Article Text

Abstract
Introduction Constipation is a common and sometimes debilitating non-motor symptom of Parkinson’s disease (PD) that can result in intestinal inflammation and microbial dysbiosis. The Mediterranean diet, rich in fermentable fibres and anti-inflammatory phenolic compounds, is associated with reduced risk of developing PD and slower progression of parkinsonism. The Mediterranean diet is often recommended for people with PD; however, no studies to date examine this diet as a therapeutic intervention to modulate gastrointestinal (GI) dysfunction.
Methods and analysis This is a randomised, controlled, parallel study. During a 2-week run-in, participants with PD and constipation symptoms (n=52) will undergo baseline nutritional and neurological assessments and provide a stool sample. Participants will be stratified by sex and Hoehn and Yahr stage and randomised to follow standard of care for constipation (control) or standard of care plus a Mediterranean diet (intervention) for 8 weeks. A study dietitian will provide dietary instruction and weekly follow-up via telephone to both groups to support adherence and monitor adverse events. Questionnaires will assess dietary intake and GI function including stool frequency, form, symptoms and laxative usage. Measurements completed at baseline will be repeated at 4 and 8 weeks of the intervention. The primary outcome is to evaluate the difference between mean change (final–baseline) in Gastrointestinal Symptom Rating Scale (GSRS) constipation syndrome scores for the control versus intervention groups. Secondary outcomes will assess stool frequency and form, weekly GSRS syndrome scores, digestive quality of life, laxative usage, faecal microbial communities and inflammatory markers, anxiety, depression, quality life, body weight and composition, dietary fibre intake and Mediterranean diet adherence.
Ethics and dissemination The study has received University of Florida Institutional Review Board-01 approval (IRB202001333). Findings will be disseminated via conference presentations, lectures and peer-reviewed publications.
Trial registration number NCT04683900.
- Parkinson's disease
- nutrition & dietetics
- functional bowel disorders
- immunology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The Mediterranean diet intervention will be compared with standard of care for constipation in Parkinson’s disease.
Sex, age, Hoehn and Yahr stage and levodopa daily dose equivalents will be added to statistical models to control for influence of these variables on secondary outcomes.
The interventions employed are education-based versus controlled-feeding studies and will rely on participant compliance.
The 8-week intervention period and sample size may not be sufficient to observe measurable differences in faecal microbial diversity and inflammatory markers.
Introduction
Non-motor symptoms in Parkinson’s disease (PD), such as constipation, are common and can overshadow motor symptoms in producing morbidity and disability.1 Constipation can impair quality of life and even become debilitating at later stages of the disease.2 3 Though poorly understood, constipation is present in up to 80% of individuals with PD and can precede the onset of motor symptoms.4 Early involvement of the gastrointestinal (GI) tract in PD has led to the hypothesis by Braak et al that alpha-synuclein pathology may originate in the GI tract, as deposition in the GI mucosa has been observed years prior to the onset of motor symptoms in PD.5 Recent models support this hypothesis of a gut-to-brain spread of alpha-synuclein via the vagus nerve as a mechanism for development of PD and that microbiota and inflammation may promote this motor dysfunction.6 7
Constipation is associated with increased intestinal dysbiosis and this may be potentiated due to the interplay with the innate and adaptive immune systems. Such interactions are thought to result in increased intestinal inflammation and leaky gut.8 9 Increased intestinal permeability, microbial dysbiosis, proinflammatory proteins and cytokines (eg, calprotectin, lactoferrin, tumour necrosis factor alpha (TNF-alpha), interleukin (IL)-1, IL-6, IL-8) have all been demonstrated to be increased in vivo or within colonic biopsies and stool samples of people with PD compared with healthy controls.10–15
More recent work has shown decreased abundance of potentially beneficial microbes, such as Prevotella, Faecalibacterium and Roseburia, and increased abundance of Akkermansia and Bilophila to be associated with slow intestinal transit and firmer stools in PD.16 These microbes have been implicated in the regulation of the intestinal barrier,17 inflammation18–20 and even increased motor symptoms in PD based on the Movement Disorder Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS)21; providing additional evidence of the involvement of the microbiota-gut-brain axis in PD.
Therapeutic targets using dietary interventions to improve GI symptoms (eg, constipation) that, in turn, modulate laxation, intestinal inflammation, permeability and microbiota in PD have yet to be explored. Dietary fibres are selectively fermented by intestinal bacteria to produce short-chain fatty acids (SCFA) that are important for improving transit time (which could decrease constipation symptoms), maintaining intestinal barrier function and reducing inflammation.22 In addition, observational evidence suggests associations between Mediterranean diet adherence and lower risk of developing PD (including prodromal symptoms of constipation) as well as slower progression of parkinsonism.23–25
The Mediterranean diet is abundant in fruits, vegetables, whole grains, healthy dietary fats (ie, olive oil, avocados, nuts and seeds), moderate amounts of fish, poultry, eggs and dairy and limited intake from red meats or sweets. Foods within this diet provide energy sources of fermentable fibres and anti-inflammatory polyphenols for intestinal bacteria thought to be beneficial. Higher adherence to the Mediterranean diet has been associated with increased stool frequency and moisture, enrichment in potentially beneficial microbes (eg, Roseburia, Prevotella and Faecalibacterium prausnitzii), increased concentrations of SCFAs, reduced inflammatory biomarkers (eg, IL-1, IL-6, TNF-alpha) and promotion of healthy weight loss.26–31 However, weight reduction is not always desirable in PD, as decreasing body mass index is associated with higher UPDRS scores, increased risk of muscle loss and malnutrition.32 33 While the Mediterranean diet is commonly recommended for people with PD, current evidence supporting its use is primarily observational and not specifically focused on constipation, let alone the risks associated with unintended weight loss.
Therefore, the purpose of this study is to test the efficacy of a Mediterranean diet intervention on improving clinical symptoms of constipation, determine the effect of this intervention on intestinal inflammation and microbial communities and characterise its impact on body weight and composition and muscle function in people with PD.
Methods and analysis
Study design and participant timeline
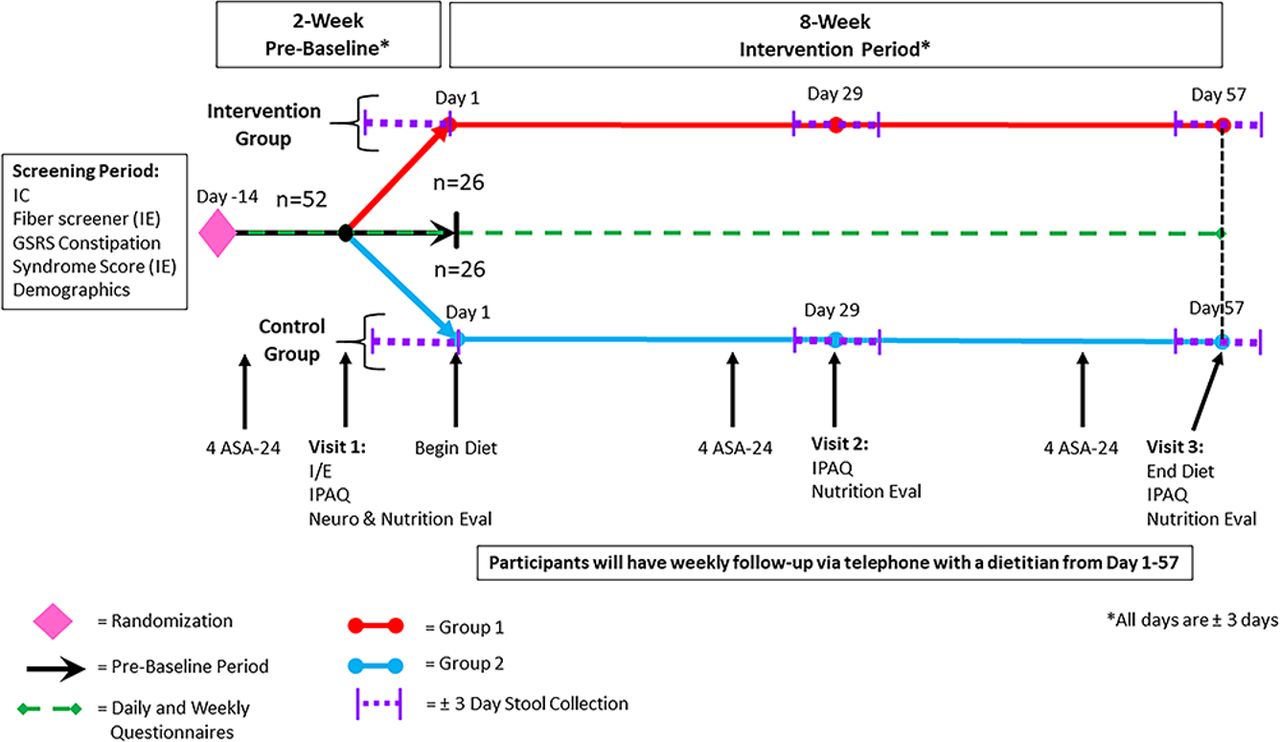
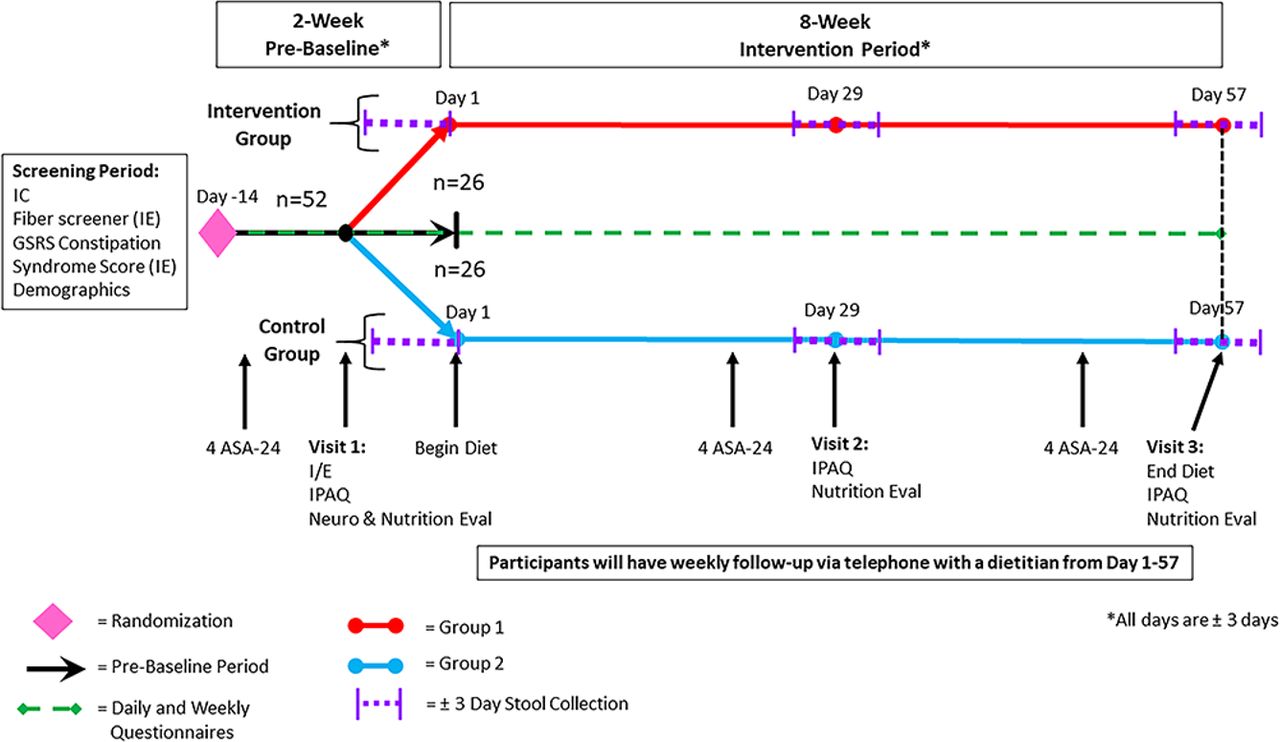
This is a randomised controlled superiority study with two parallel groups that will be conducted at the University of Florida in Gainesville, Florida, USA. After a virtual visit and providing informed consent, a parallel design will be implemented with a 2-week prebaseline period to assess preintervention GI function and an 8-week intervention to compare standard of care for constipation (control group) to standard of care plus a Mediterranean diet (intervention group) (figure 1). During the 2-week prebaseline period, participants (n=52) will begin questionnaires, be instructed to maintain their usual diet and will attend their first study visit (visit 1). Nutritional and neurological evaluations will be conducted at this visit. Participants randomised to the control group will be provided a handout on recommendations for managing constipation symptoms (standard of care). Those randomised to the intervention group will be provided the same constipation handout and counselled on the Mediterranean diet. Following the 2-week prebaseline period, all participants will be asked to begin incorporating the dietary recommendations into their daily routine (day 1). Participants will return to the study site after 4 weeks (visit 2) and 8 weeks (visit 3).
{kind=link}
Study design and participant flow. ASA-24, Automated Self-Administered 24-hour Dietary Assessment Tool; GSRS, Gastrointestinal Symptom Rating Scale; IC, informed consent; IE, inclusion and exclusion criteria; IPAQ, International Physical Activity Questionnaire.
Recruitment
Recruitment will be conducted at the Fixel Institute for Neurological Diseases at the University of Florida via posted flyers, word of mouth and support groups. Local neurology clinics will be mailed flyers about the research study. In addition, people will be identified using an ethics board-approved database at the Fixel Institute. Identified potential participants will then be contacted by study coordinators to invite them to participate in this study.
Informed consent
Potential participants will attend a virtual visit either by telephone or Zoom (Zoom Video Communications, 2019). Prior to this visit, they will be provided a copy of the informed consent form to review. The study coordinator will then review eligibility criteria, consent form and answer questions. Consents will be signed using a secure web application, Research Electronic Data Capture, hosted at the University of Florida.
Eligibility criteria
Inclusion criteria include participants with: (1) neurologist-diagnosed PD aged 40–85 years, (2) drug naïve or on stable dosage of PD medications, (3) Hoehn and Yahr (H&Y) stage ≤2.5 in the clinical ‘ON’ state, (4) constipation syndrome scores ≥2.0 based on the Gastrointestinal Symptom Rating Scale (GSRS),34 (5) consume <20 g of fibre daily based on the Block Fruit/Vegetable/Fiber Screener,35 willing and able to: (6) complete informed consent in English, (7) maintain habitual diet through the prebaseline period, (8) make dietary changes to follow a Mediterranean diet and/or receive standard of care for constipation during the intervention period, (9) complete daily and weekly questionnaires and 12 dietary recalls over approximately 10 weeks, (10) provide stool samples during the collection periods, (11) avoid strenuous exercise and alcohol 24 hours prior to each of the study visits, (12) fast at least 12 hours before each study visit, and (13) discontinue taking prebiotic, herbal or high-dose vitamin or mineral supplements that may impact inflammation throughout the study protocol (not including standard multivitamins or bulk-producing laxatives).
Exclusion criteria include: (1) atypical or secondary parkinsonism, (2) underweight (body mass index <18.5), (3) history of deep brain stimulation surgery, (4) regular use of enemas or suppositories (eg, ≥1 time per week), (5) use of another investigational product within 3 months of the screening visit, (6) antibiotic or probiotic supplement use within 2 months from the day of stool collection, or (7) currently being treated for a physician-diagnosed GI disease or condition (not including constipation, irritable bowel disease, gastroparesis, reflux or diverticular disease).
Study procedures and compliance
One virtual and three in-person visits will be involved (table 1). To ensure compliance and retention, email or text message reminders will be sent to participants for incomplete questionnaires and prior to each study visit. All participants will be followed by study dietitians with weekly phone calls to ensure compliance, improve adherence to the diet and monitor for adverse events.
Schedule of activities per visit
Randomisation
Participants will be randomly assigned to the intervention or control groups (1:1 allocation) via sealed envelopes. Randomisation will be stratified by two groups of H&Y stages (0–1.5 and 2–2.5) and sex (male/female). A member of the department not involved in the study will generate the randomisation envelopes using a random number generator available in Excel (Microsoft). Randomisation will occur in order of consent and when medical records confirming PD diagnosis and H&Y stage are available. Participants will be informed of their assigned group at visit 1 during the prebaseline period. If the H&Y stage is not available from the medical record, then participants will be randomised at visit 1 based on the H&Y stage determined by the study neurologist during the baseline neurological evaluation.
Interventions
Standard of care for constipation management
Participants in both the control and intervention groups will receive a constipation management handout that is distributed to people who present with constipation symptoms at the Fixel Institute. In brief, the handout recommends drinking at least 6–8 cups of fluids daily, as well as increasing physical activity and fibre intake. This handout lists various types of laxative medications (eg, stool softeners, osmotic, bulk producing, etc) and recommendations for usage. Recommendations are in line with current literature for management of constipation in adults.36
Mediterranean diet intervention and guidelines
Participants will receive a 1-week sample meal plan, cookbook, educational handout and counselling by a study dietitian. Guidelines were developed based on the Prevención con Dieta Mediterránea (PREDIMED) trial protocol.37 38 Because our aims are to test the efficacy of this dietary pattern on constipation symptoms in PD, we used the primary Mediterranean diet guidelines outlined in the PREDIMED protocol and did not provide additional supplementation with olive oil or nuts as these are already included in the dietary guidelines. The diet protocol includes the following: (a) abundant use of olive oil for cooking and dressing dishes; (b) consumption of ≥2 daily servings of vegetables; (c) ≥2–3 daily servings of fresh fruits (including natural juices); (d) ≥3 weekly servings of legumes; (e) ≥3 weekly servings of fish or seafood (at least one serving of fatty fish); (f) ≥3 weekly servings of nuts or seeds; (g) select white instead of red meats or processed meats (burgers, sausages); (h) cook at least twice a week with sauce (made of olive oil, tomato, garlic, onion and other aromatic herbs) to dress vegetables, pasta, rice.
Participants assigned to the Mediterranean diet should eliminate or limit the consumption of the following foods: cream, butter, margarine, luncheon meats, carbonated and/or sugared beverages, pastries, commercial bakery products and desserts, French fries or potato chips. Additionally, participants will be asked to exclude consumption from probiotic-containing foods (ie, yoghurt and kefir) due to study exclusion criteria. For usual drinkers, the main source of alcohol should be wine. If wine intake is usual, a recommendation to drink a glass of wine per day (larger volume for men, 150 ml, than for women, 100 ml) during meals is given. Ad libitum consumption is allowed for the following food items: nuts (raw and unsalted), eggs, fish, seafood, low-fat cheese and whole-grain cereals. Limited consumption (≤1 serving per week) is advised for cured ham, red meat (after removing all the visible fat), chocolate (only dark chocolate, with more than 50% cocoa), cured or fatty types of cheese.
Data collection
Daily and weekly questionnaires
Daily questionnaires will assess bowel function (eg, stool frequency and form), medication usage (including laxatives), stress and adverse medical events. Stool form will be assessed using the Bristol Stool Form Scale (BSFS), as this is more strongly correlated with whole gut transit time than stool frequency.39 Weekly questionnaires will assess GI function using the GSRS and Digestion-associated Quality of Life Questionnaire (DQLQ). The GSRS is a validated questionnaire used to assess severity of 15 common GI symptoms grouped into five syndromes including constipation, abdominal pain, reflux, indigestion and diarrhoea.34 Use of this scale will capture a range of GI symptoms within each syndrome. The DQLQ measures the effect of digestive events and experiences on quality of daily life over the past week.
Diet adherence, physical activity and energy intake
Mediterranean diet adherence will be assessed in both groups as part of the weekly questionnaires using the validated 14-item Mediterranean Diet Adherence Screener (MEDAS).40 41 Prior to the three study visits, participants will also complete four 24-hour dietary recalls (two weekdays and two weekends) using the Automated Self-Administered 24-hour (ASA-24) Dietary Assessment Tool, version 2020, developed by the National Cancer Institute (Bethesda, Maryland).42 Both the 14-point MEDAS and ASA-24 will be used to capture all food, nutrient, dietary fibre and energy intake for analyses. Participants will report levels and minutes of physical activity using the International Physical Activity Questionnaire prior to each of the study visits.43
Nutritional evaluation
Participants will be weighed at each study visit. Because weight changes do not specifically characterise fat mass versus fat-free mass versus fluid changes, it is important that dietary interventions evaluate the impact of diet on nutritional status, body composition and how potential changes influence function (eg, grip strength). A study dietitian will measure nutritional status using the Patient-Generated Subjective Global Assessment (PG-SGA) at each visit. The PG-SGA is a questionnaire used to assess prevalence of malnutrition.44 Body composition and hand grip strength will be measured at study visits using bioimpedance spectroscopy (BIS; XiTRON Hydra 4200) and dynamometer (Jamar Plus Digital Hand Dynamometer), respectively. The BIS is a non-invasive device that has been validated to measure total body water, extracellular and intracellular fluid volumes for the calculation of body composition by electrical currents. Participants with an implanted defibrillator, pacemaker, stents or metal suture material in the heart or other vessel will not undergo body composition measurements according to BIS manufacturer guidance. Measurements for the BIS will be taken after a 12-hour fast (no food or drink except water, coffee and decaf tea) and participants will be asked to avoid alcohol and strenuous exercise 24 hours prior to testing. A light breakfast will be provided when measurements requiring a fasted state have been completed. Hand grip strength will be used to characterise muscle function.
Neurological evaluation
At visit 1 a study neurologist will perform a clinical assessment (MDS-UPDRS and Montreal Cognitive Assessment45) to evaluate baseline motor and non-motor symptoms and cognitive function during the clinical ‘ON’ state. The MDS-UPDRS will be completed while fasted to minimise variability of food–medication interactions. Throughout the 10-week protocol, participants will be asked to refrain from PD medication changes, unless necessary. Medication usage, including levodopa equivalents, will be captured on daily questionnaires as a potential covariate if changes occur during the study. At weeks 0, 4 and 8, questionnaires assessing non-motor symptoms will be completed using the Parkinson’s Disease Questionnaire-39 (PDQ-39) to measure quality of life,46 Hamilton Depression Rating Scale (HAM-D) to measure symptoms of depression47 and Hamilton Anxiety Score (HAM-A) to measure symptoms of anxiety.48
Sample collection and analysis
Participants will provide a stool sample at 0, 4 and 8 weeks. Sample collection at week 4 (study midpoint) will allow for a secondary analysis point if participant adherence to the intervention is suboptimal in the second half of the study. Stool samples will be collected using a commode specimen collection system (Biomedical Polymers). Participants will be instructed to portion approximately 1 g of stool sample (size of a kidney bean) into four tubes containing preservative and 3 mm glass beads and vigorously shake. Two samples will be preserved in 3 mL RNAlater (Invitrogen) and the other two samples will be preserved in 3 mL phosphate-buffered saline solution (pH 7.4) with a final concentration of 3% protease-free bovine serum albumin, 0.05% Tween-20 and 1% protease inhibitor (Halt Protease Inhibitor Cocktail, Thermo Fisher Scientific) for microbiota and inflammatory analyses, respectively. Participants will ship the samples overnight to the study site the day of or the following day after collection, and then stored at −80℃ until processing.
Measurements of intestinal permeability and inflammation
Faecal zonulin will be measured as an indicator of intestinal permeability.49 Intestinal inflammation will be assessed by measuring faecal calprotectin.50 Both biomarkers will be measured by ELISA. These inflammatory markers have been observed to be altered with PD and may lead to increased intestinal permeability.14 15
Intestinal microbiota studies
Faecal microbiota studies will be carried out on week 0, 4 and 8 samples using 16S rRNA sequencing to determine changes in alpha diversity (Chao1, Shannon index) and beta diversity (relative microbial operational taxon unit (OTU) abundance and UniFrac). The microbes (ie, F. prausnitzii, Prevotella and Akkermansia, Roseburia, and Bilophila) previously associated with PD-related GI dysfunction will be assessed using quantitative PCR (qPCR). Higher adherence to the Mediterranean diet and its components have been associated with increased microbial richness in part due to increases in Faecalibacterium, Roseburia and Prevotella.27–29 Akkermansia muciniphila, which may be overabundant in PD, is a well-characterised mucin degrader that aides in maintenance of the physiological barrier within the intestine.17 This overabundance of degraded host mucins can increase colonic sulfur production by bacterial cross-feeders, such as Bilophila, and may influence severity of PD symptoms.51
Data management and confidentiality
After informed consent, participants will be assigned a study number for all data collection. Daily, weekly, physical activity, Mediterranean diet adherence and quality of life questionnaires will be administered electronically using Qualtrics Survey Software (SAP Software Solutions). Paper questionnaires will be offered and mailed, when requested. Dietary recalls will be administered electronically by the ASA-24. Participants who are unable to complete the dietary recalls electronically will do so over the phone with a trained study coordinator who will enter the diet recall into ASA-24. Any source data and/or questionnaires completed on paper will be entered into a spreadsheet by at least two study coordinators and data will be compared for quality control. Non-identical entries will be corrected using paper source documents. Auditing of source document completion will be completed after each study visit. Data collected during the trial will be deidentified on study closure. Protected health information concerning study data or participants will not be released to any unauthorised third party.
Safety monitoring
Participants will document any adverse event on their daily questionnaires and follow-up with study dietitians weekly for safety monitoring. Because of the short trial duration and minimal risks associated with participating, there is no outside data monitoring committee. All adverse events will be documented and evaluated by the principal investigator, study dietitians and/or study physicians to determine if the event is a direct result of their participation in the trial. Further, because unintentional weight loss may increase risk for malnutrition, participants will be withdrawn from the study if they have lost >5% of their initial baseline weight at visit 2 and study physicians determine they should not continue.
Sample size calculation
The sample size was calculated based on the GSRS constipation syndrome score. This syndrome score is the mean response for three questions (hard stools, constipation and incomplete evacuation) each scored 1=no discomfort to 7=very severe discomfort. We conducted a 5-week single-arm feasibility study in our centre that demonstrated a mean within participant change (final–baseline) in GSRS constipation syndrome score of 1.13 in participants following a Mediterranean diet who reported constipation symptoms (Rusch C, Beke M and Langkamp-Henken B. Dietary intervention to improve gastrointestinal function in Parkinson’s disease). It is anticipated that in this parallel design there will be a small decrease in mean change in GSRS constipation syndrome scores in the control group influenced by standard of care and weekly contact with the study dietitian. Therefore, a mean difference of 0.7 (eg, representing a decrease in intensity of 1 for each of the three symptoms) for the GSRS constipation score between groups was used for this two-arm, parallel study. A total sample size of 34 (17 per arm) would be required to see a significant (p<0.05, 80% power and 0.99 effect size) difference of at least 0.7 points with an SD of 0.7 between the two groups. To account for a 20% attrition rate, an additional eight participants will be included. An additional 10 participants may be recruited to account for screen failures for a total of 52 participants.
Outcomes
Primary outcome
The primary outcome of this study is to evaluate the difference between mean change (final–baseline) in constipation syndrome scores for the control (standard of care) versus intervention (standard of care+Mediterranean diet) groups.
Secondary outcomes
Secondary outcomes of this study consist of the following: stool frequency (number of weekly bowel movements), stool form (BSFS), weekly syndrome scores from the GSRS, weekly digestive quality of life scores from the DQLQ, laxative usage, qPCR to quantify bacterial species of interest (eg, F. prausnitzii, Prevotella, Roseburia, Bilophila, Akkermansia, etc), faecal microbial abundance and diversity measured by 16S rRNA sequencing analysis, faecal calprotectin and zonulin, PDQ-39, HAM-D and HAM-A scores, body weight and composition, hand grip strength, PG-SGA scores, dietary fibre intake (4-day average) and Mediterranean diet adherence. The trial registry has been updated since its initial posting to reflect the current protocol manuscript secondary outcomes that were recently funded.
Statistical analysis
Intent-to-treat (ITT) analyses will be performed for all outcomes for all eligible participants. Further, last available data/samples from withdrawn participants will be carried forward to week 8 for ITT analyses. Change (final–baseline) in constipation syndrome scores will be analysed using Student’s t-test between groups. Analyses on secondary outcomes will use generalised linear mixed models (SAS Institute, Cary, North Carolina) with intervention group, week and the interaction of group and week as fixed effects with the random effects of subject to account for the repeated measures. Sex, age, H&Y stage and levodopa equivalents will be added to models as covariates as potential explanatory variables. Per-protocol analyses will be performed for all outcomes for participants who score >10 for the intervention group and <10 for the control group based on the MEDAS at 4 and 8 weeks. Data will be reported as means±SEM. A type I error rate cut-off of 0.05 will be used to denote statistical significance.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Discussion
This trial will be the first Mediterranean diet intervention study in PD for management of constipation symptoms. Because there are no therapeutic diets developed to specifically treat the GI symptoms of PD, results of this study will be critically important in confirming the efficacy and safety of this dietary intervention in treating individuals with PD who present with GI dysfunction. Secondary outcomes in this study may help further elucidate mechanisms of how a Mediterranean diet intervention could induce changes in GI inflammation, permeability and microbiota that underlie symptom improvement. Successful outcomes of this trial will provide evidence to (1) promote Mediterranean diet counselling for individuals with PD to treat non-motor symptoms; (2) further investigate long-term adherence of the diet on motor and non-motor functions; and (3) design nutrition recommendations based on the interplay of microbiome, disease and nutritional status (ie, precision nutrition).
Ethics approval and consent to participate
This study has been approved by the Institutional Review Board-01 of the University of Florida (IRB202001333) and registered with ClinicalTrials.gov. Consent to participate will be obtained from all participants prior to the start of the trial by study coordinators. The results of this study will be presented at relevant scientific conferences and peer-reviewed journals.
Protocol amendments
Any modifications to the protocol which may impact study procedures, outcomes and potential risks/benefits to participants will require an amendment to the protocol. All amendments will be agreed upon by study team and approved by the Institutional Review Board-01 of the University of Florida prior to implementation.
Ethics statements
Patient consent for publication
References
Footnotes
Twitter @carleyrusch
Contributors CR, MB and BL-H conceived the study. CR, MB, LT, KD, CNJ and BL-H are responsible for the recruitment, coordination and data collection of participants. CR and MB are dietitians responsible for the diet education and weekly follow-up with participants. TS, TT, AR-Z and CWH are the neurologists responsible for neurological evaluations. CR, CNJ and VM are responsible for stool sample analyses. CR and BL-H are responsible for the statistical analysis. AR-Z and CWH are responsible for medical oversight and safety monitoring. CR drafted the manuscript. All authors read and approved the final manuscript.
Funding This work was supported by the University of Florida and the USDA National Institute of Food and Agriculture, Hatch Project (FLA-FOS-005636).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.