Article Text

Abstract
Objectives This study aimed to examine the prevalence of peritraumatic stress symptoms (PTSSs), perceived threat, social support and factors contributing to clinically significant PTSS among frontline COVID-19 healthcare workers (HCWs) in China.
Design and setting An online survey through self-administered questionnaires was conducted from 18 February to 4 March 2020, during the outbreak of COVID-19.
Outcomes measures PTSS was assessed using the post-traumatic stress disorder (PTSD) self-rating scale. Demographic and socioeconomic characteristics, self-reported health, physical/psychological symptoms, perceived threat from frontline work and perceived social support were investigated. Multivariable line regression analysis distinguished factors associated with HCWs’ PTSS scores.
Results A total of 676 (58.1%) HCWs have shown clinically significant high levels of PTSS. Only 441 (37.9%) self-reported good health. Most had physical symptom(s) (915 (78.7%)), psychological symptom(s) (906 (77.9%)), inability to vent emotions (284 (24.4%)), emotional exhaustion (666 (57.3%)) and 1037 (89.2%) needed professional respect. Moreover, social support received was less than expected, and the receipt of psychological services/help scored the lowest (3.11±1.73). Combined psychological and physical symptoms, difficulty in releasing tension and venting emotions timely, fear of infection, emotional exhaustion and depersonalisation are significantly associated with PTSS scores among frontline HCWs. Working ≥8 hours, having the senior professional title, self-reported health, enjoying perfect protection and control measures, economic subsidy and control policy on reducing discriminatory practices are negatively correlated with PTSS scores.
Conclusions During the outbreak of COVID-19, frontline HCWs experienced clinically significant high levels of PTSS and heavy workload, and the emergency resulted in their inadequate psychosocial support. If this is left unchecked, HCWs have a higher risk of developing PTSD. Early detection, identification and person-directed, targeted multidisciplinary interventions should be undertaken to address various influencing factors. Comprehensive measures, including setting up emotional release channels, as well as providing psychological and social support intervention for HCWs globally, are highly recommended.
- COVID-19
- health & safety
- public health
- depression & mood disorders
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Multivariate linear regression was conducted to analyse factors associated with peritraumatic stress symptom (PTSS) scores of frontline healthcare workers (HCWs).
Physical/psychological symptoms, perceived threats of frontline work and achieved/anticipated social support were investigated online during 18 February to 4 March 2020, the hot phase of the COVID-19 outbreak in China.
This was the first study to explore the gap between achieved and anticipated social support of frontline HCWs during the early stage of the COVID-19 outbreak.
Potential limitations include: the cross-sectional design, which resulted in a limit on causal inference; non-validated questions, which made extrapolation difficult; online self-reporting instruments, which caused the inherent recall bias; and the time of assessment, instruments and methods, which may have contributed to this overestimation of the prevalence of post-traumatic stress disorder.
Longitude studies monitoring PTSS rates and effective intervention are needed.
Introduction
In December 2019,1 a novel coronavirus named SARS-CoV-2, which is responsible for causing COVID-19,2 3 was detected in Wuhan, China.4 The National Health Commission (NHC) of China and the WHO reported that the confirmed cases in mainland China had increased to 72 436 on 17 February 2020, including 1868 deaths.5 Subsequently, the pandemic escalated domestically and internationally with a frightening transmission speed.6 7 The WHO declared a Public Health Emergency of International Concern and a pandemic on 30 January 20208 and 11 March 2020,9 respectively. Facing the multiple sources of unpredictable and uncontrollable stress of healthcare systems (eg, management of critical medical situations, frequent witnessing of death, insufficient or inadequate personal protective equipment) at the peak of the COVID-19 pandemic, frontline healthcare workers (HCWs) were exposed to a high risk of infection because of close, frequent contact with infected patients,10 with the infection rate of HCWs (2.10%) being dramatically higher than that of non-HCWs (0.43%).11 Human-to-human transmission,7 12 high morbidity, potential fatality13 and no vaccine for COVID-1914 may have magnified the HCWs’ hazard perception of COVID-19 and experiences of severe psychological distress, including COVID-19-related acute stress responses.15 16
Post-traumatic stress disorder (PTSD) is a stress-related mental disorder that develops after experiencing or witnessing life-threatening traumatic events.17 18 It places a s ubstantial burden not only on individuals, affecting their relationships and jobs,19 but also on the society.20 Due to cautious considerations on the clinical diagnosis of PTSD, individuals who meet the cut-off point with high scores are considered to have clinically significant peritraumatic stress symptoms (PTSSs).21 PTSS rates range from 10% to about 20%22 in HCWs working in emergency care settings, with even higher rates (8%–30%) among intensive care unit staff.23 24 Moreover, HCWs, especially those working on the frontline, have reported negative consequences since the outbreak of the COVID-19 pandemic.25–27 It is worth considering that during a pandemic, HCWs are exposed to physical and psychological stressors that may result in severe mental health outcomes.22 Lu et al28 indicated that more than 33.3% of HCWs caring for infected patients had developed significant stress symptoms during previous pandemics. The worldwide spread of COVID-19 has challenged the capacity and effective response of healthcare systems.29 Given the crucial role in responding to a pandemic, policymakers need empirical evidence to address the substantial issue of psychological distress and mental health of HCWs.30 It is, therefore, critical that concerns about mental health and systematic psychological adjustment of frontline HCWs’ response to the COVID-19 outbreak should be highlighted.22 31 32
Although most individuals prove resilient after exposure to a traumatic event,33 several risk factors may compromise adaptation effectiveness. Identifying risk factors affecting frontline HCWs with high levels of PTSS is crucial to high-risk groups and to establish specific intervention programmes. Previous research has demonstrated that HCWs experience a high degree of mental disorders,4 34 and that social support is a buffer factor between trauma and PTSS development.22
Burnout, which can be described as emotional, physical, psychological and spiritual exhaustion, can impact workers’ sense of accomplishment.35 36 Steudte-Schmiedgen et al confirmed that feeling physically or mentally exhausted is associated with a higher prevalence of PTSSs.37 Chirico et al also confirmed that burnout resulted from emotional exhaustion (8.0%) and depersonalisation (35.9%).38 Consequences of burnout are poor quality of care, professional mistakes, reduced attention to individual protection procedures and increased risk of contagion in the workplace.38–40 Thus, it is necessary to analyse the relationship between high levels of PTSS and burnout in HCWs.
Consistently, evidence indicates that support (eg, from family, friends and supervisors/colleagues) is an important resilience factor against the development of PTSS.41 42 Besides, in particular, clinical settings (eg, isolation), it often leads to subsequent decreased social support.22 Furthermore, in the context of disaster medicine with the lack of human and technical resources, HCWs could also develop acute stress disorders, potentially degenerating into chronic PTSD43; supportive resources buffer the relationship between occupational demands and psychological distress and are worthy of critical attention.44 Though organisational social support has been emphasised to fill the gap of social support (received vs. anticipated) during an outbreak,45 to the best of our knowledge, there are no studies that assess the gap between the social support anticipated and the actual support by the HCWs.
Delayed-onset PTSS reflects the worsening of symptoms over time due to stressors that occur after the traumatic event.46 A review inferred that evidence of quantitative and qualitative interventions to improve the mental health of frontline HCWs during or after disease epidemics and pandemics was lacking.47 Horesh and Brown48 and Søvold et al49 called for valuable data collection to inform high-quality practice and policy as soon as possible. Greene et al pointed out that it was important to examine mental distress and identify risk factors among HCWs at different pandemic phases.50 Furthermore, risk and protective factors, such as physical symptoms,51 of frontline HCWs with high levels of PTSS during pandemics are still understudied.29 52 Moreover, the prevalence of peritraumatic distress, perceived threat from frontline work and perceived social support among frontline HCWs exposed to the outbreak in China were not fully reported. Consequently, we hypothesised that demographic and socioeconomic characteristics, self-reported health, physical or psychological symptoms, perceived threat from frontline work and perceived social support contributed to the occurrence of high levels of PTSS. This study aims to assess Chinese frontline HCWs’ mental health to develop possible intervention strategies, with the goal of reducing HCWs’ psychiatric burden in China and worldwide in future outbreaks of infectious diseases.
Methods
Study design and sample size
This was a cross-sectional study performed via an online survey, which was run from 18 February53 (72 436 cases) to 4 March54 (80 552 cases), 2020. The study commenced 8 weeks after the COVID-19 epidemic outbreak in Wuhan.7 The sampling period corresponded to the period that witnessed the highest surge of COVID-19 cases in China,55 that is, the highest vulnerability period after the great distress with 2055 laboratory-confirmed that over 3000 medical health workers in (Wuhan) Hubei province,56 across 476 hospitals.56 57
An online survey of 1389 HCWs in the epicentre of Hubei province and other hospitals around China was conducted between 18 February and 4 March 2020. (1) PTSS, (2) demographic and socioeconomic characteristics, (3) peritraumatic distress, including self-reported health, four physical symptoms and 11 psychology symptoms, (4) perceived threat from frontline work and (5) perceived social support were investigated through a self-designated questionnaire.
The sample was obtained by recruiting HCWs working in hospitals (the eligibility criteria). An electronic version of the questionnaire was sent to all HCWs willing to participate in this survey. A quality control officer checked each returned questionnaire and deleted poor-quality responses. Of the initial 1391 HCW responses, 1389 questionnaires were included in the data analysis after removing invalid respondents.
Data analysis
The sample size was estimated on the needs of logistic regression analysis; hence, it was 10 times greater than the number of independent variables. The results of this study were generated through descriptive statistics and multivariate regression analysis. Descriptive statistical processes were applied to demographic and socioeconomic characteristics and social–psychological variables. Categorical variables were expressed by frequency and percentage (absolute values), and continuous variables were expressed as mean±SD. The normal distributions of the continuous variables were verified using P–P plots and K–S tests. Model fits were evaluated using the Durbin-Watson test. We calculated the total scores (mean±SD) of PTSS and determined the percentage of clinically significant PTSS according to the PTSS guidelines. Differences between the two categories of variables were compared by the independent single-sample t-test, and differences between three or more categories were analysed by χ2 test. Bivariate correlation analysis between continuous variables and PTSS scores. Statistics, including F values, R2 changes (ΔR2), standardised regression coefficients (β) and p values, in the regression model, were reported. To avoid omitting the important variables, less stringent selection criteria of univariate analysis were adopted. Those variables with p≤0.40 were entered into the multivariate linear models for further exploration, with PTSS scores serving as dependent variables. The internal consistency of the items was checked by the Cronbach’s alpha. The composite reliability (CR) and the explained average variance extracted (AVE) values were considered for convergent validity.58 All the statistical significance of all two-tailed tests was set at p<0.05, and SPSS V.19 software was used for the statistical analysis.
Dependent variable
Peritraumatic stress symptoms
The PTSD self-rating scale (PTSD-SS) is a self-report measure developed by Chinese experts Liu et al59 that captures the level of symptomatic responses to a specific traumatic stressor, related to the consequent development of PTSD symptoms. The PTSD-SS matched well with the specific conditions of Chinese culture and lifestyle, and was proved to be a valid screening method to identify patients experiencing trauma in China.60
Theoretically, PTSD-SS can be divided into subjective assessments of traumatic events (item 1), repeated experiences (items 2, 3, 4, 5, 17, 18, 19), avoidance symptoms (items 6, 8, 9, 10, 16, 21, 22), increased alertness (items 7, 11, 12, 13, 15, 20, 23) and impaired social functioning (items 14, 24). Based on the statement of the Diagnostic and Statistical Manual of Mental Disorders FourthEdition,61 regarding characteristics of PTSD and the PTSD response index scale,62 the diagnostic criteria of PTSD in International Classification of Diseases 11th Revision,63 and the diagnostic criteria of delayed stress disorder in The Chinese Classification of Mental Disorders, Second Edition, Revised,64 the PTSD-SS contains 24 items. These were developed to measure a set of characteristic symptoms (lasting for at least 1 month) that occurred after stress incidents, including persistent repetition of traumatic experiences, avoidance of events or situations related to traumatic events or general reaction numbness and heightened vigilance. Each item reflects the influence of traumatic events on physiology, psychology and life.65 66
The scale has been shown to have high internal consistency, with a Cronbach’s alpha within 0.921–0.965,59 67–69 good test−retest reliability and validity. Li et al70 showed that the internal consistency coefficient, the split-half reliability coefficient and the retest reliability coefficient of PTSD-SS were 0.9106, 0.9217 and 0.8547, respectively. Huang et al reported that the content validity of PTSD-SS was 0.902, and the Cronbach’s alpha was 0.939.71 Liu et al reported that the re-test correlation was 0.39 (p<0.01) and the Cronbach’s alpha was within 0.745–0.878.72 The pre-test conducted on 20 emergency department nurses and trauma patients had a Cronbach’s alpha of 0.8065 and 0.66–0.88,73 respectively. Therefore, PTSD-SS has good empirical validity and can be used as an assessment tool for PTSS scores.74
The scale contains 24 items and 3 subscales, namely, subjective assessment of intrusion, avoidance and hyperarousal. The degree of distress for each item is rated on a 5-point scale (1=the absence of a symptom to 5=maximal symptoms). For symptoms of intrusion, avoidance and hyperarousal, scores of each subscale were calculated, and an average score above 2 was used as the cut-off value. A cut-off score of 50 on the PTSD-SS total score indicated a clinically significant high level of PTSS. The higher the score, the more severe the PTSS reaction. In this study, the Cronbach’s alpha of the total scale and subscales were 0.974, 0.951, 0.941 and 0.892, respectively. The AVE and CR of the subscales were within 0.887–0.944 and 0.566–0.663, respectively. In this study, ‘COVID-19 pandemic’ and ‘during the emergency’ were respectively used for the subjects as a reference of a traumatic event and a specific time frame.
Independent variable
Independent variables included in the modelling were demographic and socioeconomic characteristics, peritraumatic distress, perceived threat from frontline work and perceived social support. Demographic and socioeconomic characteristics included age group (1=20–30 years, 2=30–40 years, 3= >40 years), gender (1=male, 2=female), profession (1=nurse, 2=physician, 3=medical technician, 4=administrator), professional title (1=without professional title, 2=primary, 3=intermediate, 4=senior) and working in a designated medical institution for COVID-19 treatment (0=no, 1=yes).
Perceived peritraumatic distress
The symptoms experienced for more than a month included physical and psychological symptoms.75 Physical symptoms comprised76: (1) palpitations, (2) discomfort or feeling of pressure in the chest, (3) headaches and (4) poor concentration. The Cronbach’s alpha of the 4-item physical symptoms was 0.909, and the AVE=0.685, CR=0.896. Psychological symptoms included77: (1) fear, (2) horror, (3) depression, (4) suspicion, (5) suppression, (6) helplessness, (7) no confidence, (8) irritability, (9) guilt, (10) solitariness and (11) frustration. Participants were asked to report if they had experienced these feelings during COVID-19 frontline work (eg, ‘Having palpitations and worrying about heart trouble’). The Cronbach’s alpha of the 11-item psychological symptoms was 0.973, and the AVE=0.745, CR=0.970. More than one physical/psychological symptom of peritraumatic reaction could be endorsed. Each reported physical/psychological symptom was rated on a 5-point Likert scale from 1 to 5 (5=strongly agree to 1=strongly disagree) and recoded into two categories: ‘0=no’ or ‘1=yes’ (rated score from 1 to 5) for the purpose of logistic regression modelling. The number of physical symptoms (maximum 4) and psychological symptoms (maximum 11) were added up to obtain the total score.
The Maslach Burnout Inventory (MBI) consisted of three subscales: emotional exhaustion (items 1, 2, 3, 6, 8, 13, 14, 16, 20), depersonalisation (items 5, 10, 11, 15, 22) and personal accomplishment (items 4, 7, 9, 12, 17, 18, 19, 21). In this study, the Cronbach’s alpha for each of the three dimensions was 0.936, 0.859, 0.877, respectively; the total scale had good internal consistency (Cronbach’s alpha=0.900).
A key question measured self-reported health, ‘Please choose one point on this 0–100 scale, which can best represent your health today; 0 means the worst and 100 means the best.’ The responses were organised into two categories; ‘0=less than 80’ and ‘1=more than 80.’ Additionally, sleep hours and working hours per day were reported by participants and classified into two categories: sleep hours per day (1=less than 6 hours, 2=more than 6 hours) and working hours per day (1=less than 8 hours, 2=more than 8 hours).
Perceived threat of frontline work
Participants also reported perceived threat from frontline work measured by self-designated questions78: ‘colleagues or relatives infected with COVID-19’ (0=no and 1=yes). Further, ‘nowhere to release tension’, ‘the inability to vent emotions’, ‘guilt towards the family’, ‘the need for professional respect’, ‘feeling physically and mentally exhausted’, all of them reported ranging from 1 (none) to 5 (very much).
Perceived social support
Future research should continue to understand the psychological well-being of HCWs who deal with infectious disease outbreaks and the effectiveness of intervention programmes.79 80 On 26 January 2020, the NHC published the ‘Guiding Principles for the Emergency Psychological Crisis of the Novel Coronavirus Infection’.81 On 10 February 2020, ‘Notice on Several Measures for Improving the Working Conditions of Frontline Medical Staff and Taking Care of the Physical and Mental Health of Medical Staff’ was also issued, which proposed more specific supports to improve the mental health of HCWs fighting with the COVID-19 outbreak.82
Therefore, participants were asked to rate the social support received and the social support demanded/anticipated to cope with COVID-1983–87 using a 6-point scale where 0=not at all, 1=very little, 2=little, 3=neutral, 4=much and 5=very much. We measured the supply of prevention and control materials, perfect protection and control measures, protection of rights and interests in pandemic prevention, support of providing more medical personnel to ease the existing overburdened staff, economic subsidy, support of providing a place to rest, support of providing psychological services and help, policy on discriminatory practices and security for the family. The Cronbach’s alpha of actual received social support (CR=0.919, AVE=0.558, factor loading range within 0.689–0.804) and demanded/anticipated social support (CR=0.912, AVE=0.537, factor loading range within 0.603–0.784) were 0.900, 0.891, respectively. The difference in each type of social support related to COVID-19 frontline work between the actually received and demanded/anticipated was calculated and sorted into three categories: 1=the actual support gained is less than the demanded/anticipated, 2=the actual support achieved is equal to the demanded/anticipated and 3=the actual support is greater than the demanded/anticipated.
Patient and public involvement statement
There was no patient or public involvement in the production of this study.
Results
Bivariate analyses
Demographic/socioeconomic characteristics
An analysis of statistics revealed that 1163 (83.7%) participants reported working in frontline positions during the COVID-19 pandemic (online supplemental etable 1). Participants’ characteristics are listed in table 1 and online supplemental etable 2. Of the total number of participants (1163), 676 (58.1%) experienced clinically significant PTSS. The majority of the respondents (72.3%) were women, and the median age was 35.75±8.52. Most (43.5%) of the participants were aged 31–40 years. Nurses comprised 55.2% of the study population, followed by physicians (27.0%) and medical technicians (10.7%). Among the respondents, without professional title, primary, intermediate and senior titles accounted for 4.8%, 47.8%, 30.2% and 17.2%, respectively. Of the participants, 56.5% reported sleeping less than 6 hours per day, 27.8% reported work more than 8 hours per day, 226 (19.4%) reported that their colleagues or relatives were infected with COVID-19 and 854 (73.4%) reported working in designated medical institutions for COVID-19 treatment. The mean score of PTSS was 57.17±21.49. The subscale of PTSS scores was 32.60±11.71, 15.65±6.88 and 8.93±3.92 for intrusion, avoidance and hyperarousal, respectively. Meanwhile, PTSS scores were significantly different in the frontline HCWs groups (eg, age, professional title, working in designated medical institutions for COVID-19 treatment, colleagues or relatives infected with COVID-19, sleep hours per day and so on). Frontline HCWs who reported sleeping less than 6 hours (p=0.002), colleagues or relatives infected with COVID-19 (p<0.001) and working in designated medical institutions for COVID-19 treatment (p<0.001) showed higher PTSS scores than those who had not.
Supplemental material
Comparison of PTSS scores among different demographic/socioeconomic characteristics in frontline HCWs fighting against COVID-19 (n=1163)
Furthermore, 78.7% of the frontline HCWs reported at least one physical symptom, 786 (67.6%) having palpitations, 741 (63.7%) having discomfort or feeling pressure in the chest, 754 (64.8%) having headaches or pressure and 753 (64.7%) having poor concentration (online supplemental efigures 1and 2).
Supplemental material
Supplemental material
Peritraumatic distress: self-reported health, physical/psychological symptoms and burnout
Moreover, the average number of physical symptoms and psychological symptoms was 2.61±1.65 and 6.29±4.63, respectively (table 2). The average score of self-reported health was 73.42±19.59, and 37.9% of the frontline HCWs self-reported good health. The self-reported health (r=−0.399, p<0.001), emotional exhaustion (r=0.663, p<0.001), depersonalisation (r=0.575, p<0.001), number of physical symptoms (r=0.609, p<0.001) and number of psychological symptoms (r=0.697, p<0.001) were significantly associated with PTSS scores.
Results of univariate ANOVAs and t-tests showing mean differences on PTSS scores based on personal factors
Furthermore, 234 (20.1%) reported nowhere to release tension, 284 (24.4%) reported inability to vent emotions, 665 (57.2%) reported feeling guilty towards the family for being unable to take care of family members due to work, 1037 (89.2%) reported the need for professional respect and 417 (35.9%) reported physical and mental exhaustion, while 57.3% reported emotional exhaustion measured by the MBI scales (online supplemental etable 3). Meanwhile, participants reported 6.29±4.63 psychological symptoms and 2.61±1.65 physical symptoms.
Perceived threat from frontline work and perceived demanded social support
Table 3 presents perceived threat from working at the frontline and perceived social support related to frontline HCWs. The correlation analysis results showed that nowhere to release tension (r=0.540, p<0.001), disability to vent emotions (r=0.517, p<0.001), feeling guilt towards the family (r=0.243, p<0.001), the need for professional respect (r=−0.084, p=0.004) and fear of infected (r=0.377, p<0.001) were significantly associated with PTSS scores.
Bivariate associations between perceived threat from frontline work and perceived demanded/anticipated social support with PTSS scores
Moreover, ‘supply of prevention and control materials (r=0.094, p=0.001)’, ‘protection of rights and interests in pandemic prevention (r=0.079, p=0.007)’, ‘more medical personnel to ease the existing overburdened staff (r=0.106, p<0.001)’, ‘economic subsidy (r=0.060, p=0.041)’, ‘support of providing a place to rest (r=0.112, p<0.001)’, ‘support of providing psychological services and help (r=0.270, p<0.001)’ and ‘security for the family (r=0.082, p=005)’ were significantly associated with PTSS scores.
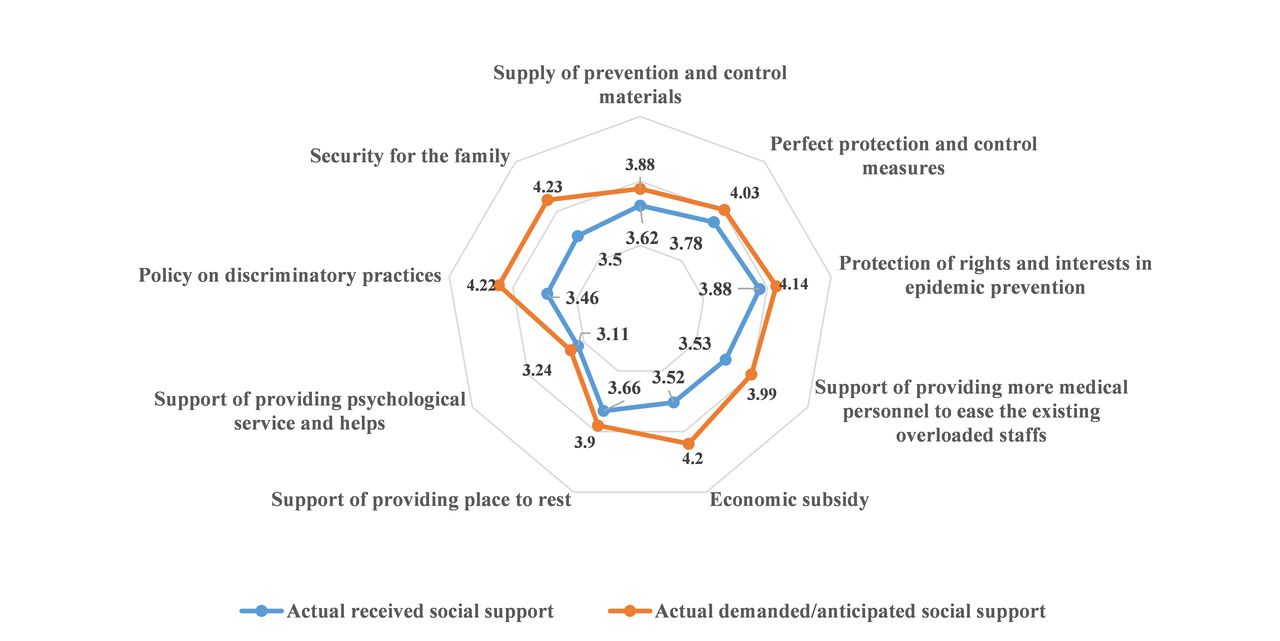
The actual perceived supply of all social support related to COVID-19 frontline HCWs is lower than its actual demanded/anticipated (figure 1). Support of providing psychological service and help was reported as the lowest actual perceived and actual demanded/anticipated. Furthermore, frontline HCWs reported the highest proportion of the need for a policy on discriminatory HCWs practices (77.9%) and security for the family (77.7%) (online supplemental efigure 3). Moreover, frontline HCWs reported significant differences in the actual received and actual demanded/anticipated of ‘supply of prevention and control materials’, ‘protection and control measures’, ‘protection of rights and interests in epidemic prevention’, ‘more medical personnel to ease the existing overburdened staff’, ‘economic subsidy’, ‘support of providing a place to rest’, ‘support of providing psychological services and help’, ‘policy on discriminatory practices’ and ‘security for the family’ (p<0.05, online supplemental efigure 4).
Supplemental material

{kind=link}
Scores of actual perceived social support and demanded/anticipated social support.
Multivariate analyses
The results of the multivariate linear regression analysis on the influencing factors associated with PTSS scores in frontline HCWs fighting against COVID-19 are shown in table 4. Number of psychological symptoms (β=0.278, p<0.001), number of physical symptoms (β=0.108, p<0.001), emotional exhaustion (β=0.239, p<0.001), depersonalisation (β=0.071, p=0.010), severity perception degree of ‘nowhere to release tension’ (β=0.113, p<0.001), ‘disability to vent emotions’ (β=0.069, p=0.009) and ‘fear of infected’ (β=0.095, p<0.001) were significantly associated with higher PTSS scores.
Multivariate linear regression analysis on influencing factors associated with PTSS scores in frontline HCWs fighting against COVID-19
Frontline HCWs who worked more than 8 hours (β=−0.090, p<0.001) and with the senior professional title (β=−0.114, p=0.003) were significantly associated with lower PTSS scores. In addition, self-reported health (β=−0.077, p<0.001), perfect protection and control measures (β=−0.057, p=0.048), economic subsidy (β=−0.064, p=0.011) and policy on reducing discriminatory practices (β=−0.063, p=0.006) were also significantly correlated with lower PTSS scores. Together, these 13 variables explained 63.3% of the variance in the outcome measures.
Discussion
A meta-analysis confirmed that HCWs exposed to frequently witnessing death and trauma are particularly at risk of PTSS.22 Our results reflected the immediate psychological responses of frontline HCWs to the early stage of the COVID-19 outbreak in China. The prevalence of clinically significant high levels of PTSS among frontline HCWs was 58.1%; the average score of PTSS was 57.17±21.49. The PTSS in this study is more serious than a cross-sectional study launched in a tertiary infectious disease hospital (27.89%, 42.92±17.88),69 indicating that a considerable proportion of the frontline HCWs suffered with high levels of PTSS themselves during their provision of life-saving care service to others in the early stage of the COVID-19 outbreak. The current study provides empirical evidence for the short-term peritraumatic effects of the COVID-19 pandemic and related factors, which can help to guide targeted care and multiple-intervention mental health services (eg, regular screening, early intervention, design prevent strategies) within practices for reducing the risk of high levels of PTSS and managing the psychological impact on frontline HCWs during the pandemic.
There is increasing evidence that PTSD is comorbid with mental and physical symptoms.88 Our results showed that frontline HCWs reported several physical symptoms (2.61±1.65) and psychological symptoms (6.29±4.63), indicating that frontline HCWs in the early stage of the COVID-19 outbreak faced serious health conditions. Specifically, frontline HCWs with more physical or psychological symptoms reported higher PTSS scores. However, a vicious circle involving immunosuppression between COVID-19 and PTSS was revealed.89 The immune mechanism is closely related to physical and psychological health,90 and stress can weaken the immune system91 or precipitate or worsen specific physical symptoms92 such as cardiovascular, respiratory, neurological or gastrointestinal symptoms.93 Meanwhile, acute psychological stress can activate the sympathetic adrenal medulla system and the hypothalamus–pituitary–adrenal axis, and this two-component stress response impacts on physical and mental health and can contribute to diseases.94 Once the immune balance breaks, frontline HCWs are directly exposed to considerable risks. Our results revealed that frontline HCWs tolerated excruciating psychological symptoms (ie, 68.8% experienced fear, 66.6% grief and 63.5% helplessness), and most frontline HCWs reported palpitations (67.6%) and headaches (64.8%). However, physical symptoms (ie, headaches, palpitations) during the COVID-19 outbreak may be over-represented due to psychological stress,93 which may reflect vulnerability to PTSD and compromise HCWs’ resilience after being exposed to a traumatic event.22 Due to the delayed appearance and inconspicuous nature of PTSSs,95 it is essential to monitor these regularly to diagnose and intervene timely and prevent the development of PTSS during the COVID-19 pandemic.96 In this study, compared with the self-reported poor health group, the self-reported good health group had a lower PTSS score. Therefore, it is crucial not to neglect such physical symptoms as they may reflect underlying psychological distress.97 Interestingly, we also found that longer daily work hours were associated with a higher risk of depressive symptoms and PTSD. An overload of work frequently imposes both physical and psychological strains on the medical staff; and the PTSS scores illustrate the importance of reasonable work arrangements for the mental health of the medical staff.98 Targeted multidisciplinary interventions addressing psychological and physical symptoms are needed to support HCWs.
HCWs’ burnout has a significant impact on the wellness and productivity of physicians, as well as on patient health outcomes. The overall pooled prevalence of burnout symptoms among nurses globally was 11.23%.99 A recent study reported that more than 40% of frontline nurses during the COVID-19 pandemic might experience burnout.100 In this study, 57.3% of the frontline HCWs reported emotional exhaustion, while only 35.9% of them perceived the threat of being physically and mentally exhausted (self-reported), indicating severe job burnout, a general lack of awareness and low concern among frontline HCWs. Our results showed that more emotional exhaustion and depersonalisation were positively related to the high PTSS score. Frontline HCWs with medium to high emotional exhaustion reported 57.3% of clinically significant PTSS, respectively. Ruotsalainen et al and Salyers et al proved that effective interventions could reduce emotional exhaustion and suggested a more active stress management policy in healthcare institutions.101 102 In this study, 55.5% of frontline HCWs reported perceived psychological service and help. Therefore, two points need attention: burnout feelings of frontline HCWs are the manifestation of fatigue and disease precursors. Notably, early detection, identification and person-directed and organisational interventions, such as incentives or insurance guaranteed by the government are essential during this pandemic.
Based on the buffering hypothesis/moderator effect model,103 social support is a beneficial factor in reducing the perception of threats, and it acts as an important environmental resource in confronting adverse situations.104 Austin et al confirmed that disproportionate social support has implications for physical health.105 In this study, the actually achieved social support and needed social support were mismatched, which is not consistent with Li et al’s106 findings that the individual’s need for support matches the type of support provided during the COVID-19 pandemic.
As frontline HCWs may underestimate their demand for psychological service, it creates the illusion that their needs are met. Our results indicated that actual perceived support of receiving perceived support from psychological service had the lowest score (3.11±1.37) among all perceived types of social support, and the self-reported need for psychological service and help was only 3.24±1.77. Frontline HCWs focused on the social support from the policy for discrimination and wounded HCWs (77.9%), security for the family (77.7%), economic subsidy (77.1%) and protection of rights and interests in pandemic prevention (76.4%). A meta-analysis of controlled studies involving single-session debriefing after trauma aimed at preventing the development of PTSS failed to show that the intervention was effective.107 Although psychological assistance services, including telephone, internet and application-based counselling or intervention, have been widely deployed by local and national mental health institutions in response to the COVID-19 pandemic,108–110 psychological intervention services were problematic. Chen et al25 reported that medical staff was reluctant to participate in the group or individual psychological interventions. Indeed, frontline HCWs may have been overwhelmed by the emotional impact of the situation.
This ‘matching hypothesis’ suggests that to satisfy the expectations of perceived support, the provider’s actions must meet the specific needs of the recipient, and social support interventions may only be beneficial if the recipient’s support needs are not already being met.111 In this study, higher PTSS scores were associated with low perfect protection and control measures, which is consistent with Muller et al’s suggestion that HCWs are more interested in occupational protection and rest than professional psychological help.42 Frontline HCWs who reported a severe degree of having nowhere to release stress (20.1%) or an inability to vent emotions (24.4%) reported a higher PTSS score than those who did not. Studies have confirmed that people who have suffered traumatic events need to alleviate their emotions timely to prevent the generation of negative emotions.112 113 However, despite the suffocating pressure, frontline HCWs may deliberately suppress emotions due to the sense of responsibility or the desire for professional respect. Problems in the provision of psychological counselling services include psychiatrists who are not willing to provide face-to-face mental health services to other HCWs who are identified as a fragile population in the COVID-19 outbreak,114 and HCWs who report reluctancy in receiving psychological intervention services (eg, due to lack of time or motivation).22 25 Supporting healthcare professionals through psychological services or counselling enables them to become aware of their emotions and remain efficient and focused during these stressful times. Financial stress and legal involvement due to trauma have been addressed in the risks of PTSS.115 Therefore, and based on ‘the Stanford Medicine Hear me, Protect me, Prepare me, Support me, Care for me’ model,116 tangible assistance and effective psychological intervention conducted by multi-agents (eg, organisation, work term, psychiatrist) are needed to explore the flexible demands of psychological support aiming to deal with the serious mental health issues of frontline HCWs involved in the COVID-19 pandemic.117
In the ongoing COVID-19 pandemic, the lack of personal protection devices represents a critical issue.22 Out of the participating HCWs, 36.8% perceived that the supply of prevention and control materials was less than the demand, and 47.5% described dissatisfaction with the hospital’s protective measures. Frontline HCWs perceived mismatches to requirements and acquisition of specific social support. Previous studies have shown that perceived threat is an essential predictor of PTSS.22 Meanwhile, burnout (eg, emotional exhaustion, depersonalisation) was a contributing factor to the higher PTSS score.118 As workers may misidentify traumatic symptoms (eg, arousal, detachment) as burnout rather than a traumatic response referring to PTSS,119 it is necessary to distinguish between PTSS and burnout of HCWs. Workplace health programmes and health surveillance for protecting the mental health of HCWs are needed.40 Among individuals diagnosed with PTSD, men and women are similar in phenotypic expression,120 and we found that males and females have no difference in PTSS scores. In this study, frontline HCWs with family members or close relatives infected with COVID-19 were not significantly related to PTSS scores. This is consistent with ‘the Psychological Typhoon Eye’ effect, indicating that repeated exposure to a catastrophic environment can increase an individual’s level of resilience and improve their ability to resist adverse life events. Therefore, mental health-related factors should be taken into account in the selection of frontier-line medical staff.121 Overall, early comprehensive, extensive longitudinal detection and interventions are essential to rebuild resilient organisations and rapidly reconfigure the well-being priorities to deal with drivers of stress.116
Limitations and recommendation
There are some limitations to our study. First, as it is a cross-sectional study, the relationships between variables were only correlative. Causal relationships could not be established, and evidence from the longitudinal or experimental study should be employed further. Second, the results depended on respondents' online self-reporting instruments, and non-validated questions were used; these are potential sources of biases, and recall bias is inherent in the survey. Results of this study should be interpreted with caution because many of the psychosocial measures analysed were not from validated survey instruments. Third, a strict application of the diagnostic criteria is essential in research on PTSD. PTSD-SS cannot be used as a substitute for full clinical diagnostic criteria or for addressing the conceptual diagnostic problems and designing research to resolve diagnostic uncertainties empirically.122 Qualitative face-to-face interviews to obtain the true inner experience of frontline HCWs are needed. Fourth, frontline HCWs willing to be investigated were included in the study, so there is a bias. Fifth, the study was conducted within a month of the COVID-19 outbreak, which was the peak of the rescue operation and might be time sensitivity assessed PTSS scores, including exposure to numerous potentially traumatic stressors to frontline HCWs. Due to the continuous progress of the pandemic, HCWs’ mental health symptoms may have fluctuated. It is not yet known whether the mental state of frontline personnel will recover. Therefore, long-term psychological implications on this population are worth further investigation.
Conclusion
The prevalence of clinically significant high levels of PTSS, peritraumatic distress and inadequate psychosocial support during the hot phase of the COVID-19 outbreak in China was high among Chinese frontline HCWs. Overall, frontline HCWs experienced physical and psychological burdens, felt they had nowhere to release tension and an inability to vent emotions, reported one or more physical/ psychological symptoms, and felt the stress of insufficient medical supplies at hospitals. Protecting HCWs is an essential component of public health measures to address the COVID-19 pandemic. As HCWs have had a shortage globally, effective and empirical psychological intervention conducted by multi-agents (eg, organisation, work term, psychiatrist) is needed to explore the flexibility demands of psychological support and develop clear pathways to constant effective psychological care for dealing with the serious mental health issues of frontline HCWs involved in the COVID-19 pandemic.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Committee on the Ethics of Harbin Medical University (HMUIRB20200003). Moreover, informed consent was obtained from each participant before the start of work. All voluntary participants gave their informed consent with the assurance of confidentiality and anonymity of the data, according to ethical principles for medical research involving human subjects. The question ‘Do you agree to participate in this survey’ was asked to acquire the consent of the participants and only the ‘Yes’ option led to the next page for the questionnaires. Once completed, the questionnaire could be submitted only once to prevent duplication. This study was conducted by the ethical standards of the Declaration of Helsinki (2008). Participants were invited personally by the investigator, and they were asked to participate voluntarily with a full right to withdraw from the study. The database used in this study contains identification data used to protect the privacy of participants. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors XQ contributed to writing; XQ, QW and JL contributed to conceptualisation and methodology; JW, HL and KW contributed to investigation; YH contributed to project administration; QW and YH contributed to funding acquisition and supervision; DAA and SS contributed to review and editing. QW is the author acting as guarantor.
Funding The National Social Science Fund of China (Grant No.19AZD013); National Natural Science Foundation of China (Grant No. 72042001).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.