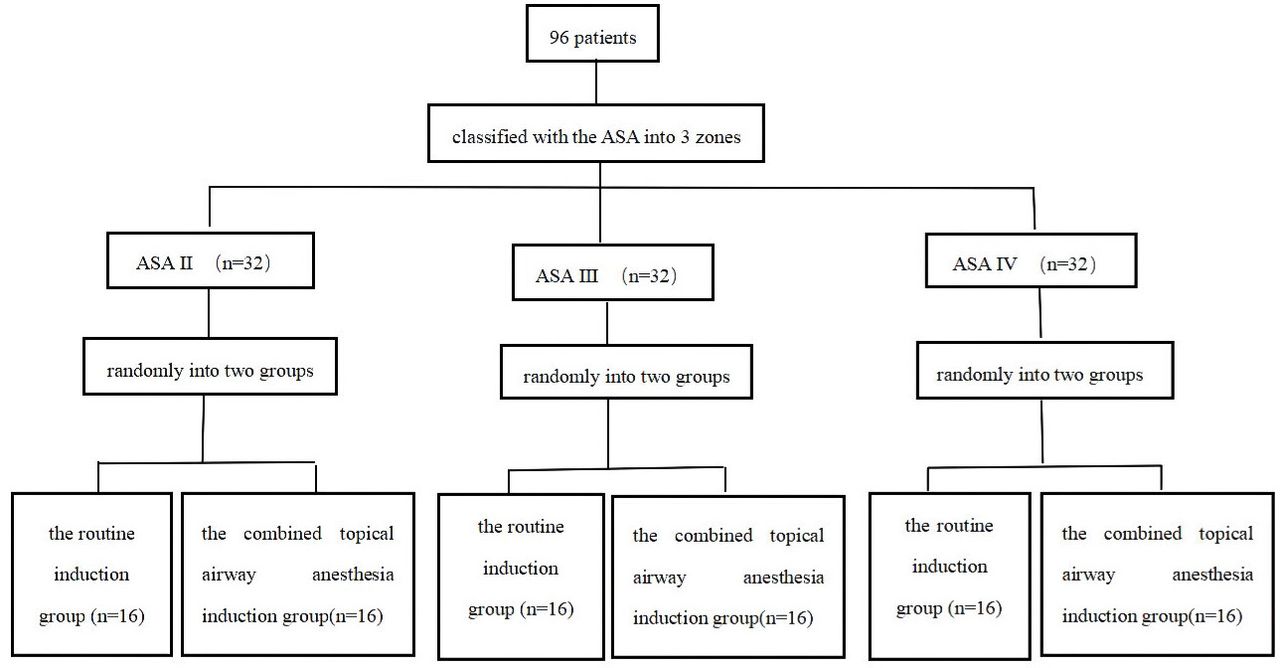
From 1 March 2021 to 31 December 2021, a total of 96 participants aged 18–85 who provide written informed consent and are scheduled to undergo elective cardiac surgery will be screened into three blocks according to the American Society of Anesthesiologists (ASA II–IV) grade and then randomly allocated into two groups, the conventional induction group and the combined topical airway anaesthesia induction group, within the block in a 1:1 ratio. Randomisation is realised using a computer-generated table of random numbers (figure 1).

Consort flowchart of patient recuirement. According to inclusion and exclusion criteria, a total of 96 participants will be screened into three blocks (ASA II, ASA III, ASA IV) according to ASA grade and then randomly allocated into two groups (the conventional induction group and the combined topical airway anaesthesia induction group) within the block in 1:1 ratio. ASA, American Society of Anesthesiologists.
Inclusion criteria
Patients enrolled must meet all of the following criteria: (1) scheduled to undergo elective cardiac surgery; (2) aged 18–85 years; ASA levels Ⅱ–Ⅳ; and (3) provide written informed consent for participation.
Exclusion criteria
Patients will be excluded if they meet one or more of the following criteria: (1) cannot cooperate to complete topical anaesthesia (with mental disorders or unable to communicate); (2) use of a left ventricular assist device prior to surgery; (3) presence of aortic dissection; (4) use of intra-aortic balloon pump prior to surgery; (5) treated with extracorporeal membrane oxygenation prior to surgery; (6) with difficult airway; (7) with hypersensitivity to lidocaine and tetracaine; (8) with atrioventricular block; (9) with haemoglobin less than 80 g/L; (10) with arterial catheterisation other than the radial artery for invasive blood pressure; and (11) participation in other clinical studies in the last 3 months.
Interventions
After admission to the operating room, participants will be continuously monitored using ECG, pulse oxygen saturation, non-invasive blood pressure and the bispectral index (BIS) of electroencephalo-graph (EEG). Radial artery catheterisation will be performed to monitor invasive blood pressure.
According to randomised allocation, experimental medications will be prepared by a nurse who is in charge of random number generation. The experimental medications include sufentanil and local anaesthetics in a vapouriser. The conventional induction group will receive sufentanil (10 μg/mL) in a 10 mL syringe, sham lidocaine and sham tetracaine with normal saline in a vapouriser and a 5 mL syringe individually. The combined topical airway anaesthesia induction group will receive 10 mL normal saline labelled with sufentanil (sham sufentanil), a vapouriser with 2% lidocaine and 1% tetracaine in syringe. Specifically, the local anaesthetics (lidocaine and tetracaine) in the conventional induction group are the sham, while in the topical airway anaesthesia group the sufentanil is the sham. All study drugs will be prepared and labelled by a nurse who is not involved in the perioperative management of the participants.
Supraglottic mucosa anaesthesia will be performed three times using a vapouriser. There will be a 2 min interval between two times of induction of supraglottic mucosa anaesthesia. The range of topical airway anaesthesia will be involved step by step, first in the oropharynx, then in the uvula and palatoglossal arch, and finally the laryngopharynx. Ten sprays will be conducted each time. Induction of anaesthesia will begin after three applications of topical anaesthesia to the superior glottic mucosa using a vapouriser.9 10 Midazolam (0.05 mg/kg), etomidate (0.05–0.3 mg/kg), rocuronium (0.8 mg/kg) and sufentanil 10 μg will be administered for general induction. In the combined topical airway anaesthesia group, 10 µg sufentanil and 10 mL normal saline in a syringe (labelled sufentanil) will be used in the general anaesthesia induction. The staff, unaware of the study design, will decide on the additional dose of sufentanil based on the physical status and haemodynamic changes of the participant. Subglottic anaesthesia will be performed approximately 3–5 min after administration of all intravenous induction drugs (once the participant’s haemodynamic variables are stable). With tracheal topical anaesthesia kit (Tuoren; Henan Province, China), 3 mL 1% tetracaine will be used for subglottic airway anaesthesia. When performing topical anaesthesia, normal saline will be used in the conventional induction group in an equal amount to lidocaine and tetracaine that would be used in the topical airway anaesthesia group and will be labelled as local anaesthetics. During the general anaesthesia induction and the endotracheal intubation period, if the blood pressure or heart rate (HR) increases over 15% from baseline and the BIS exceeds 60, 30 mg propofol, which could be used repeatedly, will be administered as rescue therapy. If the blood pressure or HR decreases over 15% from baseline and the BIS is below 60, 10 mg urapidil or 10 mg esmolol will be given, which could be used repeatedly. If the blood pressure decreases over 15% from baseline, 1 mg dopamine will be administered when the HR is <50 beats per minute and 1 μg norepinephrine will be administered when the HR is >50 beats per minute. Hypertension is defined as an intraoperative systolic blood pressure exceeding 20% from the baseline value or at least one measurement of arterial blood pressure (SAP) >160 mm Hg. Hypotension is defined as 20% of the baseline value or at least one measurement of SAP <90 mm Hg. All participants will be placed in Trendelenburg position (15°–30°) when administering intravenous induction drugs. Targeted continuous infusion of propofol (1 μg/mL) will be initiated and the infusion concentration of propofol adjusted according to the BIS. Tracheal intubation will be performed 3 min after subglottic anaesthesia.
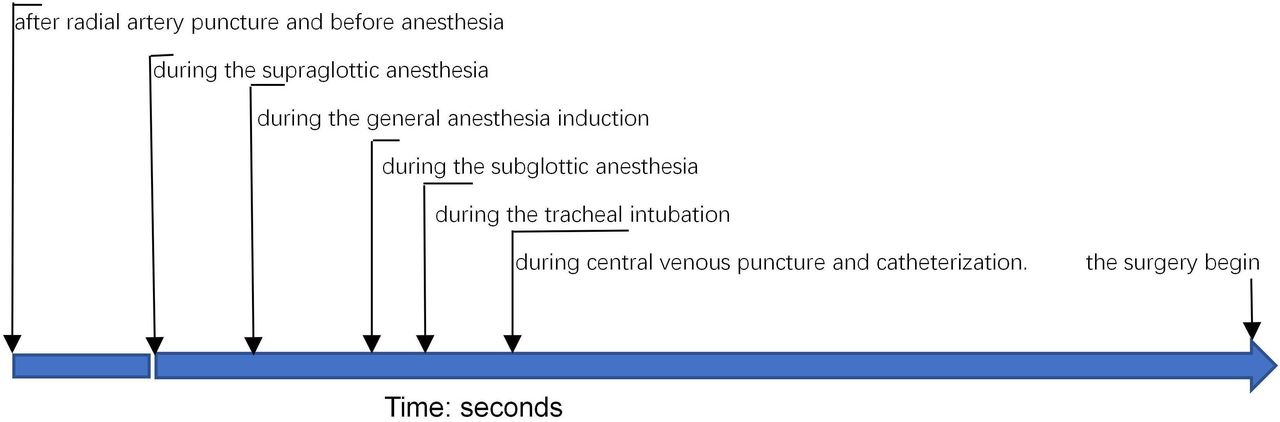
Participants’ haemodynamic parameters, including blood pressure (systolic, diastolic and mean blood pressure) and HR, will be recorded at baseline (T0; intermittent recording three to five times after radial artery cannulation and before anaesthesia), supraglottic anaesthesia (T1; will be recorded three times), general anaesthesia induction (T2; will be recorded once every 5 s), subglottic anaesthesia (T3), tracheal intubation (T4; will be recorded once every 5–30 s) and central venous catheterisation (T5; will be recorded once every 5–30 s). From the beginning of the general anaesthesia induction to the skin incision, the anaesthesiologist decides whether to administer vasopressors according to situation. The type, frequency and dose of vasopressors will be recorded (figure 2 and table 1).
{kind=link}
{kind=link}
Measurement time points. Haemodynamic variables will be recorded after radial artery puncture and before anaesthesia, during the supraglottic anaesthesia, during the general anaesthesia induction, during the subglottic anaesthesia, during the tracheal intubation, during central venous puncture and catheterisation.
Time schedule of enrolment, interventions, assessments and visits for the participants
Cardiac systolic and diastolic functions were evaluated using transthoracic and transoesophageal echocardiography during the intraoperative period. In addition, a haemodynamic monitoring system (Vigileo; Edwards Lifesciences, California) will be used to monitor relevant parameters, including cardiac index (CI), stroke volume variation (SVV), cardiac output (CO) and systemic vascular resistance (SVR).
Outcome measures
Primary outcome measure
The primary outcome is the area under the curve (AUC) below baseline mean arterial pressure (MAP-time integral) from the beginning of the general anaesthesia induction to the beginning of surgery. Numerical integration will be used to calculate the primary endpoint as the area below a horizontal line at the participant’s baseline. Baseline blood pressure is defined as the average of three measurements of invasive blood pressure after the insertion of cannula into the radial artery before general anaesthesia induction. General anaesthesia begins when an induction drug (midazolam) is administered. The beginning of the surgery is defined as the time of the skin incision.
Secondary outcome measures
The secondary outcomes include the following variables: (1) AUC above baseline MAP (MAP-time integral) from the beginning of the general anaesthesia induction to the beginning of the surgery; (2) administration of vasopressors such as norepinephrine and dopamine from the beginning of the general anaesthesia induction to the beginning of the surgery—specifics include time, dosage and type of vasopressor; (3) incidence and type of arrhythmias, such as atrioventricular block, atrial fibrillation and ventricular premature beat; (4) preoperative and intraoperative cardiac systolic function, which is represented by left ventricular ejection fraction (LVEF): LVEF (%)=left ventricular end-diastolic volume/left ventricular end-systolic volume/left ventricular end-diastolic volume × 100%; (5) preoperative and intraoperative cardiac diastolic function, which is represented by E:E′ (the ratio of E wave and E′) and E:A (the ratio of E wave and A wave); (6) intraoperative cardiac output monitoring indicators: CI, SVV, CO and SVR; (7) incidence of postoperative hoarseness at 24 and 48 hours after the surgery—hoarseness is classified as mild, moderate or severe (GRBAS (overall dysphonia grade, roughness, breathiness, asthenia, and strain) score);11 and (8) incidence rate of postoperative sore throat at 24 and 48 hours after the surgery—the severity of sore throat can be evaluated using the Numeric Rating Scale (0=no sore throat, 10=worst sore throat imaginable).12 13
Participant timeline
Potentially eligible participants will be screened according to the inclusion and exclusion criteria before surgery. After written informed consent is obtained, participants will be graded according to ASA classification and assigned to the relevant block, within which they will be randomly allocated to the conventional induction group or the combined topical anaesthesia induction group according to a computer-generated table of random numbers. From the beginning of the general anaesthesia induction to the beginning of the surgery, all relevant variables will be recorded by an independent investigator. Participants will be followed up at 24 and 48 hours after the surgery, prominently on the incidence and severity of postoperative hoarseness and sore throat (table 1).
Sample size calculation
This is a superiority, parallel-group, randomised controlled trial and the ratio of the participants in the two groups is 1:1. A one-sided, two-sample t-test with a sample size of 39 in each group achieves 80% power to detect a ratio of 0.700 when the ratio under the null hypothesis is 1.000. The coefficient of variation in the original scale is 0.6. The significance level (alpha) is set at 0.025. According to references, we identified a coefficient of variation of 60% for the AUC MAP of topical airway anaesthesia as clinically significant.14 We defined a clinically relevant effect as a between-group difference in the AUC (reduction from baseline MAP over 30 min after induction) of ≥33.3%. For this effect size, we estimated that 39 patients per study arm would be needed to demonstrate superiority (a<0.025, one-sided) with 80% power. It is estimated that the potential dropout due to various reasons is 20%, and 48 patients in each group would be calculated, resulting in a total of 96 patients.15
Recruitment
We will recruit patients on the day before surgery. A member of the research team will visit the patient the day before surgery and will explain the research protocol. The patient will be given enough time to read, assess and ask questions before deciding whether to participate or not. The patient will be assured that the quality of perioperative management will not be affected by their refusal to participate. Thereafter, written informed consent will be obtained. Cardiac function of the enrolled patients will be assessed according to the New York Heart Association (NYHA) and EuroSCORE guidelines. Subgroup analysis according to the NYHA and EuroSCORE classification will be performed during data analysis.
Allocation
Sequence generation
Participants will be screened into three blocks (ASA II, ASA III, ASA IV) according to ASA classification and then randomly divided into two groups within the block in a 1:1 ratio. Randomisation is realised by a computer-generated table of random numbers, with random number sequence arranged in ascending or descending order. To reduce the predictability of a random sequence, concealment of allocation will be maintained using opaque, sealed envelopes by the nurse.
Allocation concealment mechanism
Sequentially numbered, opaque, sealed envelopes, locked in the nurse’s office, will be used to ensure concealment until the identification of the participants, for which the nurse would be contacted. Participants will be automatically included in the analysis when numbered envelopes are opened, and the numbers on each envelope would ensure that all participants are enrolled after being randomly assigned. Recruitment records will be established and exclusion of patients will be recorded.
Blinding
Allocation to the groups will be recorded and sealed within envelopes, to which the anaesthesiologists will be blinded. Topical anaesthesia will be performed by an experienced anaesthesiologist, and haemodynamic changes will be recorded by a researcher who is unaware of participants’ allocation. According to the computer-generated table of random numbers, the investigational drugs used in the study will be prepared by a nurse who will not be blinded to randomisation. This ensures that the anaesthesiologist, clinical investigator and data analyst are blinded to the study grouping.
Data collection
Relevant data of participants will be collected by independent researchers. Standardised data collection files will be used to ensure that the data are recorded and used for future statistical analysis. For each patient, at least two investigators (the operator and the research assistant) will collect the data and the research assistant will be responsible for measuring the time using a timer. Demonstrations will be given at the Department of Anaesthesiology to explain the trial and related documentation.
Data management
Patient file number and any additional data allowing patient recognition will be collected in a different and unique Microsoft Excel file. Each patient will be assigned a number that corresponds to a number in the alternative data file. All personal data will be stored on a different locked computer in a secure room at the hospital. The data will be directly transmitted by hand from the research members to the locked computer, never via mail or the internet. Once sensitive data are entered into the computer, any written documents that would allow participants to be identified will be destroyed to avoid data leakage. Only researchers will have access to the computerised data.
Statistical methods
All statistical data analyses will be performed using the SPSS software (IBM SPSS Statistics V.25). We will conduct an intention-to-treat and per-protocol analyses for the primary outcome. Data will be expressed as mean with SD or median with IQR for continuous variables, depending on normality determined using the Shapiro-Wilk test. Categorical variables are to be described as counts (percentages). Normally distributed and continuous variables will be compared using Student’s t-test and non-normally distributed variables using the Mann-Whitney U test. Categorical variables will be described as counts (percentages) and compared using χ2 analysis or Fisher’s exact test. Analysis of variance of measurements will be performed. The primary outcome will be compared between the groups using a general linear model. The overall significance level is set at p<0.05 and Bonferroni correction will be used to control type I errors.
Handling of lost to follow-up
We will make every effort to limit loss to follow-up within 5%, such as excluding patients who may be unwilling to participate in the follow-up before randomisation, completing each follow-up as fast as possible and streamlining the experimental procedure during follow-up. If the rate of loss to follow-up exceeds 5%, multiple imputations will be performed to deal with incomplete data.
Discussion
This is a prospective, single-centre, randomised, parallel-group, double-blind, superiority, controlled trial aimed to assess the efficacy and safety of topical anaesthesia for haemodynamic stability during induction in patients undergoing cardiac surgery. This study aimed to test the hypothesis that topical anaesthesia combined with intravenous anaesthesia can reduce haemodynamic fluctuations in patients undergoing cardiac surgery, from anaesthesia induction to the beginning of the surgery.
In clinical practice, routine anaesthesia induction strategy for cardiac surgery, especially for patients with severe coexisting disorders, largely relies on high doses of opioids to decrease the stress response to endotracheal intubation. However, high doses of opioids often lead to persistent and recurrent hypotension from anaesthesia induction to the beginning of surgery. Our study might provide a better induction strategy for patients undergoing cardiac surgery which could improve haemodynamic stability during induction period.
Advantages of the current study include a unique ASA-stratified and strict randomised system, clear inclusion and exclusion criteria, a rigorously uniform protocol for topical anaesthesia and intravenous induction, and a dedicated anaesthesiologist for conducting each procedure. The findings of this study could serve as a reference for future multicentre trials to verify the effects of topical anaesthesia combined with intravenous induction on haemodynamics.
Data monitoring
Given that a recent feasibility study did not find any significant complications with the topical anaesthetic approach and due to the relatively small number of patients in each group, we will not have a formal data monitoring committee.
All data will be kept confidential. Original data will be recorded using case report forms, and completed case report forms will be checked by a study coordinator who will be qualified by the principal investigator.
Limitation
Unfortunately, it would be difficult to eliminate bias with the current research set-up in the hospital. Selection bias will be present as a consecutive series of patients will not be approached due to sufficient personal resources during on-call hours; the recruitment depends on the time availability of the anaesthesiologist.
Safety assessments
Safety assessments will include monitoring and recording of all adverse effects and severe adverse effects and regular monitoring of intraoperative critical data by the attending anaesthesiologists. Before signing the informed consent, patients will be informed of all potential harms as a standard before anaesthesia, including the risks of topical anaesthesia such as anaphylaxis and severe skin and mucosal damage. Any adverse effects or possible complications will be compiled in the data collection form. However, lidocaine and tetracaine used for topical anaesthesia in this study do not pose additional risks because they are within the safe dose range of conventional anaesthetics drugs. Due to the low dosage of general anaesthetics, compared with the combination of topical anaesthesia with intravenous anaesthesia, they cannot confer adequate depth of anaesthesia to inhibit the response to tracheal intubation.
If significant risks to patient safety occur during the trial, we will report it to the research group and the ethics committee to evaluate whether the trial should be continued. Appropriate actions, including medical attention, will be taken if and when necessary.
Trial status
At the time of manuscript submission, the recruitment of the patients has started and is ongoing.
Ethics statements
Patient consent for publication
Acknowledgments
The authors appreciate the work of Hai-xia Zhang on data collection for this study. The authors also acknowledge Professor Fang Tang and her team for assistance in statistical analysis. The authors also thank all the participating patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
TTC and ML contributed equally.
Contributors Study design: ML. Screening, enrolling participants, data collection, follow-up and writing of the report: TTC. Management and literature search: YLW and CPG. Statistical analysis: JHW. Sequence allocation and experimental medications allocation: CSW.
Funding This work was supported by the Natural Science Foundation of Shandong Province (grant number: ZR2016HL02).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.