Article Text

Abstract
Introduction Type 2 diabetes is an escalating public health problem closely related to socioeconomic position. There is increased risk of type 2 diabetes in disadvantaged neighbourhoods where education, occupation and income levels are low. Meanwhile, studies show positive health outcomes of participatory community interventions pointing towards the need for increased health promotion and prevention of type 2 diabetes in local communities. This study protocol describes Tingbjerg Changing Diabetes (TCD), a community-based health promotion and type 2 diabetes prevention initiative in Tingbjerg, a disadvantaged neighbourhood in Copenhagen, Denmark.
Methods and analysis TCD is a long-term, complex intervention, implemented in three phases from 2014 to 2032, focusing on partnership formation (phase 1, 2014–2019), developing and implementing action for health (phase 2, 2019–2030) and diffusion of knowledge (phase 3, 2022–2032). The Supersetting principles act as guidelines for development and implementation of all intervention activities of TCD, involving several population groups in a variety of everyday life settings. The implementation of TCD draws on Community Action Research design and methodologies. TCD’s evaluation and research strategy is interdisciplinary, pragmatic and multimethod, unfolding at three levels of operation: (A) evaluating activities, (B) researching cross-cutting topics, and (C) researching methods and approaches.
Ethics and dissemination TCD has been approved by the Danish Data Protection Agency. Accordingly, the initiative is carried out in adherence to rules and regulations of the Danish Data Protection Agency. As data contain no personal identifiable or sensitive data, no clearance from the Danish National Ethical Review Board can be obtained according to Danish regulations. Citizen, local agents and stakeholders are engaged in the design and execution of TCD to ensure usefulness, reflexive interpretation of data, relevance and iterative progression of interventions. Results will be published in international peer-reviewed scientific journals, presented at conferences and through public media including TCD home page, podcasts and videos.
- public health
- diabetes & endocrinology
- education & training (see medical education & training)
- health services administration & management
- qualitative research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- public health
- diabetes & endocrinology
- education & training (see medical education & training)
- health services administration & management
- qualitative research
Strengths and limitations of this study
With its long-term perspective and multidisciplinary approach, Tingbjerg Changing Diabetes (TCD) will provide innovative knowledge and evidence on processes, outcomes and effects of cocreation, intersectoral collaboration and community participation.
With a strong focus on diversity among participating citizens and with distinct efforts to engage citizens in marginalised or vulnerable positions, TCD will develop effective strategies to act on social inequity.
Due to the highly participatory and contextual approach of TCD the initiative is not directly replicable, yet it will develop and test ways of scaling complex interventions through technology transfer of principles, approaches, methodologies and tools.
Background
Social inequality and inequity in health is a major challenge to global public health, not least concerning chronic diseases. Type 2 diabetes is an escalating public health problem in many parts of the world.1 While behavioural factors such as unhealthy diet, limited physical activity, sedentary behaviour, alcohol intake and smoking constitute major risk factors for developing type 2 diabetes,2 ample evidence shows the prevalence of type 2 diabetes to be closely related to socioeconomic position.3 Hence, studies find increased risk of type 2 diabetes in population groups with limited education4 and low occupation and income levels.5
As health is strongly influenced by the social, cultural and environmental contexts of people’s everyday lives,6 7 neighbourhood characteristics also play a significant role to people’s health and risk behaviour8 9 and to long-term health outcomes such as increased risk of obesity and type 2 diabetes.10 Several studies have found that residents of disadvantaged neighbourhoods have higher rates of mortality and morbidity than residents of more affluent neighbourhoods.11–13 In addition, studies have found that cumulative neighbourhood socioeconomic disadvantage is associated with increased incidence of diabetes.14 Furthermore, major demographic and socioeconomic differences have been identified in the prevalence of risk factors and occurrence and in the treatment of diabetes.15
Recalling the Ottawa Charter, stating that health is created in the settings where people spend their everyday lives, it is clear that health promotion and prevention of type 2 diabetes should involve local communities and neighbourhoods and address social equity in health and well-being.6 It has been shown that when using multilevel, multicomponent interventions to address major public health challenges, increased engagement in community interventions has a positive impact on a range of health outcomes16 such as obesity17 and mental health.18 Moreover, evidence indicates that the ‘bottom-up’ approaches and participatory processes that are often applied in community interventions constitute important drivers of collaborative action and social cohesion at community level.19
The Supersetting approach is an intervention strategy for comprehensive community interventions.20 The approach strives to attain synergistic effects through coordinated engagement of multiple stakeholders in multiple settings to mobilise local resources and strengthen social networks for collective community action. Five core principles constitute the Supersetting approach: (1) integration, to ensure that activities are implemented through coordinated action across the boundaries of specific settings, (2) participation, to ensure that people are motivated to take ownership of processes of developing and implementing activities, (3) empowerment, to ensure that people acquire skills and competencies to express and act on their visions and aspirations, (4) context sensitivity, to ensure that everyday life challenges of citizens and professionals are respected and considered when developing and implementing activities, and (5) knowledge generation and sharing, to ensure that scientific knowledge is produced from action and used to inform action (see figure 1).

The Supersetting approach. A set of principles (listed on the left-hand side) guide action among all relevant partners (listed on the right-hand side) within the Supersetting (the circle) to develop sustainable approaches to optimised health, well-being and life quality. The Supersetting is represented as multiple settings within a local community. Activities within individual settings (the inner circles) are coordinated and integrated (symbolised by the lines) with activities in other settings as the basis for achieving synergistic effects.
The Supersetting approach has been successfully implemented in the research-based intervention project Health and Local Community that was carried out in various communities in Denmark from 2012 to 2015.21 This project aimed at promoting healthy living among children and their families and it demonstrated that the Supersetting approach can deliver sustained structural and behavioural outcomes.22 23 While the Supersetting approach proved to be successful in relatively homogeneous and socially cohesive local communities, the approach has not been applied in socially and ethnically diverse neighbourhoods.
Nevertheless, by emphasising context sensitivity and intersectoral coordinated action based on citizen participation, the Supersetting approach holds great potential as a strategy for community-based health promotion and type 2 diabetes prevention in socially, culturally and ethnically diverse neighbourhoods. Reviews on community engagement, recruitment and participation of vulnerable people find that power sharing and collaborative partnerships24 as well as extended time frames, acknowledgement of higher resourcing costs and long-term partnership operation are key elements to engagement and participation.25–27 However, while consensus exists that intersectoral collaborative action is a beneficial and cost-effective strategy in health promotion,28 we still lack knowledge on processes and methodologies of sustainable intersectoral collaboration and action among professional practitioners within the local community.
Tingbjerg Changing Diabetes (TCD) is a long-term community-based initiative that applies the Supersetting approach. The aim of TCD is to promote health and prevent type 2 diabetes among high-risk population groups living in Tingbjerg, a disadvantaged neighbourhood in Copenhagen, Denmark. TCD constitutes a strategic, organisational and locational framework for developing, implementing, evaluating and improving a variety of research-based interventions, projects and activities in a local community together with citizens, professional practitioners, researchers and decision-makers in public institutions, private enterprises and civic organisations. While TCD builds on the conceptual framework of the previously mentioned project Health and Local Community, the initiative has new ambitions emphasising new target groups (ethnically and socially diverse), new contexts (significant socioeconomic challenges), a new location (socially disadvantaged urban neighbourhood) and an additional focus (technology transfer).
Following the principles of the Supersetting approach, TCD includes multiple coordinated interventions driven by multiple intersectoral stakeholders and participants in multiple local community settings. TCD addresses the contextual social challenges of people’s everyday lives in efforts to empower them to act for better health and well-being for themselves, their families and their community. In this way, it is fundamental to the intervention to both identify and mobilise community assets and resources to support health and well-being among people and in their community with the aim of increasing their control over their health and their community.29 30 Furthermore, the ambition of TCD goes beyond local health promotion and diabetes prevention as the strategic intervention aims to test and study the transferability of the Supersetting principles, concepts and methodologies to other city contexts, communities and neighbourhoods.
The purpose of this protocol is to describe and unfold the intervention and research agendas of the TCD initiative, including the design, strategy, concepts and methodologies.
Methods/design
Aims and objectives
The overall aim of TCD is to promote health and prevent diabetes among high-risk population groups living in the neighbourhood Tingbjerg. The initiative is designed as a long-term, complex intervention that is developed and implemented in three interconnected phases from 2014 to 2032 (see figure 2).

Phases of Tingbjerg Changing Diabetes. Each of the three phases has a development side and a research side, both of which are described in the ‘Implementation of TCD’ section. Phase 1 relates to the formation of interventions; phase 2 relates to the implementation of interventions; phase 3 relates to the diffusion of interventions. TCD, Tingbjerg Changing Diabetes.
The first phase, focusing on formation, covered processes of conducting contextual analyses and establishing relationships with diverse stakeholders in Tingbjerg. The second phase, focusing on action, covers iterative processes of developing, implementing, evaluating and improving activities. The third phase, focusing on diffusion, includes the transfer of technologies that are developed, applied, studied and found effective to support intervention processes of TCD (see section on implementation of TCD for elaborations of the three phases). Accordingly, the specific objectives of the initiative are as follows:
To facilitate sustainable intersectoral collaboration and partnerships among relevant public institutions, private enterprises and civil society organisations engaged in social development and health promotion in Tingbjerg.
To cocreate community-based projects and initiatives together with residents of the neighbourhood.
To transfer evidence-based knowledge, principles and methodologies in order to carry out and evaluate complex community-based health promotion interventions in other city contexts.
The local community and its residents
TCD is implemented in the public housing area of Tingbjerg, 8 km north of Copenhagen city centre. The neighbourhood has a population size of approximately 6600 residents living in 2500 apartments and is one of the biggest public housing areas in Denmark. Tingbjerg is characterised by high ethnic diversity with more than 80 nationalities contributing to a wealth of cultures, languages and traditions. In 2017, 80% of the residents comprised immigrants or descendants of immigrants compared with 24% for the city of Copenhagen.
Tingbjerg is considered a disadvantaged neighbourhood and appears on a so-called ‘ghetto list’ introduced by the Danish government in 2010. Criteria for being listed as a ‘ghetto’ relate to population size, employment rate, education and income levels, crime rate and proportion of residents with an immigrant background. Substantial efforts to address the social challenges of Tingbjerg have been initiated over the past few decades. These have included the implementation of comprehensive social development plans jointly funded by the National Building Foundation and the Municipality of Copenhagen.
Tingbjerg has a high prevalence of type 2 diabetes and other chronic diseases compared with other areas of Copenhagen, making the area a prime target site for interventions on diabetes prevention. In 2015, a register-based assessment of diabetes risk factors in Copenhagen found major socioeconomic and geographic differences in the prevalence of risk factors in Copenhagen.15 Citizens with lower levels of education had twice the prevalence of high-risk scores compared with more highly educated citizens. Unemployed citizens had 40%–80% higher rates than employed citizens. Among the 10 districts in Copenhagen, risk scores were the highest among those living in Brønshøj-Husum, including Tingbjerg, which is the most disadvantaged neighbourhood in the district.31 A register-based investigation conducted by Steno Diabetes Center Copenhagen (SDCC) in 2020 showed that one-tenth (9.5%) of adult residents in Tingbjerg had a diagnosis with either type 1 diabetes (0.4%) or type 2 diabetes (9.1%) by the end of 2018 (data not published). These prevalence rates are significantly higher compared with Copenhagen at large, where the prevalence was approximately 5% for type 1 and type 2 diabetes combined.
TCD targets all residents of Tingbjerg, but pays specific attention to children, youth and families. Early intervention is crucial in the efforts to prevent type 2 diabetes as risk factors begin to accumulate in early life and continue across the entire life course.32 33 Furthermore, engaging families as a social setting for health constitutes an important strategy in efforts to situate interventions in the context of everyday life.34
Organisation of TCD
TCD is organised around a Coordination Group of partners based in Tingbjerg, providing administrative, logistical and practical support to community-based stakeholders involved in processes of defining, planning and implementing activities and projects in Tingbjerg. The Coordination Group closely interacts with a Research Group of research partners to exchange ideas, coordinate actions and optimise data collection and knowledge management processes. The Coordination Group is directed by a Steering Committee of decision-makers from key partner institutions. The Research Group is directed by a principal investigator who also sits on the Steering Committee. The number of people represented in each of these groups and committees varies over time in accordance with the dynamics of the partnership.
By the end of phase 1, involved partners included: Brønshøj-Husum District Political Committee; Copenhagen Hospitality College; Copenhagen Municipality (departments of culture, health, employment and social services); Danish Society for Nature Conservation; Gerlev Center for Play and Movement; Madkulturen (a self-governing food institution); Social Housing Associations of FSB and KAB; SDCC; Svanholm Gods (an organic production farm); University of Aalborg; University of Copenhagen; University of Southern Denmark.
Development and implementation of TCD
TCD applies the Supersetting approach, involving the coordinated engagement of multiple stakeholders in multiple settings to mobilise local resources and strengthen social networks for community action.20 The five principles of integration, participation, empowerment, context sensitivity and knowledge act as overarching guidelines for the development and implementation of all intervention projects and activities of TCD. Accordingly, the intervention components are multistranded, involve several population groups and include a variety of everyday life settings used by Tingbjerg residents. The specific projects and activities of the intervention are developed in collaborative processes, which are based on local priorities and needs for action, engagement of formal institutions, organisations and associations, and the involvement of informal social networks of citizens, for example, children, mothers and elders. Cross-sectoral stakeholder engagement, collaboration, coproduction and cocreation are key elements that support this integrated approach for optimal and long-lasting results, spillover effects and high levels of community and citizen engagement.
The implementation of TCD is operationalised by a Community Action Research (CAR) process design. CAR is an iterative development process that combines reflection and analysis with action in local communities. With an origin in action research and participatory action research,35 CAR is a highly participatory approach used to engage citizens, professional practitioners and researchers in joint efforts to develop, implement, evaluate and improve community interventions in accordance with the six steps of the CAR cycle (see figure 3).

The six-step cycle of Community Action Research (CAR) for sustainable interventions in local community settings. Each step is repeated iteratively to constantly evaluate and improve actions. Tingbjerg Changing Diabetes (TCD) applies the CAR processes in two ways: (1) to guide each project through a process of fulfilling the six steps, and (2) to drive and guide the TCD initiative in the long term (step 1+2 refers to phase 1, step 3+4 refers to phase 2, step 5+6 refers to phase 3).
Step 1: jointly analysing the problem and local context
This step involves citizens and professional practitioners in structured processes of gathering context-specific knowledge about the local community, including community-defined priorities, aspirations and challenges for social and healthy living. The Local Community Analysis tool has been developed and used by our researchers for this purpose.36 The Research Group facilitates and supervises these processes. Involving the local community in joint analysis secures high relevance of the analysed contextual determinants but may challenge the objectivity and validity of the findings due to limited neutrality, anonymity and impartiality of both data collectors and informers living in the local community.
Step 2: establishing the partnership and working relationships
This step involves identifying key partners to engage in a formalised partnership around the initiative. In addition, this step mobilises relevant community-based stakeholders representing public institutions, civic organisations and/or private enterprises to play active roles in concrete projects and activities. It includes discussing and negotiating the terms of engagement with partners and professional practitioners, and agreeing on the goals, values, concepts and principles of the initiative. The Coordination Group and the Research Group jointly facilitate these processes. Involving partners and stakeholders in formalised alliances in this step enables the establishment of a common framework and shared commitment based on jointly identified topics of collaboration but may complicate consensus building and decision-making in situations where policies, priorities and obligations markedly differ.
Step 3: jointly developing and planning interventions
This step involves citizens and professional practitioners in structured processes of identifying specific interests and ideas for change within the context of previously defined topics. It also includes jointly developing them into concrete interventions and activities such as community-based events and projects as well as planning their implementation and coordination, including practical, logistical, legal, ethical, financial and time-related aspects. These processes may apply the Future Workshop approach37 adapted to the characteristics of the target group and the specific purpose of the exercise.38 The Coordination Group provides administrative and practical support to the planning process and the Research Group facilitates the workshops. Involving the local community in this step empowers citizens to become dedicated agents of change and enhances the relevance of locally defined goals and strategies for action but may complicate consensus building and decision-making about community health priorities due to diverse interests among different population groups in the local community. It may also challenge the quality and efficiency of action planning processes in communities where planning skills and competences are weak.
Step 4: jointly implementing interventions
This step involves citizens and professional practitioners in structured processes of organising and implementing interventions in accordance with the implementation plan. It includes the mobilisation of resources embedded in the local community such as manpower, consumables, materials, equipment and physical space. The Coordination Group provides administrative and technical support to the action process. Involving the local community in this step fosters long-term commitment among citizens to engage in social and health interventions but may challenge implementation efficiency and jeopardise outcomes in situations where action is heavily dependent on citizens with limited or fluctuating social or mental capacity.
Step 5: jointly monitoring and evaluating interventions
This step involves citizens and professional practitioners in structured processes of evaluating interventions and their impacts based on interdisciplinary scientific methodology. It includes the training of stakeholders in research methodology such as survey design and data management. It also includes close supervision of trained stakeholders conducting field work. The Research Group facilitates and supervises these processes. Involving the local community in this step provides meaningful and relevant assessments based on data that are generated and owned by the community but may challenge the validity of the findings in situations where major compromises are made between stakeholder interests and scientific traditions.
Step 6: jointly adjusting, anchoring or scaling interventions
This step involves citizens and professional practitioners in structured processes of adjusting and anchoring interventions based on preceding evaluations and assessments. It includes facilitated meetings between involved stakeholders at which suggestions, ideas and arguments for change and sustainability are presented and discussed. Ideas for new interventions may emerge and unfold. Moreover, potential scaling of the interventions can be initiated. The Coordination Group and the Research Group jointly facilitate and support these processes. Involving the local community in this step optimises implementation processes and promotes sustainability of the intervention but may challenge the sustained motivation and engagement of citizens due to their many obligations in everyday life.
The CAR cycle guides the development, implementation, evaluation and adjustments of the projects and activities that are implemented in Tingbjerg. Proper participatory methods and approaches are needed in all steps of the cycle in order to optimise relevance and promote local ownership of activities. Moreover, the CAR process emphasises contextual reflexivity and cultural responsiveness to safeguard the application of appropriate methods that are sensitive to the high diversity of participants concerning age, gender, ethnicity and socioeconomic status.
Implementation of TCD in three phases
TCD is implemented in three interconnected phases of formation, action and diffusion (see figure 2). In accordance with the CAR principles, all activities of TCD are developed iteratively within and across each of these phases.
Phase 1: formation (2014–2019)
This phase covered processes of conducting contextual analyses and establishing relationships with diverse stakeholders in Tingbjerg for the purpose of preparing for action. Since 2014, we have conducted a variety of investigations in Tingbjerg, including mapping the physical infrastructure, describing organisations and social networks, analysing the socioeconomy of the community and documenting health and behavioural determinants and risk factors for diabetes and other chronic diseases. Specific analyses carried out include studies that have (1) analysed the use of healthcare services among socially vulnerable people with diabetes in Copenhagen using a vulnerability assessment framework;39 (2) mapped diabetes risk, diagnosis and treatment, identifying vulnerable population groups in Copenhagen using the epidemiological rule of halves framework;15 (3) described the social and organisational environments in Copenhagen, including community resources, social networks and people’s willingness to provide social support across gender, age and cultural affiliation;40 (4) analysed demographic, socioeconomic and behavioural factors among residents in Tingbjerg using a population-based survey approach as well as data from public registers (unpublished).
Furthermore, we have explored and established collaborative arrangements and partnerships with numerous stakeholders working in Tingbjerg with health promotion, social development, housing, education, employment, environment, day care, culture, leisure, agriculture, food and physical activity. Substantial amounts of resources have been invested in establishing this knowledge-based foundation for engaging with professional practitioners and citizens in the local community. Finally, a physical setting with combined indoor and outdoor facilities has been established in the heart of Tingbjerg. We call it the Tingbjerg Community Hub and it functions as a focal point for cocreating activities and social arrangements together with residents of the neighbourhood. Although the preparatory work has been completed and a proper foundation for community engagement has been established, the documentation of community contexts continues because of the ever-changing characteristics of populations, organisations and infrastructures.
Phase 2: action (2019–2030)
This phase builds on knowledge and relationships established in phase 1 and covers iterative processes of developing, implementing, evaluating and improving activities in Tingbjerg. Some of these are single-standing events and social arrangements whereas others are long-term projects requiring intensive planning and mobilisation of resources. They follow the six steps of the CAR cycle and involve academic partners, professional practitioners and citizens living in Tingbjerg. All activities and projects implemented in TCD combine civic learning and action for the good of the community and its citizens. TCD thus engages with professional practitioners and citizens through equitable partnerships based on long-term commitments of cocreation and colearning. Some of the more comprehensive intervention projects that have been or are in the process of being implemented by TCD are described below.41
Project Tingbjerg Social Garden
Located in Tingbjerg Community Hub, this project is a melting pot for citizens to develop ideas and receive practical and technical support to establish social gardening activities and projects spanning from vegetable and herbal farming in raised beds to beekeeping and poultry keeping or income-generating production of soft drinks based on herbal extracts.
Project Family Cooking Classes
Based on an expressed desire among families with children to learn about and perform healthy cooking, this project implements a series of cooking classes where parents and children receive training inspired by Benn’s food literacy model emphasising knowing (about food, nutrition and health), doing (practical and technical competences), sensing (sensory competences and food courage), wanting (participating and acting) and being (caring for and of others and the environment) regarding food issues.42 The process of developing and implementing cooking classes mobilises families and contributes knowledge on how to engage the home as a setting for health promotion.43
Project Organic Farm Cooperation
To evoke the consciousness of identity and culture among the many families in Tingbjerg who originate from rural communities in the Middle East and Northern Africa this project strengthens the rural–urban cooperation of TCD by inviting citizens to participate in farming activities of the organic production farm of Svanholm Gods located about 40 km northwest of Tingbjerg. In return, participants receive farming products such as vegetables, meat and eggs for their own consumption. Svanholm Gods also provides technical expertise and farming products to other TCD projects.
Project Community Restaurant
Inspired by diverse world cuisine cooking competences among the citizens of Tingbjerg, this project includes the establishment and running of a community restaurant in which citizens are supervised by a professional chef while organising, preparing and serving cheap and healthy three-course dinners served to fellow citizens once every week. Some ingredients are home grown, some are from the local store, while others are brought in from the organic production farm of Svanholm Gods.
Project Communities of Volunteers
Whereas community and voluntarism are key ingredients and catalysators in all TCD projects this project is designed explicitly to embrace citizens with whatever social and cognitive resources they possess and invite them to take part in different subprojects such as animal husbandry and carpentry and dressmaker workshops. To this end, TCD has developed two models (the model of participation and the model of voluntarism) to be used and tested to attract and retain citizens across a wide gradient of socioeconomic capacity.
Project Integrated Diabetes Intervention
The project is based on a holistic approach in which diabetes prevention, detection and treatment is integrated and coordinated within local community settings, and in which citizens living with diabetes are empowered and offered support to navigate the healthcare system. The project consists of three inter-related intervention components: (1) prevention and health promotion, (2) early and active detection of diabetes, and (3) complication screening and treatment.
Phase 3: diffusion (2022–2032)
This phase includes the promotion and reinforcement of the systemic uptake and transfer of technologies that are developed, applied, studied and found effective to support intervention processes of TCD. These technologies include approaches, concepts, values, principles, methodologies and tools. The uptake of technologies in established organisational structures strongly promotes their sustained use in the local community. This may be endorsed by decision-makers provided that the practicability, benefits and cost-effectiveness of interventions are properly documented and communicated. TCD continually optimises its technologies and documents their improvements while promoting their uptake in relevant public, private and civic organisations. In addition, the transfer of these technologies to new community and city contexts strongly promotes their wider use. This implies setting up new initiatives in new locations with new partners, stakeholders, settings, population groups, interventions and activities. In Denmark, setting up such new initiatives has been going on for years, either as long-term and full-scale partnership initiatives such as the Our Healthy Community project,44 or as minor and more focused collaborative projects in which our technologies are applied in processes of facilitating and supervising local community analyses, cocreation processes, etc. Internationally, the transfer of technologies is currently in the early planning phase and will be carried out within the framework of the global Cities Changing Diabetes programme,45 to which TCD is closely connected. This is expected to be the prime action arena for collaboration and technology transfer in the coming decade.
The Meta Theory of TCD
TCD builds on an overall change theory that we refer to as a Meta Theory. While individual projects and activities in TCD make use of theories of change to support project planning, implementation and assessment, the TCD Meta Theory represents theoretical and empirically grounded knowledge about how change occurs across multiple projects.46 The Meta Theory informs the theory of change of each project, thereby enhancing synergy between projects and ensuring consistency and shared visions and goals of a comprehensive and long-term intervention strategy (see figure 4).
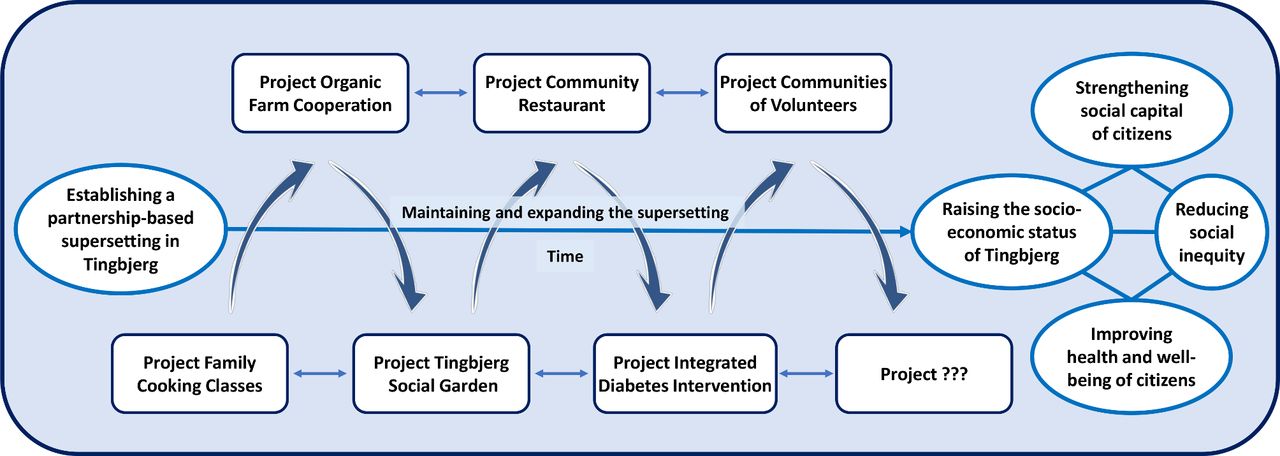
Meta Theory of Tingbjerg Changing Diabetes. The core component is the partnership-based Supersetting in Tingbjerg. This is established, maintained and expanded over time and fuelled by distinctive but interconnected projects to accumulate effects at individual, population and societal levels on social capital, socioeconomic status, health, well-being and inequity.
The Meta Theory is highly complex, involving several projects that are coordinated and implemented by a dynamic and ever-changing partnership of public, private, civic and academic partners. The partnership cocreates and codevelops distinctive but interconnected projects, and accumulates their effects at individual, population and societal levels on social capital, socioeconomic status, health, well-being and inequity.
The principles of the Supersetting approach constitute core drivers of the Meta Theory and a key to its success is partnership and project synergy. Trust has previously been identified as a crucial predictor of successful partnership synergy.47 Accordingly, a main driver of the Meta Theory is trust building among stakeholders and citizens as a foundation for establishing, maintaining and expanding the Supersetting over time. Synergy is produced by building partnerships across projects. For example, project Tingbjerg Community Restaurant was developed through synergistic effects by drawing on experiences and relations established during the implementation of project Family Cooking Classes, where Copenhagen Hospitality College is a main partner, and project Organic Farming Cooperation, where Svanholm Gods is a main partner. Furthermore, synergy occurs across projects when participants define new ideas and engage in new initiatives in the Supersetting. It is the mutual influences of people and their ideas that sustain action and accelerate change processes.
Evaluation and research strategy
TCD has defined an interdisciplinary evaluation and research strategy. Due to the high complexity of multiple iterative evolving components, the evaluation approach of TCD is pragmatic. Accordingly, the evaluation is guided by epistemological flexibility, methodological comprehensiveness and operational practicality.48 The evaluation and research unfold at three different levels of operation (see figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Evaluation and research strategy of Tingbjerg Changing Diabetes. Includes evaluation and research implementation at three levels of operation (A, B, C) and a variety of research topics for each of these levels.
Level A. Evaluating specific projects
TCD implements a variety of projects, each of which strives to fulfil the same overall objective of the initiative. The specific activities of the projects are extremely diverse, and each project therefore requires its own evaluation and research agenda. The evaluation agenda serves to satisfy the needs of the partnership to provide direction and adjust the projects. It may therefore be considered an internal agenda. Evaluation processes adhere to the principles of theory-based Realist Evaluation,49 mainly addressing the same process-related research questions of what works, for whom, in what circumstances and why? Efforts are also made to assess the extent to which the principles of the Supersetting approach are addressed by the projects and how they affect their processes and outcomes. This is done using Principles-Focused Evaluation.50 The research agenda serves to satisfy academic interests in selected project-specific topics. Such topics are, for example, investigated qualitatively through context-mechanism-outcome (CMO) configurations within a project-specific programme theory or assessments by external (non-participant) researchers of the characteristics of certain participatory action research processes.
Level B. Researching cross-cutting topics
TCD implements research on selected topics that cut across projects of the initiative. Gathering data across projects to address the same research question enriches the analytical process and its findings. There are currently four such cross-cutting topics in TCD: (1) community and social capital, (2) education, occupation and entrepreneurship, (3) health, food and physical literacy, and (4) health economy and social investment. These topics are all complemented by specific research questions that are answered using qualitative and quantitative research methods. Specific research questions for each of these topics are presented in table 1 and research methods are presented in table 2. The strategic and organisational framework of TCD, whereby several projects are implemented simultaneously and in a coordinated manner within the same local community, provides ideal conditions for undertaking this kind of cross-cutting research; including research on synergies and positive spillover effects in multicomponent health promotional interventions.
Research questions of TCD
Research methods of TCD
Level C. Researching methods and approaches
TCD researches methods and approaches related to each of the three implementation phases of the initiative: formation, action and diffusion. Specific research topics have been carefully selected based on an overall aim to contribute with research-based knowledge and evidence to the development, refinement and application of applied concepts, principles, approaches, methodologies and tools that may be adopted by public, private and civic stakeholders in other community and city contexts around the world. The specific research focus of the formation phase (phase 1) is partnership dynamics. This includes longitudinal research on partnership formation and development processes, structures and functions but also on more fundamental issues concerning how to understand the concept of partnership in complex and ever-changing community contexts. The specific research focus of the action phase (phase 2) is the Supersetting approach. This includes operational research on the Supersetting approach and its five principles as well as methodological research on the application of Principles-Focused Evaluation methodology and its complementarity to Realist Evaluation methodology for evaluating complex interventions. The specific research focus of the diffusion phase (phase 3) is technology transfer. This includes implementation research on processes of scaling interventions and transferring approaches, concepts, principles, methodologies and tools from one context to another. These topics are all accompanied by specific research questions that are answered using qualitative or quantitative research methods, or a mix of the two. Specific research questions for each of the three implementation phases of TCD are presented in tables 1 and 2.
Patient and public involvement
It is a commonly known challenge that people living in disadvantaged neighbourhoods are less likely to participate in health interventions compared with people living in more affluent neighbourhoods.25 51 Nevertheless, it remains key to TCD to engage citizens and multiple local stakeholders through equitable partnerships based on long-term commitments of cocreation and colearning to effectively ensure sustainable solutions, ownership in the local community and reduce disparities in health.52 53 Thus, drawing on extensive evidence emphasising how community-based research and action requires time and enduring commitments,35 40 54 TCD meets the challenge of participation with a long-term design, emphasising sustainable partnership and trust building among local stakeholders and residents. Hence, paying specific attention to ensuring diversity among participating citizens and with distinct efforts to engage marginalised and vulnerable groups of citizens, TCD contributes to the development of effective strategies to access, engage and retain participants from disadvantaged neighbourhoods. Accordingly, public involvement is applied in all steps of TCD.
TCD is based on collaboration and action across sectors. This is compatible with the recommendations of the Commission on Social Determinants of Health6 and implies that integrated action is accomplished through voluntary agreements and a willingness to work together with partners from different sectors such as health and care, education, occupation, housing, environment, culture and social support.55 Partnerships across sectors involving multiple stakeholders are needed to address the underlying causes of the social determinants of health and to address health disparities.28 However, consistent theoretical and methodological frameworks for successful intersectoral action remain scarce56–58 and more comparative studies and interdisciplinary research are therefore needed.59 60 TCD contributes by addressing this knowledge gap.
Ethics and dissemination
TCD adheres to all Danish ethical standards of participant information, consent, confidentiality and data handling. Written informed consent will be obtained from all participants in research activities. TCD has been approved by the Danish Data Protection Agency (journal number: P-2019-222). Accordingly, the initiative is carried out in adherence to rules and regulations of the Danish Data Protection Agency. Information on confidentiality and voluntarism is given to all study participants. As data contain no personal identifiable or sensitive data, no clearance from the Danish National Ethical Review Board can be obtained according to Danish regulations.
Results will be published in international peer-reviewed scientific journals and presented at conferences, seminars and as short reports. Also, ongoing dissemination to and with citizens and local agents, in workshops, through videos and podcasts, at the TCD web site41 and through social media is a key element throughout the initiative. TCD has a strong focus on investigating processes, methodologies and outcomes across and within projects through in-depth investigations of particular CMO configurations, partnership dynamics, principle adherence and subjective outcomes, and with an ambition to develop and test objective measures and indicators to evaluate and assess outcomes of participatory health promotion and diabetes prevention. With its long-term perspective of more than 15 years, and a solid multidisciplinary approach and research alliances, TCD is in a strong position to provide innovative knowledge and evidence on processes, outcomes and effects of cocreation, intersectoral collaboration and community participation.
Ethics statements
Patient consent for publication
Acknowledgments
TCD is a partnership initiative and the development and implementation of activities, ideas and concepts cannot take place without the commitment and hard work of all partners and citizens involved.
References
Footnotes
Contributors Intervention design: MKT, PTA, AVN, MP, TT, HV-N, AV, PB. Conceptualisation: MKT, PTA, AVN, MP, TT, HV-N, AV, PB. Methodology: MKT, PTA, AVN, MP, TT, HV-N, AV, PB. Implementation, evaluation and research: MKT, PTA, AVN, MP, TT, HV-N, AV, PB. Writing—original draft preparation: MKT, PB. Writing—review and editing: MKT, PTA, AVN, MP, TT, HV-N, AV, PB. Project administration and funding acquisition: PB. All authors have read and agreed to the published version of the manuscript. Corresponding author: MKT.
Funding TCD receives financial support from the Novo Nordisk Foundation (reference number: 0052046).
Disclaimer The foundation has no role in study design, data collection, analysis or process of publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.