Article Text

Abstract
Introduction Gingival recession is one of the most common mucogingival deformities requiring surgical correction. The American Academy of Periodontology Regeneration Workshop recommended connective tissue graft (CTG) combined with coronally advanced flap (CAF) for the treatment of Miller Class I and II single-tooth gingival recession. The disadvantages of harvesting autogenous tissue include postoperative bleeding, pain and discomfort at the donor site, restricted tissue supply, increased morbidity and prolonged operative times. Acellular dermal matrix (ADM) contains undamaged collagen and elastin matrices that can be used as a substitute for CTG during root coverage procedures. However, the use of ADM is still controversial. The objective of this split-mouth; randomised, controlled, clinical study is to evaluate the long-term effects of ADM graft (ADMG) combined with CAF on root coverage, aesthetics and patient satisfaction for the treatment of single gingival recession with thin gingival phenotype.
Methods and analysis Forty participants with bilateral Miller Class I/II gingival recession will be randomised to receive an ADMG on one side and CTG on the contralateral side, combined with CAF. Gingival recession depth, gingival recession width and keratinised tissue width will be measured at baseline, 2 weeks and 1, 3, 6, 12 and 24 months. Mean root coverage, complete root coverage, root coverage aesthetic score, colour change (∆E) and patient satisfaction will be assessed during follow-up visits.
Ethics and dissemination The present study has received approval from the Ethics Committee of Peking University School and Hospital of Stomatology (PKUSSIRB-202054029). Data of this study will be registered with the International Clinical Trials Registry Platform. Additionally, we will disseminate the results through scientific journal.
Trial registration number ChiCTR2000033230.
- oral & maxillofacial surgery
- plastic & reconstructive surgery
- clinical trials
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This will be a double-blind, split-mouth randomised controlled clinical trial.
This trial will compare the long‐term outcomes of acellular dermal matrix graft and connective tissue graft for treating gingival recessions with thin gingival phenotype.
The patients will be followed up for 24 months.
The results of this trial will improve treatments for gingival recession.
The main limitation of this study will be that the condition of exposed roots will not be evaluated.
Introduction
Gingival recession is defined as exposure of the root surface due to apical migration of the gingival margin to the cemento-enamel junction (CEJ).1 2 It is a common problem,3–5 affecting 51% of the population.6 7 Gingival recession is caused by anatomical and mechanical factors, such as biological width invasion, injury related to toothbrushing or oral piercing, muscle insertions and inflammation due to plaque.7 8 Exposed root surfaces are associated with many problems, including dentinal hypersensitivity, poor dental aesthetics, root erosion, root caries and inadequate plaque removal.9 Therefore, many patients request surgery for coverage of exposed root surfaces.
Different surgical techniques have been used for root coverage.10–20 The coronally advanced flap (CAF) is an important component of periodontal plastic surgery used to treat Miller Class I/II gingival recessions. CAF can be used alone,21 22 or in conjunction with a connective tissue graft (CTG),23–26 enamel matrix derivative (EMD),27 platelet-rich fibrin (PRF)28 or low-intensity laser therapy29 to improve outcomes. A systematic review30 reported that CAF, with or without CTG, for the treatment of Miller Class I/II recessions achieved predictable complete root coverage (CRC). The combination of CAF and CTG was associated with greater long-term stability of CRC, and is therefore the gold standard treatment for gingival recessions.31 32
The subepithelial connective tissue procedures provide excellent outcomes. They require two surgeries, which increases patient discomfort and the risk of postoperative pain and bleeding. In addition, the amount of graft may be limited by the palatal donor site and thickness, especially in the multiple gingival recession sites treatment.33–35 To overcome the limitations of autogenous tissue harvesting, PRF,28 platelet-rich plasma (PRP),36 EMD,37 xenogeneic collagen matrix (XCM)38–40 and acellular dermal matrix (ADM)41 42 and xenogeneic acellular dermal matrix43 44 have been used as alternatives to CTG for plastic periodontal and implant surgery.
ADM involves the removal of cellular and epidermal components of human dermis, to eliminate the source of disease transmission and immunological reactions, which leaves a structurally intact connective tissue matrix, composed of collagen fibrillar network, proteins, elastin filaments, proteoglycans, hyaluronan and a basement membrane. Therefore, the ADM possesses the characteristics of a soft tissue graft material, and can be used as a scaffold to promote the growth of host tissues.45 ADM was first used in the 20th century,46 47 and has since been used extensively in various areas of dental practice.31 48 ADM graft (ADMG) is recommended as an alternative to autogenous CTG for the treatment of alveolar ridge deformities,49 to increase the width of the keratinised tissue (KT) around teeth and implants50–52 and to guide bone53 54 or tissue regeneration55 and root coverage.56 57 Although the clinical efficacy of ADMG has been discussed in several reviews,31 48 58 the application of this material is still controversial. Moreover, the data on the long-term clinical and patient-reported outcomes after ADMG are of low quality.
Gingival phenotype affects the clinical outcomes of root coverage procedures.59 60 Gingival thickness (GT) less than 1 mm is associated with a lower likelihood of CRC.61 GT may have a greater influence on the final outcome of root coverage procedures than the amount of KT.59 62 The ADM, as a ‘non-vital’ structure, depends on the recipient site for cells and blood supply for reorganisation. Therefore, the gingival phenotype is critical for a good clinical outcome. To the best of our knowledge, no randomised controlled clinical trial has compared the outcomes of CTG and ADM for the treatment of gingival recessions in patients with thin gingival phenotype. Therefore, the aim of this study is to compare root coverage, aesthetics and patient satisfaction between ADMG combined with CAF and CTG combined with CAF for the treatment of Miller Class I/II gingival recessions in patients with thin gingival phenotype.
Methods and analysis
This will be a prospective, single-centre, split-mouth randomised controlled clinical trial including 40 patients with Miller Class I/II gingival recessions who require root coverage. This study will be conducted at the First Clinical Division, Peking University School and Hospital of Stomatology, China. This study was approved by the Biomedical Ethics Committee of Peking University School and Hospital of Stomatology (PKUSSIRB-202054029), and registered in the International Clinical Trials Registry Platform (ICTRP). Figure 1 summarises the research framework.

Consolidated standards of reporting trials diagram. ADMG, acellular dermal matrix graft; CAF, coronally advanced flap; CTG, connective tissue graft.
Participant selection
Patients scheduled for a root coverage procedure at the First Clinical Division, Peking University School and Hospital of Stomatology, and who provide written, informed consent, will be recruited to the study.
Patients who meet the following inclusion criteria will be included: (1) age ≥18 years; (2) willing to attend the study and provide an informed consent; (3) systemically healthy with no contraindication to periodontal surgery; (4) Miller Class I or II adjacent gingival recessions≥3 mm and a thin gingival phenotype (the white colour of a colour-coded phenotype probe (Hu-Friedy, Chicago, Illinois, USA) inserted into the sulcus should be clearly visible through the tissue63–65) affecting the same teeth (central or lateral incisors, canine or first or second premolars) on each side of the maxillary or mandibular arches, without any evidence of active or chronic periodontal disease; (5) gingival recession with at least 1 mm of KT apical to the recession; (6) full-mouth plaque and bleeding scores≤15% (7) and no history of surgery in the relevant areas. In patients with multiple recessions, the deepest one will be selected, if all recessions are of the same depth, one will be selected according to the result of a coin toss.66
Patients with any of the following will be excluded: (1) habitual tobacco smoking and/or chewing; (2) habitual alcohol consumption; (3) pregnant or lactating women; (4) history of dental crown placement; (5) restorations involving the CEJ, or those with non-identifiable CEJ and (6) penicillin allergy or use of medications that may interfere with healing.
Patient and public involvement
The priorities, experiences and preferences of patients will not be used to develop the research question or outcome measures. Patients will not be involved in the design, recruitment or conduct of the study. The study results will be disseminated through publications in dental journals. The study outcomes will be assessed by periodontists. Patient advisors will be acknowledged in the manuscript.
Randomisation and blinding
Patients will be randomised by a professor using a software programme that generates random permuted blocks. The investigators will be blinded to the randomisation, and the allocation will be concealed in opaque envelopes, which will be opened immediately before the surgery to determine the test site. The corresponding contralateral tooth will be subjected to the control procedure. All participants will be treated by an experienced periodontist who will not be involved in the allocation, examination or statistical analysis. The examiner and statistician will be blinded to the treatment plan and allocation. Unblinding will be permissible in cases of postoperative adverse events.
Interventions
All surgeries will be performed at the First Clinical Division, Peking University School and Hospital of Stomatology by the same periodontist. Preoperatively, the periodontal status will be evaluated, a comprehensive clinical examination will be performed and the aetiology of the recessions will be determined by a calibrated examiner. Identified etiological factors will be treated as necessary, oral hygiene instructions (OHI) will be provided and full-mouth supragingival scaling and polishing will be performed. The participants will be re-evaluated at least 4 weeks before the surgery to confirm that they meet the inclusion criteria and have good oral hygiene.
The surgeries are performed by an experienced periodontist. Both the test and control surgeries will be performed during the same visit. The same surgical procedure will be used for both the test and control sites, except that the test sites will receive ADMG and the control sites CTG (figure 2). Following local anaesthesia, a CAF will be designed using the method described by Zucchelli et al.67 Briefly, an intracrevicular incision will be made at the bottom of the crevice. Two mesial and distal vertical releasing incisions will be made, including the papillae adjacent to the area of gingival recession. The papillae will be de-epithelialised by interdental incisions. The flap will be elevated using a split-full-split approach in the apico-coronal direction, and full-thickness soft tissue apical to the exposed root will be elevated to cover the recession area. Finally, the apical part of the split-thickness flap will be raised to release muscle tension, and the flap will be positioned passively over the CEJ without tension. Following flap elevation, the exposed root surface will be gently planed using sharp curettes (Gracey Curettes, Hu-Friedy, Chicago, Illinois, USA).

{kind=link}
{kind=link}
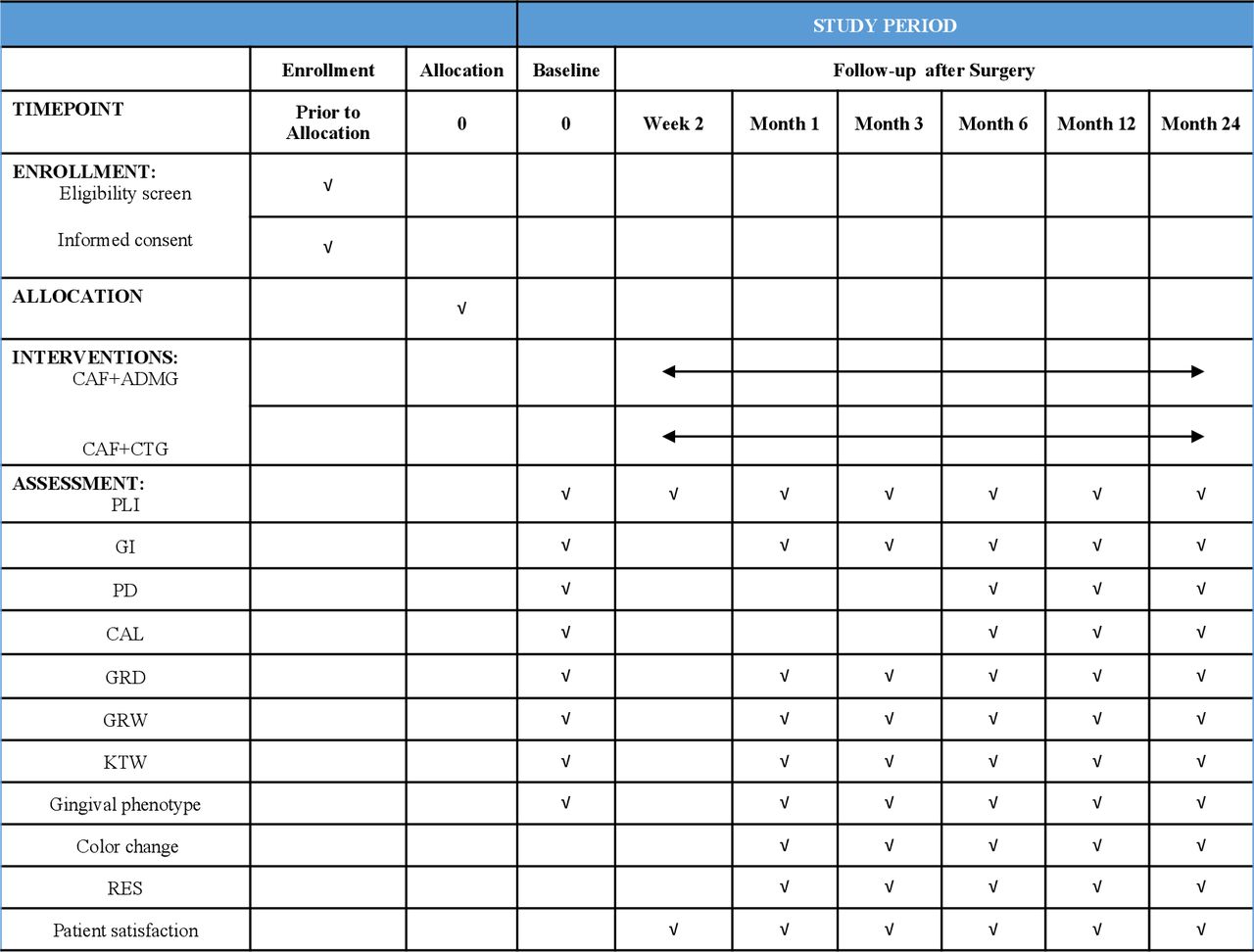
The schedule of enrolment, intervention and assessments. ADMG, acellular dermal matrix graft; CAF, coronally advanced flap; CAL, clinical attachment level; CTG, connective tissue graft; GI, gingival index; GRD, gingival recession depth; GRW, gingival recession width; KTW, keratinised tissue width; PD, probing depth; PI, plaque index; RAS, root coverage aesthetic score.
As previously described, a single-incision technique will be used to obtain the subepithelial CTG (without harvesting the periosteum) from the lateral palate in the control group.23 The connective tissue will be trimmed to a shape and size appropriate to cover the root surface and surrounding bone. The graft will be 1-mm thick.
In the test group, exposed root surface will be treated with ADM (Qingyuanweiye, Beijing, China) that is aseptically rehydrated in sterile saline. ADM will be rinsed with sterile saline three times before use, in accordance with the manufacturer’s instructions. The graft will be trimmed to a shape and size appropriate to cover the root surface and surrounding bone. In accordance with the technique described by Harris, the graft will be positioned with the basement membrane adjacent to the bone and tooth, and the connective tissue adjacent to the flap.68 The graft will be 1-mm thick.
The ADM and CT will cover the recipient area at the level of CEJ on the coronal site, as well as the vascular tissues located 3 mm lateral and apical to the recession. The grafts in both groups will be secured in the interdental areas and lateral sites using bioabsorbable suture material (6–0, DS-12; Serafit; Serag-Wiessner, Naila, Germany). The CAF will be positioned 1 mm coronal to the CEJ, covering the entire graft in both groups.67 The CAF will be sutured using non-absorbable suture material (6–0, DS-15; Seralene; Serag-Wiessner, Naila, Germany) by sling and interrupted technique, without creating tension. This suture will also be used to secure the donor site. Microsurgical hand instruments (Hu-Friedy, Chicago, Illinois, USA) and 4.0×loupe (Q Optics, Texas) will be used during surgeries. No periodontal dressing will be used postoperatively.
All patients will be instructed to discontinue tooth brushing, and to avoid trauma or pressure at the surgical site. Gargling with 0.12% chlorhexidine digluconate will be prescribed two times per day for 14 days,69 and amoxicillin (500 mg, three times per day) will be prescribed for 7 days.
The sutures will be removed 14 days after surgery, and the patients will be instructed continuing to clean the surgical sites with 0.12% chlorhexidine digluconate gargling two times per day in the next 14 days, following which use of a soft toothbrush (with the careful roll technique) will be allowed over the treated areas for 8 weeks. During follow-up visits, OHI will be re-emphasised, and the teeth cleaned if needed.
Examination
At baseline, acrylic stents will be prepared for use as a reference when positioning the probe, and to ensure reproducibility during follow-up examinations.
Clinical parameters including plaque index (PLI), gingival index (GI), probing depth (PD), clinical attachment level (CAL), gingival recession depth (GRD), gingival recession width (GRW) and keratinised tissue width (KTW) will be measured using a periodontal probe (PCP-UNC 15; Hu-Friedy, Chicago, Illinois, USA) and rounded to the nearest 0.5 mm. The parameters will be measured by a calibrated examiner (not the therapist), who will be trained to ensure adequate levels of accuracy and reproducibility. Colour-coded phenotype probes (Hu-Friedy, Chicago, Illinois, USA) will be inserted into the sulcus to determine the gingival phenotype. Gingival biotype will be classified as thin (white portion of the probe clearly visible through the tissue), medium (green portion, but not the white one, of the probe clearly visible through the tissue), thick (blue portion, but not the white or green one, clearly visible through the tissue) or very thick (none of the colours visible through the tissue).63–65
Participants will be re-evaluated at 2 weeks and 1, 3, 6, 12 and 24 months after surgery (figure 2). At 1, 3, 6, 12 and 24 months after surgery, the PLI, GI, PD, CAL, GRD, GRW, KTW, gingival phenotype, aesthetic outcomes (root coverage aesthetic score, RAS)70 and colour measurements using an intraoral spectrophotometer (SpectroShade, Medical High Technologies) will be evaluated by a calibrated examiner.
Visual Analogue Scale/Score (VAS) will be used to evaluate patient satisfaction with root coverage; gingival colour, shape and contour; pain and discomfort during the surgery and postsurgical pain, swelling and complications.71
The primary outcomes of this study are mean root coverage (MRC), CRC, KTW, RAS and colour change (∆E). The MRC percentage (%) will be calculated as follows: ((baseline GRD − GRD at 1, 3, 6, 12 and 24 months)/baseline GRD) ×100%. The CRC percentage (%) will be calculated as the percentage of teeth with gingival recession that achieved complete coverage, as follows: ((teeth with CRC)/(all treated teeth))×100%. The secondary outcomes of this trial are PD, CAL and VAS of patient satisfaction.
Sample size
The sample size of this trial was calculated using the following formula:  . In the preliminary experiment results and previously published articles,72 the mean difference of the reduction in gingival recession (δ) was around 0.1 mm and the standard deviation (σ) was around 0.3 mm.
. In the preliminary experiment results and previously published articles,72 the mean difference of the reduction in gingival recession (δ) was around 0.1 mm and the standard deviation (σ) was around 0.3 mm.
If the inspection level (α) is set at 0.05 and the power of test (β) at 90%, 36 participants will be required for each group. Assuming a loss to follow-up of 10%, 40 participants will be required in each group.
Statistical analysis
The statistical analysis will be performed using a software program (SPSS V.22; IBM Corp., Armonk, New York, USA). The distribution of the variables was validated by D’Agostino-Pearson omnibus normality test. Parametric tests will be used for intergroup and intragroup comparisons. The paired t-test will be used for intergroup comparisons of the PLI, GI, PD, CAL, GRD, GRW, KTW and changes therein. Intragroup comparisons for the same variables will be performed using repeated measures one-way analysis of variance test, and followed by Bonferroni correction for post hoc multiple comparisons. The number of teeth with MRC and CRC in both groups will be compared using Fisher’s exact test. Multiple imputations will be used to handle missing data. Two-tailed p-values<0.05 will be considered statistically significant.
Data analyses will be performed using SPSS software (V.22; IBM Corp., Armonk, New York, USA).
Withdrawal
Participants will be allowed to withdraw from the study at any time without providing a reason. If a participant withdraws from the study, their treatment will not be affected. Intervention may be discontinued in case of postoperative adverse events.
Dissemination of data
The results of this trial will be published at the International Clinical Trials Registry Platform (ICTRP) and in an international peer-reviewed journal, to ensure that the results are accessible to the public.
Discussion
Several graft substitutes for CTG and surgical techniques have been investigated to treat gingival recession.44 73 74 ADM may increase the coverage of exposed roots and thickness of the keratinised gingiva.75 76 However, previous studies that compared ADM and CTG reported conflicting results.75 77–79
Clinicians are becomingly increasingly interested in the long‐term outcomes of root coverage procedures.80–82 A study of the 20‐year outcomes of CAF alone for the treatment of localised gingival recession reported that gingival recession decreased from 68.59% (at 1 year) to 56.11% (at 20 years), and the gingival margin remained stable in 56% of the treated sites.81 In other study publiced by the same authors, patients treated with CAF +CTG for gingival recession were also evaluated, and CTG was reported to durable results, with minimal changes observed in the MRC (from 74.23% at 1 year to 67.69% at 20 years).83 Similar results were reported for the recurrence of gingival recession following root coverage procedures.78 80 81 84 A recent systematic review and network meta-analysis of periodontal soft tissue phenotype reported that graft materials significantly increased the GT. Additionally, KT was significantly increased after CTG and ADMG. The modification of periodontal soft tissue phenotype increased the expected benefits in root coverage procedures.62 Previous studies have only evaluated the short-term outcomes of ADM during root coverage procedures.85–87 However, long‐term clinical studies reported significant worsening of the outcomes of root coverage using ADM.75 78
This study aims to compare the long‐term outcomes of ADMG and CTG for treating single-tooth gingival recessions with a thin gingival phenotype. To the best of our knowledge, no previous studies have evaluated this. We hope that our results will improve the treatment for gingival recession. The main limitation of this study will be the lack of appraisal of the condition of exposed root. Additionally, the size of CTG may be limited by the palatal donor site in patients with multiple gingival recessions. Therefore, further studies will be required to evaluate the role of ADMG in the treatment of multiple gingival recessions.
Trial status
The trial has been registered at International Clinical Trials Registry Platform (ICTRP), registered on 25 May 2020. The recruitment began in June 2020, and the recruitment will be completed in June 2021.
Ethics and dissemination
The present study has received approval from the Ethics Committee of Peking University School and Hospital of Stomatology (PKUSSIRB-202054029). The patients will be enrolled in this trial only after their signature has been obtained. The study will be performed according to the 2013 revision of the Helsinki Declaration of 1975. Personal information of all subjects will be stored in Peking University School and Hospital of Stomatology. Data of this study will be registered with the International Clinical Trials Registry Platform. Additionally, we will disseminate the results through scientific journal.
Ethics statements
Patient consent for publication
Acknowledgments
We thank all enrolled subjects and patient advisers for their participation.
References
Footnotes
Contributors YZ, MW and FL conceive the study design and drafted the protocol. XC participates in the recruitment and allocation. YZ is the major contributor in writing the manuscript. All authors read and approved the final manuscript.
Funding This study is supported by research funds from the National Key Research and Development Programme: 2019YFB1404801 and the National Natural Science Foundations of China (NSFC): 81 800 976.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.