Article Text

Abstract
Objectives To determine whether the terrorist attacks occurring in Paris on November 2015 have changed benzodiazepine use in the French population.
Design Interrupted time series analysis.
Setting National population-based cohort.
Participants 90 258 individuals included in the population-based CONSTANCES cohort from 2012 to 2017.
Outcome measures Benzodiazepine use was evaluated according to two different indicators using objective data from administrative registries: weekly number of individuals with a benzodiazepine delivered prescriptions (BDP) and weekly number of defined daily dose (DDD). Two sets of analyses were performed according to sex and age (≤50 vs >50). Education, income and area of residence were additional stratification variables to search for at-risk subgroups.
Results Among women, those with younger age (incidence rate ratios (IRR)=1.18; 95% CI=1.05 to 1.32 for BDP; IRR=1.14; 95% CI=1.03 to 1.27 for DDD), higher education (IRR=1.23; 95% CI=1.03 to 1.46 for BDP; IRR=1.23; 95% CI=1.01 to 1.51 for DDD) and living in Paris (IRR=1.27; 95% CI=1.05 to 1.54 for BDP) presented increased risks for benzodiazepine use. Among participants under 50, an overall increase in benzodiazepine use was identified (IRR=1.14; 95% CI=1.02 to 1.28 for BDP and IRR=1.12; 95% CI=1.01 to 1.25 for DDD) and in several strata. In addition to women, those with higher education (IRR=1.22; 95% CI=1.02 to 1.47 for BDP), lower income (IRR=1.17; 95% CI=1.02 to 1.35 for BDP) and not Paris residents (IRR=1.13; 95% CI=1.02 to 1.26 for BDP and IRR=1.13; 95% CI=1.03 to 1.26 for DDD) presented increased risks for benzodiazepine use.
Conclusion Terrorist attacks might increase benzodiazepine use at a population level, with at-risk subgroups being particularly concerned. Information and prevention strategies are needed to provide appropriate care after such events.
- substance misuse
- mental health
- preventive medicine
- public health
Data availability statement
Data are available upon reasonable request. Personal health data underlying the findings of our study are not publicly available due to legal reasons related to data privacy protection. CONSTANCES has a data sharing policy, but before data transfer, a legal authorisation has to be obtained from the Commission Nationale de l’Informatique et des Libertés, the French data privacy authority. The CONSTANCES email address is contact{at}constances.fr.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The use of a large sample from a population-based cohort of participants randomly recruited from the general French population.
The use of objective and exhaustive data for our two outcomes, allowing a precise measure of benzodiazepine use at repeated time points within a large period centred by the terrorist attacks.
Even considering a large sample of randomly recruited subjects in different health centres across the country, participants may not be representative of the general population.
The reporting method of benzodiazepine use was based on delivered prescriptions; therefore, it is not possible to check whether or not those benzodiazepines were consumed.
Introduction
On 13 November 2015, France faced deadly terrorist attacks.1 Shootings occurred in different places in Paris while hundreds of people were held hostage in a large concert hall. These attacks killed 129 people and wounded more than 300, corresponding to the largest terrorist strike in France since the Second World War.1
Prior literature found that exposure to acts of terrorism could be associated with subsequent mental health issues at a population level,2 3 including post-traumatic stress disorder (PTSD),4 PTSD-related symptoms,5 depressive symptoms,5 negative thoughts6 and acute stress reactions such as anxiety.5 7 Women and those directly exposed to the event might be at higher risk.4 8 However, the impact is not restricted to directly exposed groups, as demonstrated by the nationwide increase in stress reactions after the 9/11 attacks in the USA.9 Nevertheless, it remains unknown whether the exposure to such traumatic event could lead to a nationwide increase in anxiolytic drugs, especially benzodiazepines.
Such an increase would not only highlight the psychological impact of the event but would also have health consequences of its own.10 Short-term use of benzodiazepines is associated with negative side effects such as an increased risk of accidents due to altered psychomotor and cognitive performances.11 12 These negative outcomes of benzodiazepine use are of particular concern in older people. Benzodiazepines could also increase disinhibition and impulsive behaviours, including suicidal behaviours.13 Moreover, patients often use benzodiazepines beyond the recommended short prescription durations, which could be partially explained by the emergence of symptoms of dependence, occurring after only a few weeks of treatment.14 Indeed, benzodiazepines lead to a feeling of well-being quickly perceived by the patient, thus leading to increased risk of misuse, with those at risk being women and older adults.15–19 Furthermore, the specific context of recent exposure to a traumatic event might require particular caution. Some studies have suggested that benzodiazepines should be contraindicated in this context, considering their ineffectiveness in prevention of PTSD symptoms and even their potential association with an increased risk of developing PTSD or depressive state as well as decreased response to psychotherapy.20
We took advantage of the unique features of the large national population-based CONSTANCES («CONSulTANts des Centres d'Examens de Santé ») cohort to examine benzodiazepines prescriptions, which are collected longitudinally and objectively from administrative registries.21 Thus, our aim was to examine changes in benzodiazepine use in the French population after November 2015 terrorist attacks in Paris using two different indicators: the number of individuals with a prescription and the overall amount of benzodiazepine consumed. We hypothesised that the terrorist attacks were followed by an increase in benzodiazepine use. Age and sex are associated with discrepancies regarding vulnerability to affective disorders on one hand,8 17 22 and different pattern of benzodiazepine use on the other hand.10 15–19 Indeed, women were found to be more vulnerable to both affective disorders and benzodiazepine use, whereas older subjects were found to be more vulnerable to benzodiazepine use and less to affective disorders. Particularly, being over 50 years of age has been found to be an important risk factor of benzodiazepine use.19 Thus, all the analyses were conducted separately for age and sex.10 15–19 In addition, we performed additional stratified analyses for education, income and area of residence to search for at-risk subgroups.4 8 10 15 19
Methods
Cohort description
The CONSTANCES23 cohort is a national population-based cohort of randomly recruited participants, including volunteers aged 18–69 years at baseline in 22 selected health centres. To be recruited, participants must be covered by the general health insurance scheme (more than 90% of the French population). Written informed consent was received from all of the subjects in the CONSTANCES cohort. In the present study, we selected participants included in the cohort from 2012 to 2017 who gave consent for their data to be linked to administrative registries.
Patient and public involvement
Patients or members of the public were not involved in the design of this study, nor in its implementation. Patients and general public will be informed of the results of the study via publication.
Indicators of benzodiazepine use
The CONSTANCES cohort benefits from its systematic linkage to the ‘Système national d’information inter-régimes de l’Assurance maladie’ database.21 This national administrative database contains detailed individual medical data, including reimbursement data of prescribed drugs. We extracted filled prescriptions for all benzodiazepines having a marketing authorisation in France from the database, that is, prescriptions that patients have been purchased in pharmacies. These benzodiazepines include: clonazepam, chlordiazepoxide, diazepam, oxazepam, potassium clorazepate, lorazepam, bromazepam, clobazam, prazepam, alprazolam, nordazepam, ethyl loflazepate and clotiazepam. Then, we built two complementary indicators of weekly benzodiazepine use to monitor and evaluate modifications in benzodiazepine consumption at a population level—the total number of participants with a benzodiazepine delivered prescription (BDP) per week—the overall amount of consumed defined daily doses (DDD) per week. DDDs are widely used to assess drugs global consumption.24
Stratification variables
We ran two sets of analyses, stratifying on sex on one hand and age on the other hand (≤50 vs >50). Within these two sets, additional stratified analyses were planned for the following sociodemographic factors : (a) education based on the 2011 International Standard Classification of Education and categorised in aggregated modalities: (1) levels 0 and 1 (early childhood education and primary education) and level 2 (lower secondary education); (2) levels 3 and 4 (upper secondary education and post-secondary non-tertiary education); (3) levels 5 and 6 (short-cycle tertiary education and Bachelor’s or equivalent level) and (4) levels 7 and 8 (master’s or equivalent level and doctoral or equivalent level); (b) household income in euros per month and categorised in four modalities (<2100; from 2100 to 2800; from 2800 to 4000; >4000); (c) residence area (Paris region and outside Paris).
Statistical analyses
To examine changes in benzodiazepine use, we conducted interrupted time series analyses (ITS). ITS is a quasi-experimental design classically used to evaluate public health interventions.25–27 ITS allows to examine whether an event could change the course of a time-dependent variable at a population level when a preinterruption period and a postinterruption period can clearly be identified.25 Segmented regressions were performed using Poisson regressions adjusted for overdispersion. A level change model was implemented as we hypothesised that the terrorist attacks would have an immediate effect on benzodiazepine use. The event was introduced as a binary variable to estimate its role on weekly benzodiazepine use according to the two aforementioned indicators (considered as counts). Therefore, all model included one of the two indicators as the outcome. Variables included in the different models were: the binary variable representing the occurrence of the event, with the resulting coefficients (β1) estimating the level change following the event, and a continuous variable representing the elapsed time (in weeks, as observations were taken in weeks), with the resulting coefficients (β2) estimating the underlying trend.25 Since our goal was to estimate the immediate effect of the terrorist attacks, results present the estimations of the coefficients associated with the occurrence of the effect. Results are presented as incidence rate ratios (IRR) with their 95% CIs (95% CI). Considering that in ITS statistical power increases with the number of time points included,25 28 we aimed to maximise the number of included time points while avoiding other periods close to other specific traumatic events. We consequently introduced in the time series a total number of 60 time points, that is 30 weeks before and 30 weeks after the attacks. Sensitivity analyses were conducted to examine potential confounding period effects. We reproduced our main analyses focusing on the second week of November 2013, a period in which there was no particular traumatic event at a population level. We also ran sensitivity analyses using hypnotic treatments (such as zopiclone and zolpidem) to address whether the observed effects could be specific to the aforementioned benzodiazepine group. Analyses were conducted between June 2019 and March 2020. All the analyses were performed using Stata V.15.0 (StataCorp).
Results
Characteristics of the overall sample
A total of 90 258 participants (46.8% of men and 53.2% of women) have been included in the statistical analyses. The median age of our sample was 49 years old and 53.2% were women. Detailed participants’ characteristics are available as online supplemental material 1. Within the included time period (ie, 60 weeks), the mean number of subjects per week with at least a BDP was 569 (SD=7.2) and the mean number of DDD per week was 12 454 (SD=164.7). The mean numbers of subjects per week with at least a BDP were of 548 (SD=8.6) and of 591 (SD=10.4) for the 30 weeks before and after the attacks, respectively. The mean numbers of DDD per week were of 12 157 (SD=202.5) and of 12 751 (SD=251.6) for the 30 weeks before and after the attacks, respectively. Using paired t-tests for dependent variables, we did not find a statistically significant difference between DDD means (p=0.07), but there was a statistically significant difference between BDP means(p=0.005).
Supplemental material
When applying the regression model within the whole sample, we found no statistically significant increase in benzodiazepine use neither for BDP nor DDD: IRR=1.08 (95% CI=0.98 to 1.18; p=0.116) for BDP and IRR=1.05 (95% CI=0.95 to 1.17; p=0.327) for DDD.
Changes in benzodiazepine use within sex groups
The mean numbers of men subjects per week with at least a BDP were of 209 (SD=26.2) and of 223.4 (SD=21.3) for the 30 weeks before and after the attacks, respectively. The mean numbers of DDD per week were of 5369.4 (SD=717.1) and of 5525.3 (SD=715.9) for the 30 weeks before and after the attacks, respectively. Paired t-tests comparison didn’t find a significant difference for DDD (p=0.42) but found a statistically significant difference for BDP.
However, when applying the regression model, we found no statistically significant increase in benzodiazepine use overall, nor among any strata in men (table 1).
Incidence rate ratio of benzodiazepine use in men associated with the occurrence of the terrorist attacks (N=42 218)
The mean numbers of women subjects per week with at least a BDP were of 338.7 (SD=26.4) and of 367.7 (SD=39.1) for the 30 weeks before and after the attacks, respectively. The mean numbers of DDD per week were of 6787.4 (SD=552.5) and of 7226 (SD=786.9) for the 30 weeks before and after the attacks, respectively. Paired t-tests comparison found statistically significant differences for both BDP (p=0.002) and DDD (p=0.015).
When applying the regression model among women, no statistically significant modification in benzodiazepine use was identified overall (IRR=1.09; p=0.064 for BDP; IRR=1.08; p=0.136 for DDD), but an increase in benzodiazepine use was found within several strata. Regarding age in this group, we found a statistically significant increase in benzodiazepine use among women under 50 years (table 2). There was a 18% increase in the number of women with at least a BDP per week (IRR=1.18; p=0.006) after the attacks, and a 14% increase in the overall DDD per week (IRR=1.14; p=0.014). We found a significant increase in benzodiazepine use among women with higher education level. Specifically, women with short-cycle tertiary education and Bachelor’s or equivalent level presented a statistically significant increase in the number of subjects with a BDP (IRR=1.17; p=0.043), as well as those with at least a Master level or equivalent (IRR=1.23; p=0.022). The latter also presented a significant increase in overall DDD per week (IRR=1.23; p=0.045). We found a significant increase in benzodiazepine use after the attacks among residents of the Paris region regarding the number of subjects per week (IRR=1.27; p=0.014). We found no changes in benzodiazepine use in stratified analyses according to income.
Incidence rate ratio of benzodiazepine use in women associated with the occurrence of the terrorist attacks (N=48 040)
Changes in benzodiazepine use within age groups
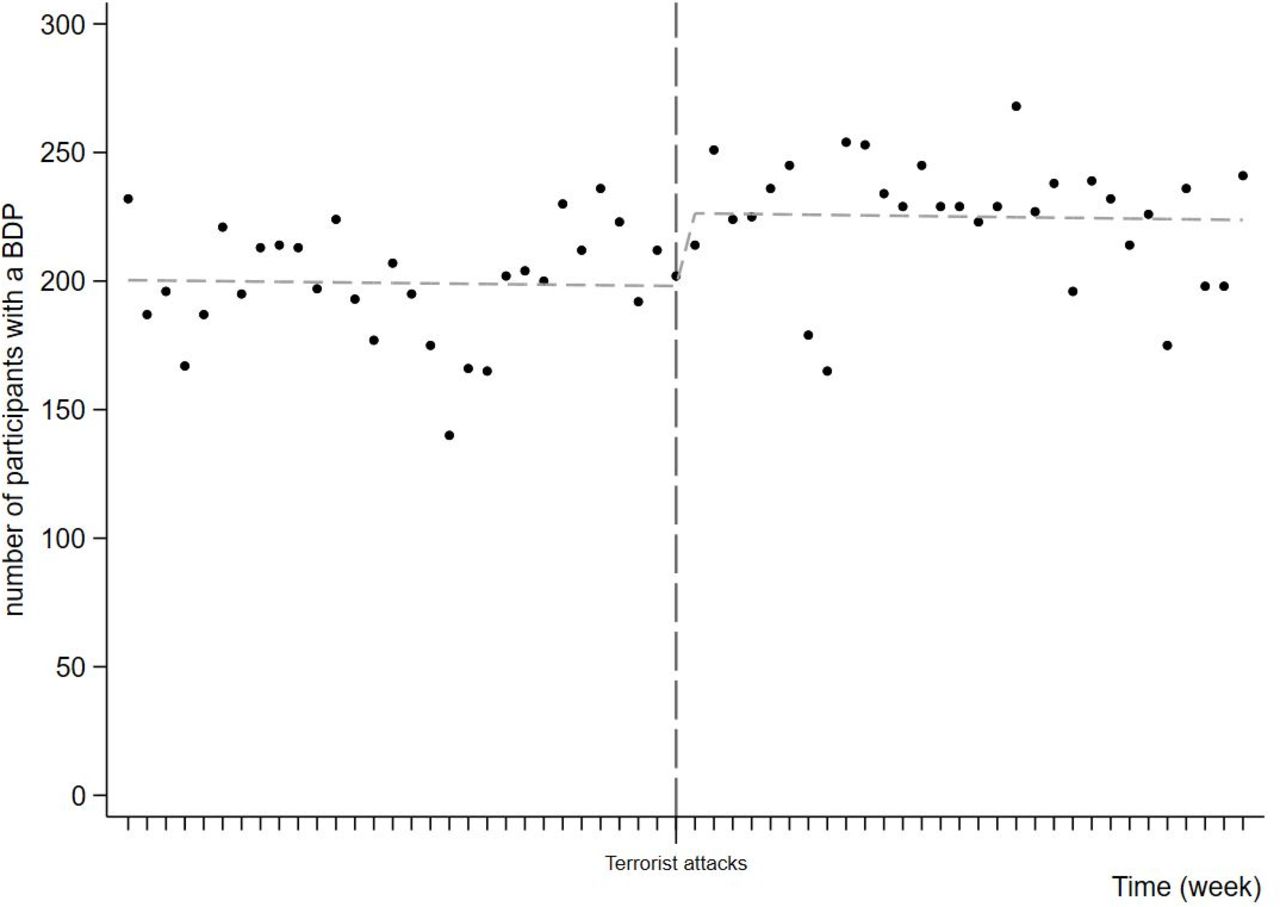
The mean numbers of subjects aged under 50 per week with at least a BDP were of 199.2 (SD=22.3) and of 225.1 (SD=24.1) for the 30 weeks before and after the attacks, respectively. The mean numbers of DDD per week were of 4373.8 (SD=450.6) and of 4836.6 (SD=516.4) for the 30 weeks before and after the attacks, respectively. Paired t-tests comparisons found statistically significant differences for both BDP (p<0.001) and DDD (p=0.002).
When applying the regression model within participants under 50, an increase in benzodiazepine use was found overall (IRR=1.14; p=0.019 for BDP and IRR=1.12; p=0.039 for DDD) (table 3). Figure 1 displays these changes graphically (for BDP). Increased benzodiazepine use was also found within several strata. As already shown, women had a significant increase regarding both indicators. We found a significant increase in BDP among participants under 50 with greater education level. Those with short-cycle tertiary education and Bachelor’s or equivalent level presented a statistically significant increase in the number of subjects with a BDP (IRR=1.19; p=0.042), as well as those with at least a Master level or equivalent (IRR=1.22; p=0.030). We found a significant increase in benzodiazepine use among participants under 50 with lower household income (≤2100), with a 17% increase in the number of subjects with a BDP per week (IRR=1.17; p=0.027). In this younger age group, we did not find a significant increase in benzodiazepine use after the attacks among residents of the Paris region. For this association, the estimated effect size of the number of subjects with a BDP per week was similar to the one obtained within the women strata (IRR=1.20, (95% CI=0.96 to 1.49) and IRR=1.27 (95% CI=1.05 to 1.54), respectively), but did not reach significance. However, we found a significant increase in benzodiazepine use among residents of the Paris region. Precisely, there was a 13% increase in the number of subjects with a BDP per week after the attacks (IRR=1.13; p=0.025), and a 13% increase in the overall DDD per week (IRR=1.13; p=0.013).
{kind=link}
Number of participants aged under 50 with a benzodiazepine delivered prescription (BDP) per week during the 60 weeks period centred on the terrorist attacks of November 2015 in Paris (N=48 040). Dashed line=predicted trend based on the regression model.
Incidence rate ratio of benzodiazepine use in participants aged under 50 associated with the occurrence of the attacks (N=48 818)
The mean numbers of subjects aged over 50 per week with at least a BDP were of 348.5 (SD=30.7) and of 366.1 (SD=36.8) for the 30 weeks before and after the attacks, respectively. The mean numbers of DDD per week were of 7782.9 (SD=763.1) and of 7914.7 (SD=935.5) for the 30 weeks before and after the attacks, respectively. Paired t-tests comparison did not find any significant difference, neither for DDD (p=0.55) nor BDP (p=0.051)
When applying the regression model within participants aged over 50, no significant modification of benzodiazepine use was found overall. Considering the different strata, we only found an increase in the number of subjects with a BDP among residents of the Paris region (IRR=1.18; p=0.030) (table 4).
Incidence rate ratio of benzodiazepine use in participants aged over 50 associated with the occurrence of the attacks (N=41 440)
In sensitivity analyses focusing on the second week of November 2013, prior significant differences in changes in benzodiazepine use were no longer observed.
Sensitivity analyses using BDP or DDD for hypnotic treatments did not find any increase in hypnotic treatment use.
Of note, among all the parameters estimating an underlying trend within the different strata, none of them was significantly associated with any of the outcomes.
Discussion
This study provide results suggesting that the November 2015 terrorist attacks were associated with an increase in benzodiazepine use in several groups of the French population. Increased benzodiazepine use was observed in individuals aged less than 50 but also within subgroups of women (those under 50, with higher education and residents of the Paris region). In addition to the overall increased risk of benzodiazepine use identified within the group of younger participants, particularly at-risk subgroups of participants under 50 were also identified: women as expected, but also those with higher education, lower income and living outside Paris.
We did not find an overall increase in benzodiazepine use when considering the entire population of the study. Nevertheless, patterns of benzodiazepine use widely differ within sex and age groups, so an overall analysis may ignore specific schemes in more vulnerable groups.
According to this latter statement, we found an increase in benzodiazepine use within several strata in women but not in men, which is in line with prior studies identifying sex as an important risk factor for benzodiazepine use.15 16 19 Sex differences in benzodiazepine use could be explained by more frequent mood and anxiety disorders among women.17 Women could also have a more frequent use of the healthcare system, and be more likely to use medication to cope with stress.17 Furthermore, women could present a greater vulnerability to the effects of traumatic events.8
In prior studies, older age had been identified as a strong risk factor of benzodiazepine use.15 19 Here, we identified a greater variation in benzodiazepine use after a nationwide traumatic event in younger participants. That might be explained by a greater vulnerability to external events in younger subjects, as compared with older ones which are already at-risk of consumption, due to other factors. Furthermore, these terrorist attacks targeted sites particularly frequented by younger people, such as concert hall, restaurants and bar terraces. Thus, the increased risk of benzodiazepine use after the attacks among this age group may partially rely on stronger identification mechanisms leading to greater emotional distress. This could also apply to the other criteria defining at-risk subgroups, such as higher education and lower income, since students and young actives could be more prone to frequent the sites in which the attacks took place. We also found that Paris residents were at increased risk of benzodiazepine use which is consistent with prior studies identifying geographical proximity as a major risk factor for developing various stress reactions after a traumatic event.4 5 29 However, an increase in benzodiazepine use was found in those living outside the Paris region, indicating that the attacks might have also affected people far from the attacks site, which is in accordance with prior findings.9 Indeed, it has already been highlighted that terrorist attacks represent shared traumatic experiences at a population level that may lead to psychological consequences among people not directly exposed.5 30 It is noteworthy that participants residing outside Paris who were at increased risk were particularly vulnerable subjects (ie, the younger ones). As suggested by other studies,31 32 media exposure could also play an important part.33
Our study has a number of strengths. We used a large population-based cohort, with a sufficient sample size to search for at-risk subgroups. The use of administrative registries also allowed us to use objective and exhaustive data while ensuring the stability of our population (ie, the sample (and its sociodemographic characteristics) remain the same through the time period considered). In addition, we used two complementary indicators of benzodiazepine use, that is, number of BDP and overall DDD. For instance, in some subgroups, there was only a significant increase in the number of subjects per week with a BDP, but not in the overall DDD per week. These results could reflect an increase in prescriptions of low dosages or short duration of treatments. Finally, since benzodiazepine use data came from administrative registries, our outcomes relied on exhaustive (ie, no missing data) and objective data (ie, treatment purchased in pharmacies).
However, this study has also some limitations. First, even in a large sample of randomly recruited subjects, these participants may not be representative of the general population. Second, our reporting of benzodiazepine use was based on delivered prescription and therefore does not ascertain those benzodiazepines were actually used and does not include over-the-counter consumption. However, this reporting method reflects a health condition requiring a medical examination that led to a prescription of an anxiolytic drug. Furthermore, benzodiazepines cannot be obtained without prescription in France. Third, the results presented here are obtained from exploratory analyses using different stratification variables. Although multiple comparisons lead to alpha risk inflation, it is of note that all the observed associations point towards the same direction, in line with our hypotheses. Fourth, since our main outcome was a count obtained from aggregated data, we are not able to examine individual trajectories of benzodiazepine use. Therefore, we could not formally discriminate between a small effect shared in a large number of participants and a large effect in few individuals. However, we had two complementary indicators of benzodiazepine use, taking into account the total number of individuals using benzodiazepine and the overall amount of benzodiazepine used. Finally, although our sensitivity analysis did not find any modification of benzodiazepine use on a similar time period of 2013, more advanced statistical analyses can be used to describe variations other time.34 We cannot totally rule out that the observed changes in benzodiazepine use could result from other co-occurring factors. However the use of ITS with precise measures at repeated time points over a well-defined period centred by the event should limit those biases.25 28 Moreover, sensitivity analysis showed no changes in benzodiazepine use over the same period in the previous year.
Our findings have different implications from a public health perspective. First, they reflect the importance of acute stress manifestations at a population level following a terrorist attack, leading to an increase in benzodiazepine use. Women and younger subjects could be particularly vulnerable. Public health policy-makers should be aware of these detrimental consequences to better inform the population and design prevention strategies. Second, benzodiazepines are not recommended to treat acute stress manifestations in this context.20 General practitioners and other primary care workers should thus be better informed on the recommended non-pharmacological strategies.35 We also identified sociodemographic factors that could help to target vulnerable subjects for such information and prevention strategies. Moreover, even those that are not geographically close to the sites of the attacks may experience an emotional distress intense enough to result in a benzodiazepine prescription. Therefore, caregivers should pay attention to acute stress manifestations among their patients, considering that they could be affected even without having being directly exposed.
Future studies should focus on defining different trajectories of changes in benzodiazepine use in order to distinguish those who would only have transient consumption and those who would start chronic use. Future studies could also focus on shorter time periods or on the use of emergency care to identify whether a critical time period is particularly concerned. Qualitative studies aiming at understanding the motivation to use benzodiazepines in this particular context would also be particularly helpful while defining information and prevention strategies.
Data availability statement
Data are available upon reasonable request. Personal health data underlying the findings of our study are not publicly available due to legal reasons related to data privacy protection. CONSTANCES has a data sharing policy, but before data transfer, a legal authorisation has to be obtained from the Commission Nationale de l’Informatique et des Libertés, the French data privacy authority. The CONSTANCES email address is contact{at}constances.fr.
Ethics statements
Patient consent for publication
Ethics approval
The CONSTANCES cohort has obtained the authorisation of the National Data Protection Authority (Commission Nationale de l’Informatique et des Libertés, no. 910486) and was approved by the Institutional Review Board of the National Institute for Medical Research-INSERM (no. 01-011).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CG, GA, CL, MZ and MG designed the study; CG, GA and EC worked on literature search; SK, MZ and MG contributed to collection and assembly of data; CG, GA, SK, CL, MZ, MG and FL contributed to data analysis and interpretation; SK, MZ, MG and EC provided technical support. All authors have contributed to interpretation and critically reviewed the manuscript. All authors approved the final version of the manuscript.
Funding There are no funders to report for this specific submission. The CONSTANCES cohort is supported by the Caisse Nationale d’Assurance Maladie des travailleurs salaries-CNAMTS. CONSTANCES is accredited as a ‘National Infrastructure for Biology and health’ by the governmental Investissements d’avenir program and was funded by the Agence nationale de la recherche (ANR-11-INBS-0002 Grant). CONSTANCES also receives funding from L’Oreal, MSD, AstraZeneca and Lundbeck managed by INSERM-Transfert (Award number : Not Applicable). EC is supported by the Medical Research Council (MR/T032499/1). CG confirms that he had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Disclaimer The funders did not have any role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests CG, EC, MG and MZ have no conflict of interest to report. GA has received speakers and/or consulting fees from Pfizer, Lundbeck and Pierre Fabre. CL has received speakers and/or consulting fees from Boehringer Ingelheim, Janssen, Lundbeck and Otsuka Pharmaceutical. FL has received speaker and/or consulting fees from AstraZeneca, Lundbeck, Janssen, Roche, Servier and Otsuka Pharmaceuticals.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.