Article Text

Abstract
Objectives Purposefully designed and validated screening, triage, and severity scoring tools are needed to reduce mortality of COVID-19 in low-resource settings (LRS). This review aimed to identify currently proposed and/or implemented methods of screening, triaging, and severity scoring of patients with suspected COVID-19 on initial presentation to the healthcare system and to evaluate the utility of these tools in LRS.
Design A scoping review was conducted to identify studies describing acute screening, triage, and severity scoring of patients with suspected COVID-19 published between 12 December 2019 and 1 April 2021. Extracted information included clinical features, use of laboratory and imaging studies, and relevant tool validation data.
Participant The initial search strategy yielded 15 232 articles; 124 met inclusion criteria.
Results Most studies were from China (n=41, 33.1%) or the United States (n=23, 18.5%). In total, 57 screening, 23 triage, and 54 severity scoring tools were described. A total of 51 tools−31 screening, 5 triage, and 15 severity scoring—were identified as feasible for use in LRS. A total of 37 studies provided validation data: 4 prospective and 33 retrospective, with none from low-income and lower middle-income countries.
Conclusions This study identified a number of screening, triage, and severity scoring tools implemented and proposed for patients with suspected COVID-19. No tools were specifically designed and validated in LRS. Tools specific to resource limited contexts is crucial to reducing mortality in the current pandemic.
- infection control
- accident & emergency medicine
- public health
- COVID-19
Data availability statement
The full dataset is available on reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We provide the first review of COVID-19 screening, triage, and severity scoring tools both proposed and implemented among initial patient presentations to the healthcare system.
Many screening, triage, and severity scoring tools have been proposed and implemented, but none are specific to low-resource settings (LRS).
We identified 51 tools—31 screening, 5 triage, and 15 severity scoring—that have variables feasible for collection in LRS.
Feasibility, however, does not predict that a tool will be accurate or effective, and no tools from this review were validated in LRS.
It is likely that many tools being used in healthcare systems worldwide are not published and thus cannot be described in this review.
Introduction
SARS-CoV-2 was declared a global public health emergency on 30 January 2020.1 In the time since, more than 153 million people have been infected and over 3.2 million have died.2 While many low-income and middle-income countries (LMICs) were relatively spared from high mortality rates, public health measures to contain the virus have put enormous strains on health systems and the ability of countries to care for existing disease burdens.3–5 The influx of patients with COVID-19 stressed healthcare systems worldwide by increasing demand for personal protective equipment (PPE), diagnostics, oxygen and mechanical ventilators.6 Low-resource settings (LRS) have limited access to these resources and remain disproportionately challenged during the COVID-19 pandemic.7 8 Even in regions where viral transmission remains low, patients with suspected COVID-19 require precautions, and confirmed cases require costly treatment and care. As the pandemic endures, continued resource demands have the potential to overwhelm LRS healthcare systems.3
Early recognition and treatment of acute conditions are integral to reducing general mortality in LRS.9 Previous evidence suggests three specific processes—screening, triage, and severity scoring of patients—improve patient outcomes in LRS.10 11 These practises reduce resource utilisation across a variety of settings and inform ongoing patient management,12 but appropriate implementation during public health emergencies can be challenging. The need for screening, triage, and severity scoring tools in real time may lead to the use of both unvalidated and potentially ineffective protocols.
Although emergency care has developed rapidly in LMICs over the past two decades, it remains undeveloped in many regions, particularly outside of urban areas.13 Many healthcare systems lack formal emergency units (EUs), and those with dedicated spaces for emergency and acute care may not routinely screen or triage patients. Implementing these tools can be challenging in LRS, where equipment, staff and systems are lacking.7 Despite the limitations, the exceptional risks of COVID-19 have placed screening and triage procedures at the forefront: practical screening and triage protocols maximise use of limited available resources and keep patients and providers safe.
Screening refers to the process of identifying and isolating patients with COVID-19 risk factors on initial presentation to the healthcare system, such as to outpatient clinics and EUs.9 It is a rapid process to evaluate potential risk of infection, typically using basic clinical and historical information. In order to be successful, it must be based on easily understood case definitions, as it is frequently performed by non-healthcare personnel (such as security guards). With screening, high sensitivity is typically prioritised over specificity, so that all cases are identified. This process is fundamentally different from diagnostic testing, which is also referred to as screening in some literature. Triage—a systematic method of sorting patients into priority groups based on the severity of their clinical syndrome, and matching these groups with available resources–is usually conducted following screening.14 Triage is seen as a fundamental component of effective emergency care15: in order for triage to improve patient outcomes, the triage protocol must effectively prioritise the sickest patients for emergency interventions and direct patients to the appropriate levels of care.16 Severity scoring stratifies patients with a diagnosis (eg, confirmed or suspected COVID-19) based on risk of poor outcomes, such as mortality or admission to the intensive care unit, and can complement the triage process and further inform resource allocation.
To date, there have been no published reviews detailing available tools for identification and triage of patients with COVID-19. This review aimed to identify currently proposed and/or implemented methods of screening, triaging, and early severity scoring of patients with suspected COVID-19 on initial presentation to the healthcare system and to evaluate the utility of these tools in LRS.
Methods
Search strategy
A systematic search was conducted to identify literature describing screening, triage, and severity scoring practices that have been implemented or proposed for use with patients with suspected COVID-19 on first presentation to emergency or acute care settings.
Four electronic databases (Embase, Ovid/Medline, PubMed and Web of Science) were searched using keywords, with adaptations made based on controlled vocabulary standards for each database. Initial search terms included “COVID,” “COVID” and “SARS-CoV-2”, coupled with “screening,” “triage,” “severity,” “risk,” and “stratification,” “prediction,” “tool,” “index,” and “score,” (online supplemental appendix 1). A secondary search was completed after reviewer comments with the inclusion of emergency specific search terms to help refine the search given the overwhelming growth in the published literature on COVID-19 related topics. Targeted searches were conducted to identify grey literature through Google Scholar and Open Grey. Websites of key regional and international health organisations were also searched, including the European Centre for Disease Prevention and Control, Infection Control Africa Network, International Committee of the Red Cross, Medecins Sans Frontières, UNICEF, US Agency for International Development, US Centers for Disease Control and Prevention, and WHO.
Supplemental material
Inclusion and exclusion criteria
All studies published in English between 1 December 2019 and 1 April 2021 were eligible for inclusion. Multiple forms of literature, including published and preprint manuscripts, correspondence, reports and published guidelines, were considered. Studies were required to describe screening, triage and/or severity scoring of suspected positive or confirmed COVID-19 patients performed by general practitioners or emergency care providers in the prehospital, hospital or clinic setting. Both previously existing tools applied to patients with COVID-19 and novel tools developed specifically for the COVID-19 response were eligible for inclusion. A description of the tool, including inputs (eg, hypoxia) and any relevant parameters (eg, value of input, such as oxygen saturation <93%), was required. As this review aims to describe all tools that may be in use, outcomes data from implementation and/or validation studies were not requisite. Tools could be either proposed or in use, with or without validation. There were no restrictions on the populations that tools may be used in.
Studies in languages other than English or published prior to 1 December 2019 were excluded. Studies describing screening, triage and/or severity scoring only by specialist physicians and those lacking a complete description of the tool were not included. Community-based and population-based screening efforts, performed by healthcare providers or otherwise, were excluded, as were at-home self-triage tools. Descriptions of physical screening or triage infrastructure (eg, a walk-up or drive-through facility) and methods of administering screening (eg, telehealth) were not included.
Data extraction and analysis
Multiple reviewers (SH, JLP, CB and AVN) independently assessed studies for eligibility at the title, abstract, and full-text levels. Any discrepancies were resolved via discussion and a third independent reviewer (AVN, EJCH and CB) where necessary. Relevant data were extracted from eligible texts, including, year of publication, country and setting in which the tool was proposed or implemented, status of the tool as proposed or implemented, and any tool inputs (eg, comorbidities, clinical symptoms and findings and diagnostic and laboratory results). A second researcher reviewed all data extractions to ensure accuracy.
Descriptive analyses were performed, and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses – Extension for Scoping Reviews checklist was used to guide analysis and reporting of these results.17 Feasibility of inputs for use in LRS was determined based on investigation of key literature, including The World Bank’s Disease Control Priorities, Third Edition, and the African Federation for Emergency Medicine’s 2013 consensus statement describing facility level specific, expected capacities for emergency care delivery on the continent.18 19 As with any other setting, LRS have health facilities of varying capacities. In this review, feasibility was targeted towards district level hospitals, as it is these facilities that the majority of LRS populations are likely to initially present to.18 Additionally, as fully resourced health facilities have struggled with the COVID-19 surge, these feasibility inputs may also apply when excess patient volume consumes critical resources or makes imaging difficult.
Patient and public involvement
Given the nature of this review, it was not appropriate to involve patients or the public in this study’s design or execution.
Results
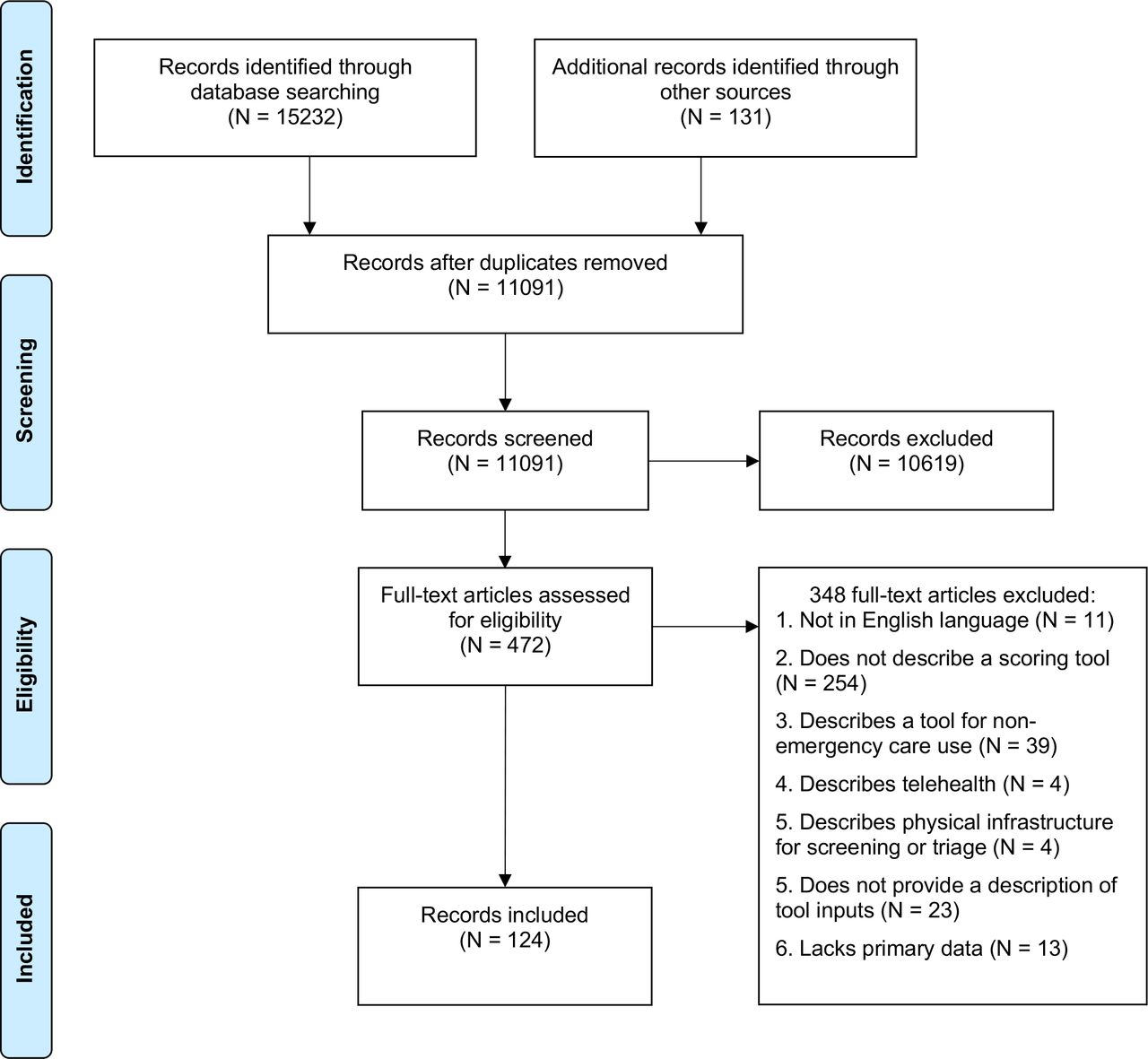
The search strategy yielded a total of 15 232 articles (figure 1). After duplicates were removed, 11 091 unique titles were assessed for inclusion. Following title and abstract screening, 472 articles remained. Full-text review resulted in 124 articles for full inclusion and data extraction (online supplemental appendix 2, tables 1–3).
Supplemental material
{kind=link}
PRISMA flow chart for selected studies.
At the time of inclusion, most articles were peer reviewed (n=99, 79.8%) or preprint manuscripts (n=9, 7.3%). Three articles from the grey literature were also included in the review, reporting on three tools. Articles originated from 27 countries, with the majority published or conducted in China (n=41, 33.1%), followed by the USA (n=23, 18.5%) and Italy (n=10, 8.1%). International recommendations were described in three articles (2.4%).
The majority of the available literrature described severity scoring tools (n=54 articles, 43.5%). Screening tools were described in 48 (38.7%) and triage in 12 (9.7%). Some studies described more than one triage or severity scoring tool. In 10 studies, both screening and triage were described. In total, 57 screening, 23 triage and 54 severity scoring tools were described (table 1).
Overview of tools used to screen, triage and evaluate the severity of patients with COVID-19
Many tools were designed for hospital-wide (n=51, 38.1%) or EU (n=19, 14.2%) use. More than one-third (n=52, 38.8%) did not have a specified setting and were considered to be designed for broad use throughout the healthcare system. Seven tools (6.4%)—five for screening and two for triage—were specific to paediatric settings; nearly all others (n=115, 85.8%) lacked age specifications.
More than one-quarter of tools (n=37, 27.6%) provided validation data supporting their use (online supplemental appendix 2, table 4), with four (of 37; 10.8%) validated prospectively. Most tools were validated against the following outcomes: diagnosis of severe COVID-19 disease (n=8, 21.6%), confirmation of COVID-19 via RT-PCR (n=5, 13.5%) or 30-day mortality (n=4. 10.8%). Only four screening tools (7.0%) and two triage tools (8.7%) had associated validation data, while 29 severity scoring tools (53.7%) did. All of these tools were validated in high-income (n=18, 48.6%) or upper middle-income (n=19, 51.4%) country settings. Of those validated in upper middle-income countries (n=19), 16 were validated in China (84.2%), 2 in Turkey (10.5%) and 1 in Mexico (5.3%).
A total of 204 unique inputs were included in the screening, triage and severity scoring algorithms (table 2 and online supplemental appendix 2, table 5).
Overview of inputs in tools used to screen, triage and evaluate the severity of patients with COVID-19
Screening tools had a median of four (IQR: 3–7) inputs. Most (n=36, 63.2%) included epidemiological risk factors. Fever was commonly included as a reported symptom (n=31, 54.4%) or a measured vital sign (n=17, 29.8%). Triage tools had a median of eight (IQR: 2.5–13.5) inputs. Oxygen saturation was the vital sign most commonly used (n=22, 16.4%), followed by tachypnoea (n=20, 14.9%). Concurrently diagnosed acute conditions were present in multiple triage tools (n=6, 26.1%). Severity scoring tools had a median of five inputs (IQR: 1–8.5). The most frequently used inputs in these tools were age (n=22, 40.1%), lactate dehydrogenase (n=11, 20.4%), respiratory rate (n=7, 37.0%) and temperature (n=5, 9.3%).
Several studies used pre-existing tools to stratify suspected-positive COVID-19 patients: 11 for triage and 19 for severity scoring (online supplemental appendix 2, table 6). The most common tools for severity scoring were the qSOFA and CURB-65 scores and were used in five and four studies, respectively.
Tool inputs that relied on imaging and nearly all laboratory testing were deemed largely impractical for routine use in many frontline EUs in LRS.7 8 In the context of these restrictions, just over half of screening tools (n=31, 54.4%) were viable for use in LRS EUs; a smaller number (n=5, 21.7%) of triage and severity scoring (n=15, 27.8%) tools were also feasible. Many studies describing tools inappropriate for LRS EUs included imaging: 17 screening tools (29.8%), 16 triage tools (69.6%) and 14 (25.9%) severity scoring tools required a chest X-ray, chest CT and/or lung ultrasound. At least one laboratory value was included in seven screening (12.2%), six (26.0%) triage and 28 severity scoring (51.9%) tools. Screening tools were proposed or implemented in six LMICs: 19 in China, 2 in India and 1 each in Mexico, Timor-Leste, Turkey and Uganda, with 16 (55.2%) of these tools deemed feasible for LRS. Triage tools were proposed or implemented in four LMICs: three in China, three in India and one each in Timor-Leste and Turkey, with only four (17.4%) deemed feasible for LRS. Of the 25 severity scoring tools proposed or implemented in LMICs, 18 were from China, 2 were from Pakistan and there was 1 each from Argentina, Brazil, Mexico, Turkey and India; just three (5.6%) are likely feasible in LRS.
Discussion
This scoping review identified a wide range of tools being used to screen, triage, and predict the severity of suspected-positive COVID-19 patients worldwide. A disproportionate share of tools were described in three countries: China, the USA, and Italy, a reflection of the combination of early disease burden and host country research capacities. While more than half of screening tools provided some information about implementation, less than half of triage tools and no severity scoring tools did so. Overall manuscript quality was high, with nearly three-quarters from peer-reviewed publications. Uncertainty remains in regard to the accuracy of these tools: only one-quarter were validated, and variations in settings and reporting make it difficult to generalise and compare data. Almost all studies providing both training and prospective validations showed substantial decreases in accuracy with prospective cohorts. There was also variance in accuracy of the same tools—such as National Early Warning Score (NEWS) and NEWS2—across different high-income and upper middle-income settings.
A majority of the tools identified were for screening, followed by severity scoring, and triage. Tool length varied, though most were short (between four and five inputs). Identified tools with fewer inputs likely have more utility in EUs but, only a small number of tools were purposely designed for EUs. Despite the impact of severity scoring tools on informing appropriate patient interventions and disposition,10 there was no literature available to guide the implementation of severity scoring tools in EUs. While there is substantial variance in presentations in children versus adults,18 very few tools specified a target age group for utilisation. This, in combination with a lack of paediatric-specific tools, suggests a need for additional investigation into appropriate tools for identification and risk of poor outcomes in suspected COVID-19 in paediatric populations.
Screening is an essential means of separating patients with suspected illness from the general population on presentation to the health system. This is particularly critical in LRS, where laboratory testing for COVID-19 is limited,19 and PPE and other resources need to be conserved for positive cases. Most of screening tools found in this review recommended conducting screening on patients using epidemiological risk factors and symptoms consistent with the case definition of suspected COVID-19, such as cough and fever. Non-validated use of such tools could be problematic for multiple reasons. First, it is well documented that there is poor, inaccurate self-reporting of epidemiological risk factors, including exposure to other patients and travel history.20 The impact of epidemiological data in a tool is also limited by the establishment of widespread community transmission, since such transmission indicates that nearly all patients are at risk of exposure. Compounding this is the fact that a substantial portion of COVID-19 cases present atypically, without the commonplace symptoms that providers are screening for using these tools.21 For example, one study of 1099 confirmed COVID-19 cases demonstrated that only 43.8% of COVID-19 positive cases presented with fever.22 More than half of screening tools included fever as a symptom, and many of them considered it requisite to meet the suspect case definition. Challenges in capturing the correct epidemiological data and meeting ‘typical’ case definitions suggests that many screening tools may not effectively identify patients with COVID-19. In addition, in many LRS where the infectious disease burden is high, using fever or cough alone for identification and isolation may be insufficiently specific and create excess burden of suspected cases, leading to delays in care and cross-contamination.23 Also of concern is that, despite the intention of screening as a rapid, first-pass method of identifying patients with suspected COVID-19, many published screening tools relied on laboratory investigations. It is likely that intensive precautions must be taken with these patients while awaiting diagnostic results since, even in the highest resource settings, laboratory results take time. The resources to take these precautions are almost universally limited, and inaccurate screening may place healthcare workers and patients at unnecessary risk.
After screening, patients with suspected COVID-19 should be triaged to determine symptom severity using a standard triage tool contextually validated.24 Following this, patients should be further risk stratified using a severity scoring tool in order to guide clinical management and hospital disposition. Among both triage and severity scoring tools, there was a general lack of consensus about key inputs for prognosticating patients with COVID-19. This is unsurprising, given the novelty of SARS-CoV-2 and the numerous typical and atypical presentations of COVID-19 disease. Despite emerging evidence that any comorbidity, as well as obesity, cerebrovascular disease, chronic obstructive pulmonary disease, diabetes, hypertension, and smoking history correlate with the likelihood of more severe COVID-19 disease,25–27 there was little agreement on which comorbidities to include in tools. Many triage and severity scoring tools included age as an input, congruent with large-scale data that age is a severity modifier. Fewer tools included male sex, despite similar evidence of its predictive value.26 27 Shortness of breath, cough and fever were used in many tools. A concurrent meta-analysis identified that fever and shortness of breath were significant predictors of severe COVID-19 disease, while cough was not.27 A core set of five vital signs—heart rate, oxygen saturation, respiratory rate, systolic blood pressure, and temperature—were seen across triage and severity scoring tools. Although limited data are available on the utility of mental status in predicting COVID-19 illness severity, a majority of reporting studies do indicate that abnormal oxygen saturation, respiratory rate, systolic blood pressure, and temperature are significant predictors of poor outcome.27
Although a large number of screening, triage, and severity scoring tools were described in the literature, LRS use is likely to be limited. More than half of the screening tools identified in this review are likely feasible in LRS, but only a small number of triage and severity scoring tools are. Of the tools proposed for use in LMICs, 51–31 for screening, 5 for triage, and 15 for severity scoring were deemed feasible in LRS. The most notable of these was the integrated screening and triage process used by Howitt et al28 in Timor-Leste. The algorithm was adapted from Ayebare et al29 (Uganda) with the removal of laboratory testing for COVID-19. It uses well-supported inputs, including oxygen saturation and respiratory symptoms, to identify and prognosticate potentially positive COVID-19 patients in a rapid manner. The general lack of validated tools, specifically those for severity scoring, led to the recent development of a contextually appropriate COVID-19 mortality scale for LRS.30 Though not included in this study due to initial search parameters, the AFEM-CMS is a pragmatic tool that makes use of seven demographic, historical, and clinical inputs to evaluate potential risk of death in patients with COVID-19; a second tool includes pulse oximetry. While many LRS EUs lack pulse oximeters needed to evaluate for hypoxia,8 these devices are becoming increasingly available. As such, this review considered pulse oximetry feasible in LRS.
Limitations
Feasibility does not predict that a tool will be accurate or effective. Tools should be validated in the setting of intended use. This review found no tools validated in low-income and lower middle-income countries. Of those validated in upper middle-income countries, nearly all were from well-resourced areas of China, substantially limiting generalisability to LRS. Without contextually appropriate validation data, it is difficult to predict if feasible tools are effective in identifying and risk stratifying patients with COVID-19.
Most of the tools discussed in this review were peer-reviewed publications or guidelines by reputable international organisations, with a smaller number in the form of editorials, published correspondence and preprints. The latter forms of publication often lack peer review and may be of lower quality. Furthermore, this review is likely missing a number of tools. Almost every health system worldwide maintains some form of screening and triage processes, along with processes for further decision making around admission. While in use, both before and during the COVID-19 pandemic, these tools have not been formally published and cannot be described here. Feasibility in LRS was acknowledged if there was a well-described and low-input method of diagnosis available (eg, case definition coupled with vital signs abnormalities) even if it was not necessarily the gold standard of diagnosis in high-resource settings. Risk of bias assessments could not be performed because most articles were in the form of descriptive reviews, rather than the presentation of primary data.
Conclusions
In LRS, where definitive diagnostic tests for COVID-19, such as RT-PCR, may not be available, screening, triage, and severity scoring of potential COVID-19 patients are critical. Rapid identification and prognostication of patients with suspected COVID-19 in LRS EUs will allow for appropriate precautions and care to be rendered to all patients, resulting in conservation of resources and reductions in morbidity and mortality. At present, no screening, triage, or severity scoring tools have been designed and validated specifically for LRS. In the face of an enduring pandemic, it is critical that such tools be developed, validated, and made available, so that limited resources can be conserved for those in greatest need and unnecessary loss of life is prevented.
Data availability statement
The full dataset is available on reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CB, EJCH and SH designed the study. SH and JLP performed the initial literature searches. SH, JLP, CB, EJCH and AVN screened article titles, abstracts and full texts for inclusion and extracted data. SH, CB and JLP cross-checked all data extractions. SH, JLP and AVN drafted the initial manuscript. All authors contributed to manuscript structure and revisions and have approved of the final version. CB is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement statement Given the nature of this review, it was not appropriate to involve patients or the public in this study’s design or execution.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.