Article Text

Abstract
Introduction Osimertinib, a third-generation epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor (TKI), is widely used as the first-line treatment for EGFR mutation-positive non-small cell lung cancer (NSCLC). Nevertheless, most cases ultimately acquire resistance to osimertinib, and no effective treatment has been currently established for cases having progressive disease (PD) with osimertinib. In clinical practice, EGFR-TKI therapy could be continued beyond response evaluation criteria in solid tumours (RECIST)-defined PD cases when they are clinically stable. Currently, the progression pattern of osimertinib and criteria for identifying patients who might benefit from osimertinib beyond PD are unknown. In addition, the efficacy and safety of osimertinib as the first-line treatment in real-world clinical practice remain unclear in Japan. This multicentre study was designed to evaluate the real-world data on first-line osimertinib and its post-treatment.
Methods and analysis The study enrols patients with EGFR mutation-positive, advanced or recurrent NSCLC who received EGFR-TKI as the first-line therapy after 1 September 2018, from October 2019 to August 2020, and those started on osimertinib will be followed up until August 2022. We will evaluate the efficacy and safety of the first-line osimertinib treatment, adherence to it, progression patterns on RECIST PD and subsequent treatment.
Ethics and dissemination All participating patients will provide written informed consent before entering the study. The protocol, amendments and patients’ informed consent forms will be approved before study commencement by the institutional review board or independent ethics committee at each participation site (Lead Ethics Committee; Japan Red Cross Medical Center (26 April 2019, order number 976)). Patients will be anonymised before registration into the study and their anonymised data will be collected from the case report form. The results of this study will be presented at the national and international conferences and submitted for publication.
Trial registration number UMIN000038683.
- clinical trials
- oncology
- respiratory medicine (see thoracic medicine)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The strength of this study is that it is the first large, multicentre study in Japan to investigate osimertinib as the first-line treatment in real-world clinical practice.
This study confirms the progression pattern of osimertinib and examines the optimal subsequent treatment.
The factors that make osimertinib less effective will be analysed by identifying medication adherence.
The classification of the progression pattern in this study is yet to be validated.
End points with small number of events might not be adequately analysed.
Introduction
Lung cancer is the most leading cause of cancer deaths in developed countries, including Japan. In Japan, non-smallcell lung cancer (NSCLC) accounts for approximately 85% of all lung cancers, and among non-small cell cancers, approximately 45% of adenocarcinomas are known to have activating mutations of the epidermal growth factor receptor (EGFR) gene.1 Patients with advanced or recurrent NSCLC with EGFR mutations have been reported to be highly responsive to first-generation and second-generation EGFR-tyrosine kinase inhibitors (TKIs); however, they become resistant to EGFR-TKIs, and the median progression-free survival (PFS) with EGFR-TKI is approximately 9–14 months.2–5
Notably, approximately half of the resistance was determined to be because of the acquired T790M mutation,6 and osimertinib, a third-generation EGFR-TKI, was noted to be effective against T790M mutation-positive lung cancer and was initially established as the standard treatment for T790M mutation-positive lung cancer.7 More recently, osimertinib has been shown to provide a significantly longer PFS and longer overall survival (OS) than the first-generation EGFR-TKI as the first-line treatment for EGFR mutation-positive NSCLC, which has been noted to be more effective and provided a longer PFS than the second-generation EGFR-TKI.8 9 Currently, osimertinib is widely used as the first-line treatment for EGFR mutation-positive NSCLC with or without T790M mutation.
We have previously studied EGFR mutation-positive NSCLC in Japanese patients treated with first-generation and second-generation EGFR-TKIs, such as gefitinib, erlotinib and afatinib after being diagnosed as progressive disease (PD) per the response evaluation criteria in solid tumour (RECIST) criteria.10 In that study, when RECIST PD was determined, several patients were not clinically PD, and 35% of patients continued to receive EGFR-TKI. The median time from RECIST PD to clinical PD or discontinuation of EGFR-TKI was 5 months, and no major differences were observed regarding OS or survival after PD with RECIST related to continuing EGFR-TKI treatment beyond PD than stopping EGFR-TKI treatment during RECIST PD. Because several patients are clinically stable even after being diagnosed as RECIST PD, EGFR-TKI therapy is often continued beyond PD in clinical practice. Moreover, it has been reported that the addition of radiotherapy to EGFR-TKI could have favourable outcomes,11–15 if the progression site is limited to brain metastases only.16 17
Most cases receiving osimertinib also ultimately acquire resistance to it, with the median PFS of 19 months.8 However, currently, no effective treatment has been established for PD after osimertinib. In the Japanese subset of the FLAURA study, PFS was prolonged with osimertinib compared with first-generation TKIs, but its initial superiority in OS disappeared in the middle of the curve, which may be because of the post-treatment effect of the first-line TKIs.18
Clinicians have to decide when observing PD to osimertinib whether to discontinue or continue the drug or to switch to cytotoxic anticancer drug. Hence, information regarding the progression pattern at the time of PD would be useful in deciding the optimal treatment after osimertinib resistance. Yang et al reported that the clinical mode of failure of EGFR-TKIs can favour strategies for subsequent treatment and predict survival benefit in advanced NSCLC.19 Progression patterns to TKIs could be divided into progression of brain metastasis alone, progression of oligometastasis, systemic progression,20 progression on imaging alone and clinical PD.10 Per the former classification, patients with brain metastasis alone or oligometastatic progression could continue osimertinib treatment with the addition of local therapy,16 17 and in the latter classification, patients without clinical PD might continue osimertinib treatment beyond PD. However, currently, the progression patterns of osimertinib are not investigated, and neither the clinical relevance of ‘osimertinib beyond PD’ nor the criteria for identifying patients who would benefit from it is known. In addition, the efficacy and safety of osimertinib as the first-line treatment in real-world clinical practice remain to be fully established in Japan, as is shown in the FLAURA Japanese subset data.
In this study, we will survey the choice of EGFR-TKIs used as the first-line therapy in patients with advanced or recurrent EGFR mutation-positive NSCLC and evaluate the efficacy and safety of osimertinib treatment in clinical practice, the progression patterns in RECIST PD with osimertinib and subsequent treatment. In addition, we will examine the factors that make osimertinib less effective by identifying medication adherence.21 22
Methods and analysis
Design
This observational study is a multicentre, prospective cohort study involving patients with EGFR mutation-positive advanced or recurrent NSCLC in Japan. The study does not include any particular intervention, patients will be managed using routine clinical care, and all treatments and examinations will be performed as in regular practice. The study will periodically survey and collect data on the registered patients using medical records. Overall, 35 institutions in Japan, including cancer centres, university hospitals and community hospitals, participated in the study.
Patient and public involvement
There is no patient and public involved in the study. In principle, the results of the study will be disclosed if the research participant wishes to disclose the results of the study.
Study period
The study will be conducted from October 2019 to June 2023. Registration will take place from the approval date of ethical review at each institution to August 2020. The follow-up period will extend until August 2022 (2 years after the last patient was enrolled). Data entry and analysis will be completed by June 2023 (10 months after the last patient is observed).
Participants
Patients will be included in the study if they are aged ≥20 years and have advanced or recurrent metastatic NSCLC (the stage will be defined based on the UICC International Union for Tumors Lung Classifications (2017, 8th edition)), that is, EGFR activating mutation-positive. Recurrent metastatic NSCLC is defined as patients who cannot be treated with local treatments alone and require systemic chemotherapy with EGFR-TKIs. Notably, any type of EGFR mutation will be acceptable. In addition to exon 19 deletion and exon 21 L858R susceptibility gene mutations (common mutations), rare EGFR mutations (uncommon mutations) will be eligible. Moreover, an additional eligibility criterion will be for patients to have started their first EGFR-TKI treatment on or after 1 September 2018.
Regarding EGFR-TKI treatment, patients who used anticancer drugs as local therapy like pleurodesis, patients treated with cytotoxic chemotherapy as prior therapy, patients treated with EGFR-TKIs and other anticancer drugs or angiogenesis inhibitors, patients who were primarily treated with EGFR-TKI as monotherapy and alternating between EGFR-TKI and other anticancer drugs, and patients who were enrolled in other clinical trials will also be deemed eligible.
Patients who had started EGFR-TKI treatment before 1 September 2018, and patients deemed inappropriate for inclusion by each investigator will be excluded.
Research procedures
The investigators will select patient candidates, obtain written informed consent, complete the case registration form and fax it to the data centre. The data centre will verify the patient’s eligibility and register the patient based on the case registration form.
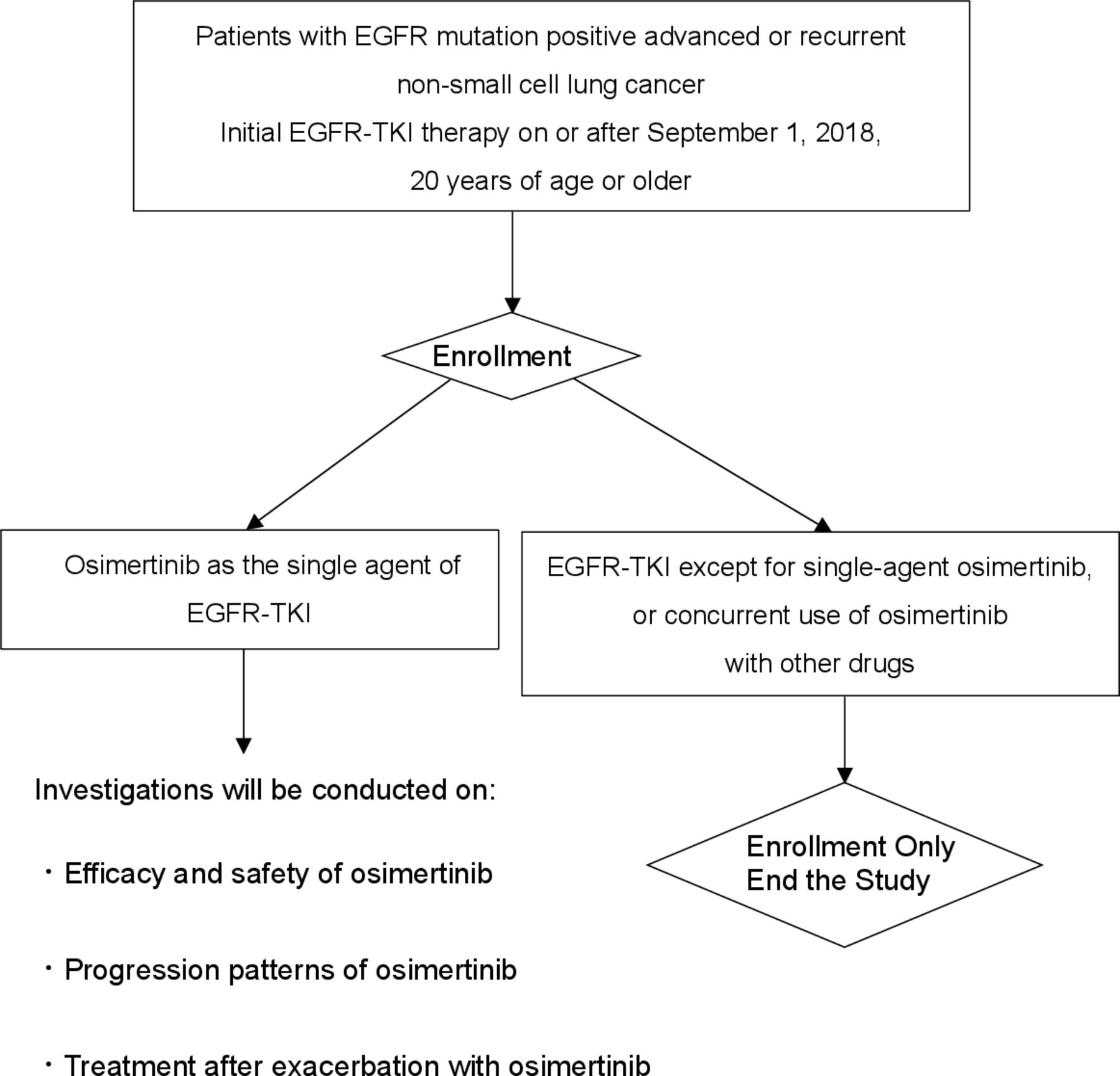
The patients will be classified into two groups based on the data provided at enrolment (figure 1). One group will comprise patients treated or to be treated with EGFR-TKI other than osimertinib, and patients treated or to be treated with osimertinib in combination with other anticancer drugs or angiogenesis inhibitors from the beginning of treatment. The other group will comprise patients who started or will start osimertinib monotherapy. Patients who have been receiving combination therapy with other anticancer drugs or angiogenesis inhibitors during the course of osimertinib treatment or who have been receiving replacement therapy with other anticancer drugs will be included in this group provided they were initially treated with osimertinib monotherapy.
{kind=link}
Study schema. EGFR, epidermal growth factor receptor.
For the first group, the study will be completed at the time of enrolment survey with confirmation of patient characteristics, details of EGFR-TKI therapy and concomitant drugs before initiation of EGFR-TKI therapy. In the second group, the study will continue survey until the end of the study period. Each survey will include treatment details, concomitant medications, imaging assessments, clinical exacerbations, flare events, adverse event reports, outcomes and post-treatment details after osimertinib treatment. The investigators will conduct a simultaneous survey once every 6 months, using medical records from enrolled patients. The final survey will be conducted 2 years after the last patient was enrolled. The results of each study will be recorded in a continuing case report form for each study and sent to the data centre.
Patient-reported osimertinib compliance survey will be conducted in patients who were started newly on osimertinib since the start of the study. Patients will be given a medication notebook, which they will fill out themselves, and a copy of the notebook will be mailed to the data centre 180 days after starting osimertinib with a medication investigation report for each patient.
All adverse events occurring during osimertinib treatment that are suspected to be related to the treatment will be documented in the continuing case report form, regardless of the severity. In the event of a serious adverse event, the standard reporting protocol of a serious adverse event will be performed appropriately, including reporting to the head of the medical institution and the authorities. In addition to that, the study mandates that the report be emailed to the administrative office within 24 hours and the primary report be emailed to the administrative office within 72 hours, using the ‘Emergency Adverse Event Notification Form’. Finally, the administrative office will report the serious adverse event to the principal investigator of the study and AstraZeneca through email.
Data management and monitoring
Data will be centrally managed at the designated data centre. Central monitoring will be performed to ensure that the study is conducted safely and in accordance with the protocol.
End point
This study’s primary endpoint is coprimary endpoint. First primary endpoint is PFS of osimertinib, time from the start of osimertinib to RECIST PD or death from any cause. Another primary endpoint is percentage of patients with progression patterns listed below when RECIST PD was encountered with osimertinib treatment. This progression pattern classification was modified from the paper by Goto et al10; however, this is yet to be fully validated. Progression patterns are classified into nine categories (3×3) based on progression site and patient status as follows:
A. Progression patterns based on progression sites
(A1) Central nervous system only (including brain metastasis and carcinomatous meningitis)
(A2) Oligometastasis (one to three lesions in one organ other than the brain)
(A3) Progression in multiple organs (except A1 and A2).
B. Symptoms at exacerbation and exacerbation patterns per the patient’s general condition
(B1) Asymptomatic, without progression as defined by B3 (This pattern is applied when a patient has PD on RECIST due to the appearance of a new lesion or the enlargement of a target or non-target lesion, but the appearance or enlargement of the lesion is asymptomatic and the patient has no symptoms.)
(B2) Symptomatic, without progression as defined by B3
(B3) Decreased PS (Performance Status) or major organ-threatening conditions (cancerous lymphangitis, bone marrow metastasis, carcinomatous meningitis, hepatic metastasis with hepatic disorder, etc).
The study has several secondary endpoints, which are listed below
Response rate of osimertinib in patients with measurable lesions.
OS (time from the start of osimertinib to the date of death, irrespective of cause of death).
Percentage of patients who continued or discontinued osimertinib at RECIST PD.
Number and type of drugs prescribed concomitantly with osimertinib (polypharmacy): oral drugs are classified and aggregated according to the type (gastrointestinal, antihypertensive, diabetic, etc) and number (less than 5, 5–9, 10 or more).
Osimertinib adherence (survey of actual conditions using the medication handbook).
Duration of osimertinib treatment.
Percentage of patients who experienced flare, defined as rapid disease deterioration within 1 month resulting in hospitalisation or death, after discontinuation of osimertinib treatment, except in cases of infections, venous thrombosis and other causes not directly related to NSCLC exacerbation.10
Percentage of patients receiving concurrent chemotherapy or radiotherapy along with osimertinib after osimertinib PD.
Percentage of patients who received chemotherapy after discontinuation of osimertinib treatment.
Percentage of patients readministered osimertinib after more than 4 weeks of discontinuation (if it is less than 4 weeks, it will be considered to be temporary interruption rather than discontinuation).
Percentage of patients with advanced or recurrent EGFR mutation-positive NSCLC receiving osimertinib as initial therapy after September 2018 when osimertinib was approved for use in patients with NSCLC untreated with EGFR-TKI in Japan.
Effects of osimertinib in patients with uncommon EGFR mutations.
Incidence of grade 3 or higher adverse events with osimertinib treatment.
Incidence of pneumonitis caused by osimertinib.
Effects of osimertinib in patients with uncommon EGFR mutations will be analysed within secnodary endpoint 12, and other efficacy endpoints will be analysed for common EGFR activating mutations.
In addition, we will also perform exploratory analysis to investigate the content and efficacy of post-treatment after osimertinib PD.
Sample size
Between September 2018 and August 2020, 700 patients were expected to be enrolled from 50 potential participating institutions. Of the 700 patients, the proportion of osimertinib was estimated to be 70% on average over 2 years, and the number of patients treated with osimertinib was considered to be 500. Based on previous clinical trial data, the median PFS for osimertinib is expected to be about 19 months. The study has a 2-year enrolment period and a follow-up period of 2 years from the last patient’s enrolment. Therefore, all 500 patients will be followed up for more than 2 years. For PFS, which is one of the primary endpoints, we would expect events to occur in more than 60% of cases (number of events was 361, assuming a constant rate of enrolment over 2 years, minimum follow-up of 2 years and an exponential distribution of median PFS of 19 months), and we believe that one of the primary endpoints, that is, the pattern of exacerbations, could be evaluated.
Data analysis
All efficacy analyses will be based on the full analysis set (and per protocol set for supportive analysis). The results of all statistical analyses will be performed using 95% CIs and two-sided p values. Final analyses will be performed for all endpoints after the data have been finalised after the final investigation.
PFS, OS and duration of osimertinib treatment will be summarised using Kaplan-Meier methods, and 95% CI of median time will be calculated using Brookmeyer and Crowley based on the log–log transformation of survival function. For PFS, we will perform subgroup analyses for the following covariates: gender (male, female), age (≧≥65 years, <65 years), primary disease (clinical stage, histology, metastatic organ), smoking history (yes, no), PS (0, 1), types of EGFR mutations, provided there is a certain number of events in each category. Regarding the percentage of patients with nine progression patterns as the primary endpoint, the percentage of response rate and the percentage of patients with various secondary endpoints, the ratio and the 95% CI of Clopper-Pearson will be calculated.
Ethics and dissemination
This study will be conducted per the principles of the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research Involving Human Subjects. All participating patients will provide written informed consent before entering the study. However, informed consent will not be required for patients who are dead at the time of registration. The protocol, amendments and patient informed consent forms will be approved by the institutional review board or the independent ethics committee at each participating site before study commencement (Lead Ethics Committee; Japan Red Cross Medical Center (26 April 2019, order number 976))
Furthermore, for data management and to ensure patient privacy, patients will be anonymised before registration, and their anonymised data will be collected using the case report form. All personnel involved in the study will ensure confidentiality of all participating patients. The anonymisation procedure planned is as follows: the investigators at each institution will give each participating patient an original number unique to the institution that is unrelated to the name and hospital ID of the patient and register the patient in the data centre using that original number. Subsequently, the data centre will assign a registration number for this study. Each institution will prepare a list of correspondence between the original number of the institution and the registration number of this study, which will be strictly controlled by the institution. Enrolled patients are identified and queried using the registration number of this study. Information that can be used by a third party to directly identify a registered patient, such as the medical record numbers in clinical practice or the names and contact details of a registered patient, will not be provided to the data centre and not be registered at the data centre. Data collected from patients in this study will not be used for any other purpose, and potential information that discloses patient identity will not be published.
Discussion
This is the first study to evaluate the efficacy and safety of first-line osimertinib in real-world clinical practice in Japan. Moreover, this study will determine the pattern of exacerbation of osimertinib in RECIST PD and investigate and analyse the real-world post-treatment. The study results will help identify the optimal treatment of patients with EGFR mutation-positive NSCLC based on the real-world exacerbation patterns after first-line osimertinib treatment. The results of this study will be presented at the national and international conferences and will be submitted for publication. We expect that all the data obtained and analysed by this study will facilitate improved treatment strategies in the future for patients with EGFR mutation-positive lung cancer.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank the Data and Safety Monitoring Committee Junji Furuse and Toshimi Takano; the data centre, Hiroshi Otsu and Akemi Yasuhara; and Akira Yamao and Miho Akita of Public Health Research Center Comprehensive Support Project for Oncology Research, the administrative office.
References
Footnotes
Contributors KW, KY, YH, KaU, GN, KK, KoU, YO and HK conceived and designed the study. KW, YH and HK drafted the protocol of the study. KW, KY, YH, KaU, GN, KK, KoU, YO and HK refined the study protocol and study implementation. All authors have read and approved the final version of the manuscript.
Funding This study is financially supported by AstraZeneca.
Disclaimer AstraZeneca will not be directly involved in the data management, source data verification, or the statistical analysis.
Competing interests KW, KY, YH, KaU, GN, KK and HK have received personal fees from AstraZeneca. KY and GN have received research grants from AstraZeneca.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.