Article Text

Abstract
Objectives This study aimed to achieve an expert consensus on how to define and group footwear interventions for children, with a further focus on the design characteristics and prescription of off-the-shelf stability footwear for children with mobility impairment.
Setting A group of multinational professionals, from clinicians to those involved in the footwear industry, were recruited to ensure a spectrum of opinions.
Participants Thirty panellists were contacted, of which 24 consented to participate and six withdrew before round 1, a further two withdrew after round 1. Sixteen panellists completed the consensus exercise.
Primary and secondary outcome measures A Delphi consensus method was employed with round 1 split into three sections: (1) terms and definitions, (2) specifics of off-the-shelf stability footwear design and (3) criteria for clinical prescription of off-the-shelf stability footwear. The panel was asked to rate their level of agreement with statements and to provide further insights through open-ended questions. The opinions of the experts were analysed to assess consensus set at 75% agreement or to modify or form new statements presented through the subsequent two rounds.
Results Therapeutic footwear was the agreed term to represent children’s footwear interventions, with grouping and subgrouping of therapeutic footwear being dependent on their intended clinical outcomes (accommodative, corrective or functional). Both the heel counter and topline as well as the stiffness and width of the sole were identified as potentially influencing mediolateral stability in children’s gait. A consensus was achieved in the prescription criteria and outcome measures for off-the-shelf stability therapeutic footwear for cerebral palsy, mobile symptomatic pes planus, Duchenne muscular dystrophy, spina bifida and Down’s syndrome.
Conclusions Through a structured synthesis of expert opinion, this study has established a standardisation of terminology and groupings along with prescription criteria for the first time. Reported findings have implications for communication between stakeholders, evidence-based clinical intervention and standardised outcome measures to assess effectiveness.
- paediatric orthopaedics
- paediatric orthopaedic & trauma surgery
- rehabilitation medicine
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The authors will share the data for this work on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
A multinational sample of professionals from clinicians to those involved in the footwear industry was sought to ensure a spectrum of opinions were included.
Analysis followed a standard mixed-method approach for Delphi consensus surveys and employed both qualitative and quantitative analysis.
The study was limited to countries with English as their first language, and there may be differences in expert opinions outside the selected expert’s countries (Australia, UK and USA).
This research paves the way for the development of appropriate mechanical testing methods for off-the-shelf therapeutic stability footwear.
Introduction
Footwear is a fundamental common boundary between the ground and the foot in daily activities; it modifies forces and sensory stimulus with demonstratable effects on children’s gait.1–3 Correspondingly footwear has been used both historically and in modern healthcare practice as an assistive aid for children with mobility impairment.4 5 However, a recent scoping review6 highlighted that footwear as a clinical intervention for children lacks a common understanding of terms and definition as to the specifics of its clinical role. The development of recognised terms, definitions and characteristics of a healthcare intervention afford an understanding of how it should work, the value it should provide, who should benefit, how to measure its success, what risks are present and what is and is not included within the intervention.7 8 The scoping review6 demonstrated that numerous terms have been used in the literature concerning clinical footwear interventions, including orthopaedic shoes, rehabilitative boots, modified shoes, supportive shoes and special shoes. Additionally, there was no clear definition of the clinical role and outcome measures to classify and group the range of available children’s footwear interventions. The results of the scoping review suggested therapeutic footwear as a potential overarching term to represent the myriad roles and designs of children’s clinical footwear interventions, with three primary groupings of therapeutic footwear categorised according to common identified clinical roles. The groupings were: corrective (footwear designed to bring about the correction of congenital skeletal lower limb alignment), accommodative (footwear designed to reduce stresses on children’s foot deformity through the matching of footwear dimensions to the child’s foot) and functional (footwear designed to improve dynamic gait parameters of mobility-impaired children, reducing pathological movements and facilitating typical walking patterns inclusive of stability).6
Among the therapeutic footwear groupings suggested in the scoping review,6 those that offered a stabilising role were the most studied. Research has demonstrated potentially beneficial clinical outcomes to children with mobility impairment with increased velocity and lowered mediolateral excursions of the centre of mass in walking.9–11 Children’s stability footwear may be bespoke or have uppers that come in a range of modular adaptions but are most commonly made to a manufacturer’s standard stock model, which are termed off the shelf.10 12 The body of research concerning off-the-shelf stability footwear has chiefly focused on its biomechanical effects. However, the specific standard design characteristics for this footwear that are requisite for stability were not clearly identified or consistently reported in the literature.6 9 The lack of recognised characteristics of an intervention prevents a common understanding of how it should work clinically7 8 and preclude a meaningful comparison throughout any evidence-based research.9 Thus, it is important that a consensus understanding of design characteristics required to enhance stability during gait is obtained, from both a manufacturing and clinical perspective, for this footwear.
In respect to who may benefit from this intervention,7 8 there were seven childhood mobility impairments considered for off-the-shelf stability footwear intervention among the research identified through the scoping review: cerebral palsy, pes planus, toe walking, Duchenne muscular dystrophy, spina bifida, Down’s syndrome and intoeing.6 However, there appeared to be no clear prescription criteria for the use of off-the-shelf stability footwear in these conditions. Specific gaps in prescription criteria included the stated clinical role, the grade/severity of the condition when this footwear should be used as a sole assistive aid or an adjunct to other aids such as ankle foot orthoses (AFOs) and the suitable age range for intervention.6 9 In addition, there appears to be no standardised set of agreed outcome measures, both physical and psychosocial, to ascertain the effectiveness of this footwear.9 Identification and consensus agreement of outcome measures for both research and clinical practice allows for a unified measure of the effectiveness of an intervention, informing on value-driven healthcare and the development of a consistent evidence base.13
Although terminology and means of grouping clinical footwear interventions as a whole have been suggested by a synthesis of the available research,6 9 a common understanding and usage of these terms would require an opinion on their practical application from experts who provide footwear to children with mobility impairment. Once the overall groupings and terminology of clinical footwear interventions have been established among experts in this area, it will be possible to identify and define individual intervention footwear categories for childhood mobility impairment, such as stability footwear. Off-the-shelf stability footwear appears to offer a beneficial effect on the broadest range of childhood mobility impairments.6 9 However, as stated, a common understanding of the specifics and purpose of their design and the proposed clinical outcomes of this treatment is not apparent in the research.6 9
Where there is contradictory or insufficient information, the ability to formulate effective clinical reasoning can be affected; here consensus surveys such as the Delphi offers a valid and reliable method of determining expert opinion to inform on these areas.14–16 Delphi surveys incorporate the collective opinion of a panel of experts fed back to the panel through a series of iterative rounds in an anonymised and controlled manner, with the underlying goal to achieve expert consensus on a certain issue where no agreement previously existed. This technique has been used successfully to achieve professional consensus on school footwear design17 and the use of orthoses for mobility impairment.18 19 The only previous study relating to the synthesis of expert opinion on footwear interventions was performed by Staheli and Giffin in 1980.4 This was a single round cross-section survey of practice and opinion that lacked the staged systematic approach of a Delphi survey and was restricted to the correction of musculoskeletal alignments that are mainly found in typically developing children. The survey did not consider the footwear terminology used, the purpose of the specific designs of footwear or any effects on children’s gait.4 Establishing a common understanding of terms, definitions and groupings of clinical footwear as a whole, alongside design characteristics and prescription criteria for specific footwear groupings, may be achieved by conducting a Delphi consensus with experts in the field of clinical footwear provision and design. The consensus opinion may then be used to develop consistent terms and definitions for footwear interventions and prescription criteria and design characteristics for off-the-shelf stability footwear for children with mobility impairment.
Aims and objectives
The overall aim of this study was to achieve an expert consensus on how to define and group clinical footwear interventions for children, with a further focus on the design characteristics and clinical prescription of off-the-shelf stability footwear for children with mobility impairment.
The objectives were:
To establish expert consensus on the terms, definitions and groupings of children’s clinical footwear interventions, providing a consistent and common clinical understanding to identify and categorise the purpose of these footwear types as an assistive aid for children.
To establish a consensus of expert opinion of the ideal design characteristics of off-the-shelf stability footwear and the purpose of these characteristics.
To develop expert consensus recommendations for the prescription criteria and outcome measures for off-the-shelf stability therapeutic footwear.
Method
This Delphi consensus study followed the methodological and reporting recommendations suggested by Keeney, Hasson and Mckenna.20 21 The development and purpose of this survey were informed by scoping and systematic reviews performed by the authors.6 9
All panellists provided written informed consent to participate in this study.
Patient and public involvement
Due to the nature of this study, no patients or public were involved in the design, implementation or analysis of results.
Identifying panellists
Experts were recruited by the purposeful sampling of individuals meeting specific criteria:
Registered practitioner in healthcare or clinical footwear manufacture.
≥10 years of practice in clinical footwear provision/manufacture.
≥25% clinical caseload involving the provision of footwear interventions to children with mobility impairment or ≥25% of their workload involved with the design or manufacture of footwear intended for therapeutic use in children with mobility impairment.
Recruitment was initially through professional networks of the research team and subsequently recruited experts were asked to identify additional experts who they felt met the criteria for this study. A multinational sample of professionals from clinicians, researchers and those involved in the footwear industry was sought to ensure a spectrum of opinions were included. Although there are no agreed definitions for an effective size convention ranging from 10 to 100 panellists within the literature,22 researchers have suggested a sample size of 10 will provide a diversity of expert opinion.23
Contacting experts
Experts were contacted with the information sheet by email, with consent and a participant professional characteristic survey captured by Microsoft Forms.
Questionnaire design
The study took the form of a modified Delphi15; the first round was informed by scoping and systematic reviews of research in relation to children’s clinical footwear interventions6 9 and benchtop analysis of design characteristics of a range of off-the-shelf footwear proposed to offer a stabilising effect on mobility impaired children. This approach allowed the development of informed questions from the available evidence. The survey consisted of closed-ended ranked and option questions, with ranked questions using a 7-point Likert scale. Open-ended questions were also provided to explore the panellists’ opinions on the statements and questions posed and to allow them to offer alternatives or raise further salient items in relation to children’s clinical footwear interventions. The first round of the survey, therefore, captured qualitative and quantitative data. This generated a combined synthesis of the current literature evidence base in relation to children’s clinical footwear interventions alongside that of the experts’ opinions from working in the area of clinical footwear provision.
The survey was designed by the first author with calibration and modification of questions among all authors. The survey was also piloted on an expert in clinical footwear provision to ensure the questions were appropriately framed and phrased to avoid ambiguity or multiple events within any question.24 The first round consisted of three sections:
Section 1 asked the panellists for their opinion on consistent terms, definitions and groupings of clinical footwear interventions for children with mobility impairment. An example of the type and structure of the questions is provided in figure 1, with the full section 1 survey available in online supplemental appendix S1.
Supplemental material
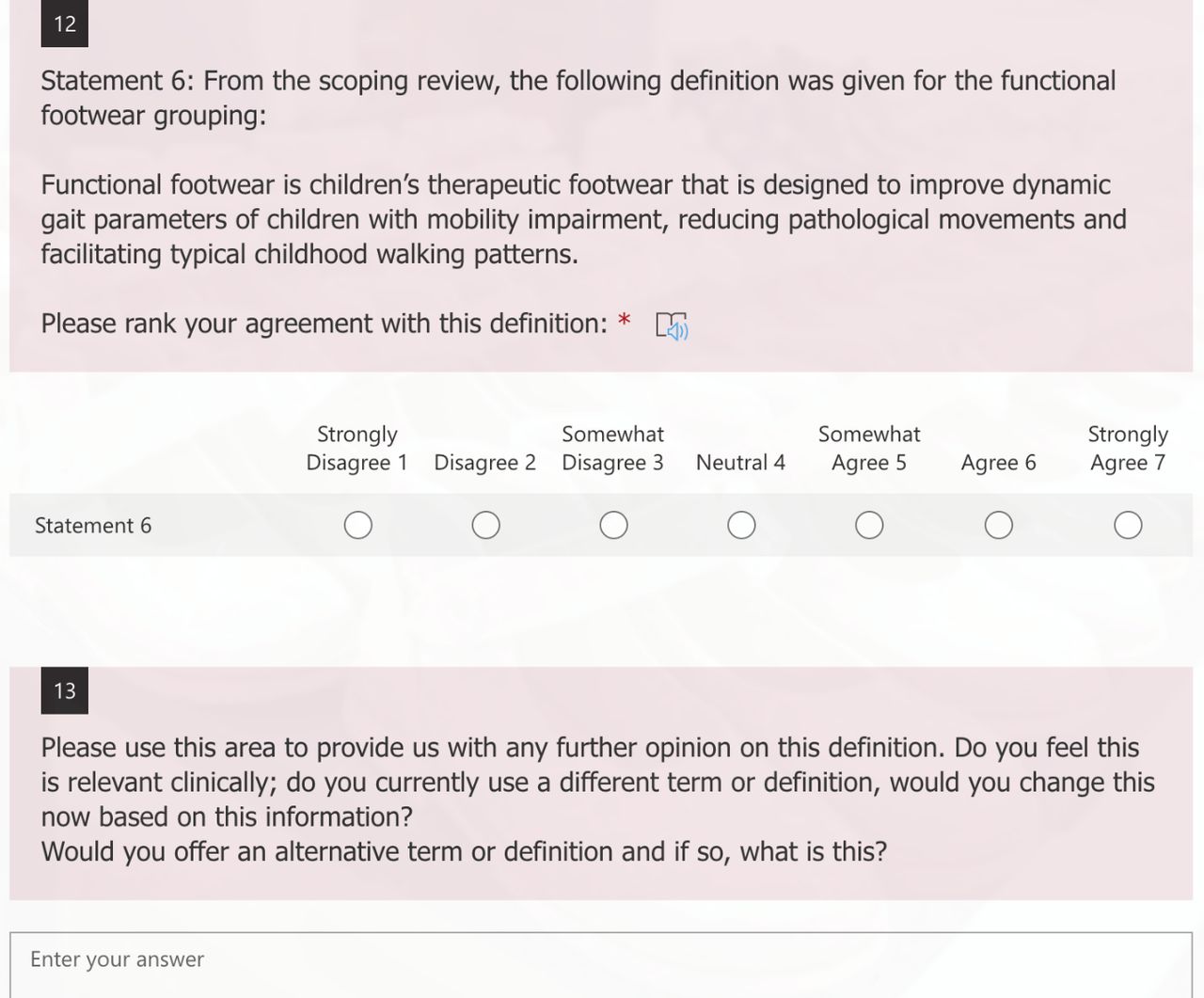
An example of a question from section 1 exploring consistent terms and definition of clinical footwear interventions (* indicates required answer).
Section 2 asked the panellists for their opinion on the ideal design characteristics of off-the-shelf stability footwear and the purpose of these characteristics. An example of the type and structure of the questions is provided in figure 2, with the full section 2 survey available in online supplemental appendix S2.
Supplemental material
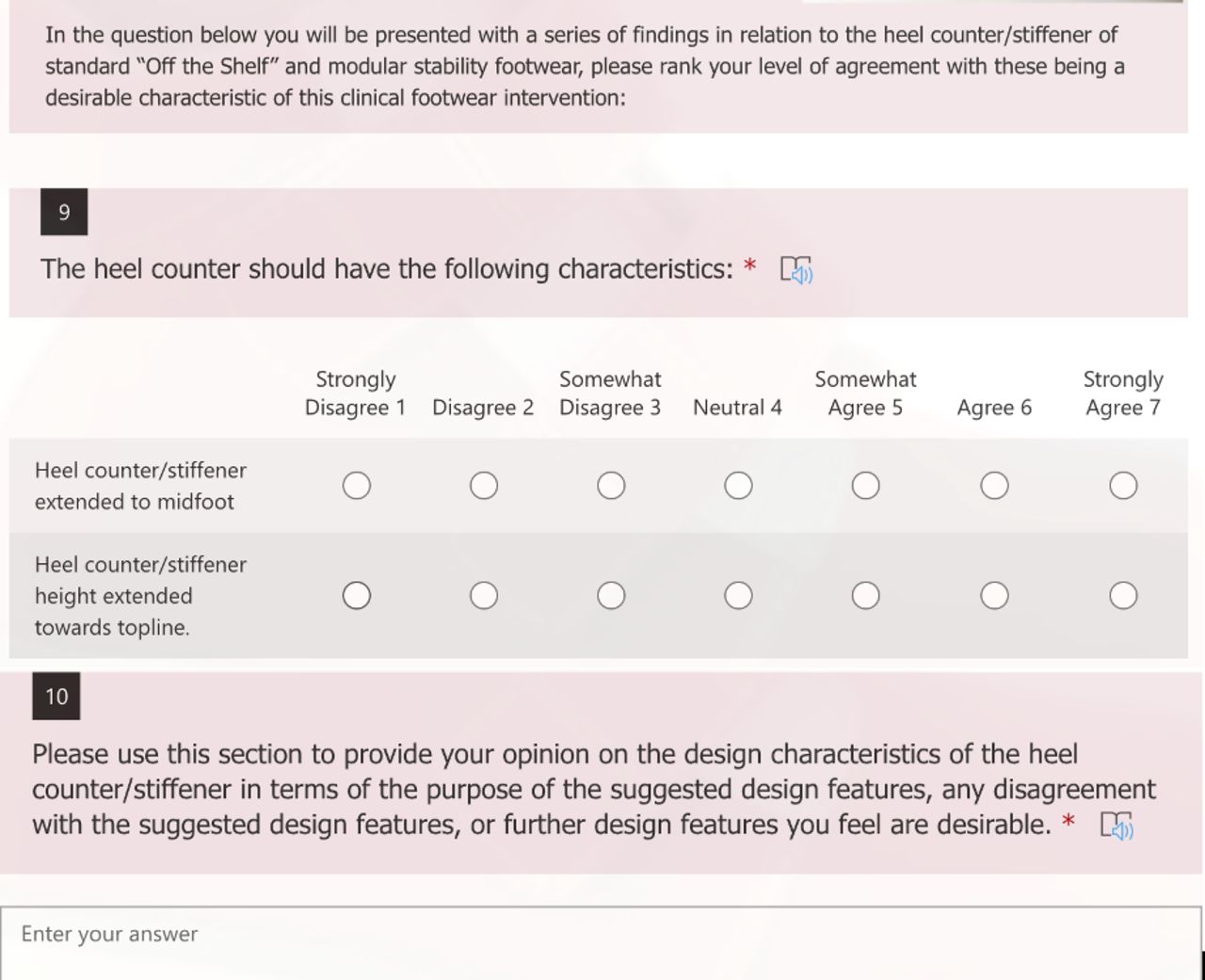
An example of a question from section 2 exploring recognised design characteristics of children’s off-the-shelf stability footwear (* indicates required answer).
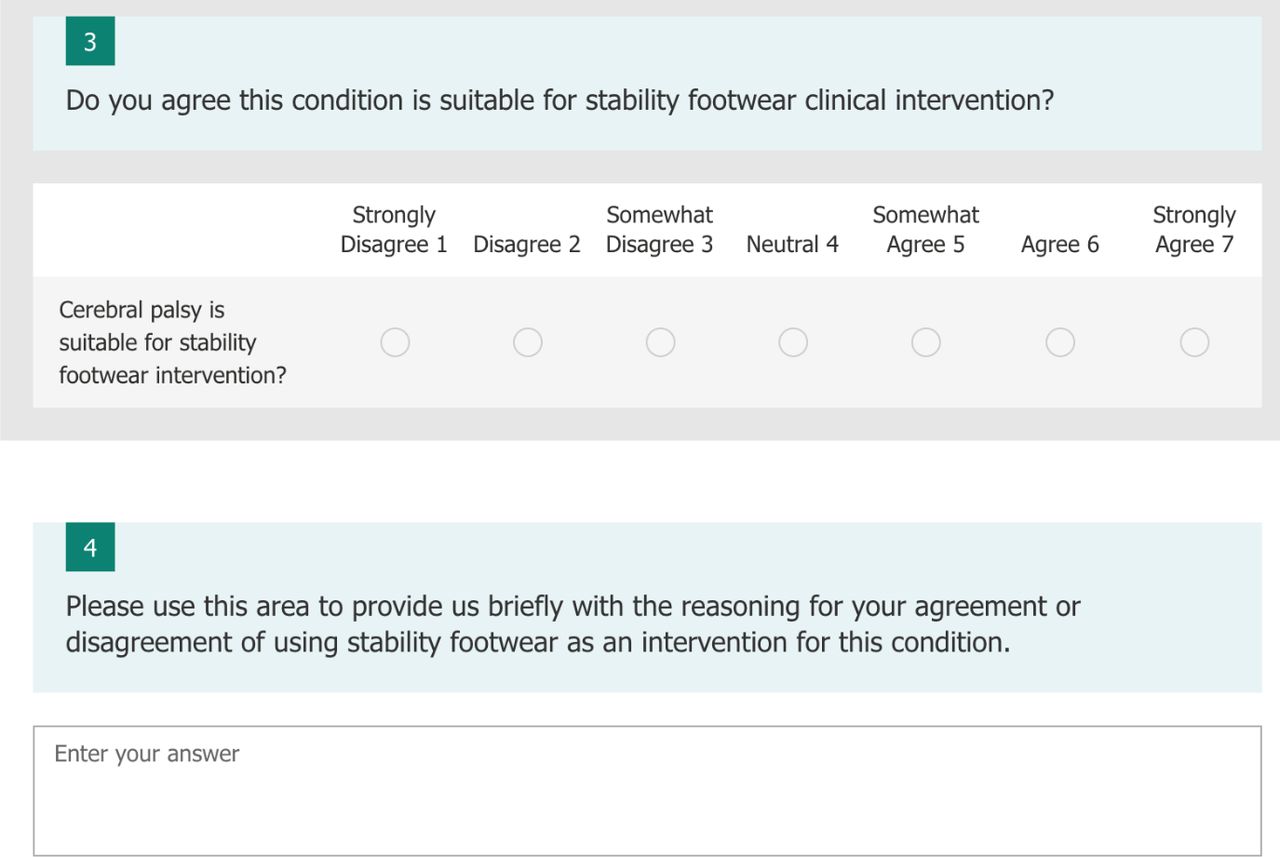
Section 3 asked the panellists for their opinion on the prescription criteria of issuing commercially available off-the-shelf stability footwear in a range of mobility impairments and the outcome measures to be used to assess the effectiveness of this footwear. An example of the type and structure of the questions is provided in figure 3, with the full section 3 survey available in online supplemental appendix S3.
Supplemental material

An example of a question from section 3 exploring prescription criteria for the provision of children’s off-the-shelf stability footwear.
The panellists were given instructions on how to complete the survey in the introduction of each section.
Distribution
The survey was distributed among panellists electronically via Microsoft Forms. Panellists were reminded to complete the survey 1 week before the deadline. Late responders were followed up and offered an appropriate extension if required.
Analysis of results
Analysis followed a standard mixed-method approach for Delphi consensus surveys and employed both qualitative and quantitative analysis. The combined findings were used to inform the development of subsequent rounds of Delphi (two and three) in addition to the final results.
Analysis of open-ended questions involved an inductive themed content analysis framework performed by the first author.25 The process involved the identification of statements that were the same or could be constructed to mean the same thing. These statements were grouped together, and themes were developed around similar statements. Once statements were grouped under a common theme, a decision was made among the research team as to whether these themes should be collapsed into one statement to be presented to the Delphi panel in the subsequent round. Unique statements that did not fall into any common theme were kept as the original statements. The wording of all statements was assessed by the research team for potential multiclauses and ambiguity.
The grouped themed and unique statements were presented to the panellists alongside a summary of the collective panellists’ reasoning in rounds 2 and 3. These were in a series of ranked Likert scale questions or options alongside the original statements from round 1 or 2. Rounds 2 and 3 followed the same format of round 1 with three sections (online supplemental appendices S1–3).
Descriptive statistics: central tendency and dispersion of the responses (median analysis, IQR) and % frequency to the ranked questions were fed back to the panellists in rounds 2 and 3 for an estimation of the general response of the other expert panellists (online supplemental appendices S1–3). The quantitative values were also recorded for consistency analysis across the rounds.
Consensus
There is no agreed guidance on consensus but is often achieved through generating a predetermined percentage level of consensus of ranked questions or panellists preferred option (frequency).14 15 The range of preset agreement is variable among Delphi studies; however, a value of 75% is a commonly reported value26 and the one chosen to define consensus among the recruited panel in the present study. Statements would reach consensus when there was 75% or greater frequency of response for a preferred option or ranked questions of ‘agree’ to ‘strongly agree’.
Cut-off
The Delphi was set a priori to run over three rounds or if there was a greater than 30% drop off of panellists.
Results
Thirty panellists were contacted in January 2020, of which 24 consented to participate; six participants withdrew from the study prior to commencement of the first round. Eighteen panellists participated in round 1; the panel consisted of orthotists, podiatrists and a physiotherapist with a range of experience and roles in clinical footwear provision for children, including direct patient contact, education, research and commercial sales and manufacture. The international panel was composed of panellists from the UK, Australia and the USA; a full breakdown of the panellists' characteristics are provided in (table 1).
Participant characteristics
Of the 18 panellists, 16 completed all rounds of the Delphi survey resulting in an 11% drop off from the initial round (figure 4). From the initial 45 statements (11 in section 1, 27 in section 2 and 7 in section 3), a further 238 statements were developed or modified from panellist feedback (figure 4) for a total of 283 statements. Consensus agreement among the panel was reached on a total of 150 statements (figure 4). The statements for each section inclusive of the original, modified and those that reached consensus are found in supporting information files (online supplemental appendix S4–6). The results for each section are presented and discussed separately.
Supplemental material
Supplemental material
Supplemental material
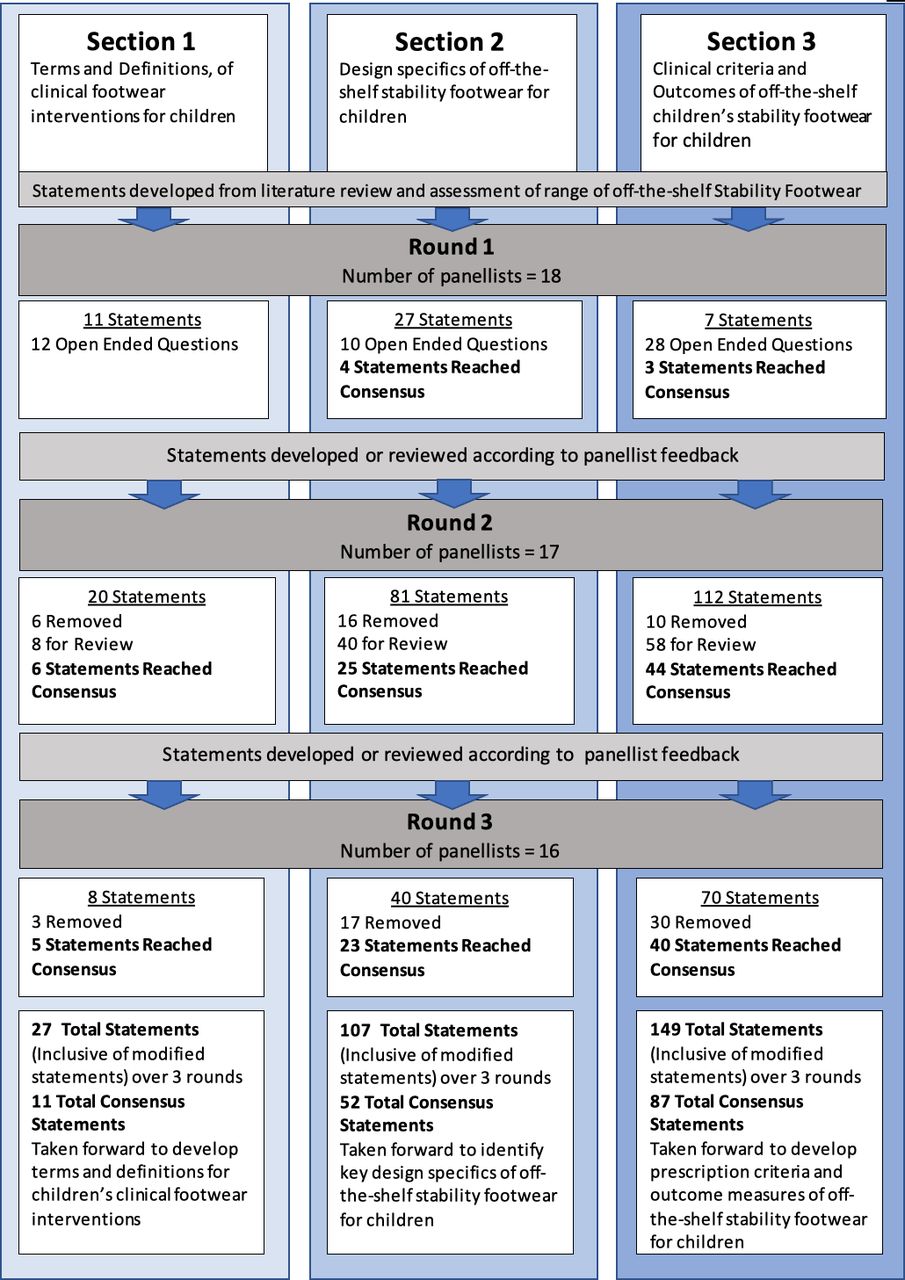
The Delphi survey three-round process and individual sections results.
Section 1
The 11 consensus statements from section 1 were taken forward to establish consistent terms and definitions to broadly group and categorise children’s clinical footwear interventions. There was a considerable majority consensus of the panel (81% agreement) who favoured therapeutic footwear as the overarching term for children clinical footwear interventions (figure 5). This term was felt by the majority of the panel to reflect the holistic aspect of footwear interventions on childhood mobility rather than be limited to aspects of aligning body structure that would be suggested by ‘orthopaedic’ and ‘orthotic’. A broad overarching definition was established by panellists (82% agreement) for these interventions as:
Footwear that is designed or adapted specifically to protect, support, align, prevent, or correct foot deformity, or to assist mobility and standing in children.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Terms and groupings of clinical footwear interventions for children derived from section 1.
This definition comprised the scope of the potential role of footwear as a clinical intervention while also recognising that designs may incorporate specific therapeutic footwear or standard shoes that are adapted to meet a clinical purpose. Groupings of footwear fell under the overarching term therapeutic footwear (100% agreement), and panellists felt they should be grouped and categorised according to intended clinical outcomes of the components of the footwear (100% agreement). This was modified from the suggested method of groupings from the scoping review6 in which the groupings assigned footwear as an individual design. The current grouping recognised that footwear might have more than one clinical role, that is, footwear may have both a direct functional component on gait and an accommodative component of the child’s foot deformity. The main groupings of therapeutic footwear were those offered in round 1, which were taken from the scoping review6: accommodative, corrective and functional (figure 5). However, the definitions were modified by panellist’s feedback with all achieving consensus in the second round:
Accommodative footwear is children’s therapeutic footwear that is designed to prevent deterioration of children’s foot deformities through the dimensional matching of the footwear to the child’s foot. (76% agreement)
Corrective footwear is footwear that is designed or adapted to support correction of congenital or acquired foot and ankle deformity in children. This may be secondary to a primary corrective measure such as serial casting or surgery. (82% agreement)
Functional footwear is children’s therapeutic footwear that is designed or adapted to directly assist mobility and standing in children. (76% agreement)
Panellists felt that functional footwear could be placed into subgroupings dependent on the design and intended clinical outcomes of the footwear similarly to that suggested for the main groupings of therapeutic footwear (76% agreement). The panellists favoured the subgrouping of stability footwear suggested from the scoping review provided in round 1 (94% agreement) (figure 5). However, the definition was modified by panellists’ feedback and did not achieve consensus until the third round:
Stability Footwear is footwear that is designed to assist mobility and standing in children by influencing movements and potentially proprioception of the foot and ankle. (94% agreement)
Panellists felt that the separate subgroupings of lift (raise*), rounded bottom (rocker bottom*) suggested from the scoping review in round 1 should be considered to fall collectively under one subgrouping. Therefore, a new separate subgrouping of functional footwear adapted sole was suggested from panellist feedback; this reached consensus in round 2 (76% agreement) (*preferred alternative terminology suggested by the majority of panellists in round 1) (figure 5). This was defined as:
A range of customised sole or heel adaptions to any suitable children’s footwear, with the adaptions designed to assist mobility or standing in children.
From panellist feedback, the subgrouping of adapted sole recognised that there is a range of sole adaptions offering varied functional roles broader than stability. However, it was beyond the scope of the current Delphi to fully categorise and define the many sole adaptions that could fall into this subgrouping. Further detail on panellist opinion in the development of the subgrouping adapted sole may be found in online supplemental appendix S4.
Section 2
The 52 consensus statements from section 2 concerning the specific ideal design characteristics and purpose of off-the-shelf stability therapeutic footwear were distributed in nine regions of the shoe: topline, upper, facings and fastenings, heel counter/stiffener, heel, inlay, sole unit, sole rocker, in addition to overall consideration of the footwear’s mass (table 2). Three key themes emerged from panellist feedback concerning the ideal design characteristics and their purpose those of stability, ergonomics and aesthetics (table 2). Stability was felt to be achieved by material stiffens of the heel counter (81% agreement), which may be assisted by an increased topline height in offering mediolateral stability to the foot and ankle (81% agreement). Panellists also felt that the fitting of the shoe inlay/insole to the child’s heel should not be overlooked to increase vertical ground reaction forces in this area in addition to the firm anchorage of the counter to the welt and outer sole (88% agreement) (table 2). Although a proprioceptive effect of the heel counter and topline was suggested by some panellists, full consensus (69% agreement) could not be achieved as a number of panellists were not convinced that the current evidence base supported the design components influence on proprioception. Other design features that were thought to impart stability and reached consensus were the: width of the heel in relation to the upper (87% agreement), stiffness of the outsole at the midfoot and rearfoot (88% agreement), tread depth of the outsole (87% agreement), lace fastenings (81% agreement) and leather upper of high tensile strength properties (93% agreement). The overall mass of the shoe was not thought to improve the stability properties of the shoe; it was, however, proposed and achieved consensus as a potential cause of instability in the swing phase of gait if too heavy.
Themes of the ideal design specifics and purpose of off-the-shelf therapeutic stability footwear derived from section 2
The second key theme concerning the ideal design characteristics of off-the-shelf stability therapeutic footwear was in relation to ergonomics. Ergonomic aspects considered the fit and comfort of the shoe during wear and the ease in which the shoe could be donned and doffed on a child’s foot with limited mobility. Originally in round 1, specific statements were presented to the panellists in relation to the design of this footwear, for example, ‘Extended topline height above the ankle’ and ‘The fastening should have the following characteristics: Lace’. However, panellist opinion and feedback established a consensus preference to a pragmatic range of ergonomic options based on the child’s ability, age and clinical need over the course of rounds 2 and 3, for example:
The topline extension should come in an optional range both above and below the ankle dependent on the patient’s ability and needs. (93% agreement), and The Fastenings should be Optional dependent on patient’s ability and desired goal (eg, Velcro for limited hand dexterity, lace for greater stability). (93% agreement)
Panellists felt that the upper (93% agreement) and heel counter (80% agreement) should be available in a range of dimensions for any given size of off-the-shelf stability therapeutic footwear to accommodate a child’s foot and ankle anatomy. The material of the upper should come in a range of materials to include breathable and wipeable fabrics for warm climates and issues with continence (100% agreement). The topline should be padded at the collar (88% agreement) and contoured to the ankle anatomy (80% agreement) to minimise mechanical stress to this region. Facings should be offered extended to the toe box to allow easy access (donning and doffing of the footwear) for children with limited movement of the foot and ankle (93% agreement).
Fastening should be in both lace and Velcro fastening to accommodate children’s manual dexterity and allow a degree of independence (93% agreement). The mass of the footwear should be the lowest reasonable to reduce the physiological cost of walking (100% agreement). However, it was recognised that older children might require heavier footwear to account for increased mobility or enhanced stability requirements such as a stiffened outsole or extended heel counter that may additionally increase the footwear’s mass (93% agreement). A consensus of the panellist was reached concerning the inlay/insole of off-the-shelf stability footwear, in that contouring at the heel improves rearfoot fit (81% agreement), and the inlay should be removable and thick enough to represent replacement by a possible adjunct orthosis (100% agreement). However, the specifics of the design in relation to contouring to the arch and heel failed to reach a consensus (63% agreement). Similarly, the purpose of a forefoot rocker to facilitate forward progression in gait and not affect the swing phase of gait reached a consensus (93% agreement). However, the standard design requirements of the rocker did not reach a consensus (56% agreement). Aesthetics of the footwear was proposed by the panellists in recognition of the psychosocial needs of children and felt that the visual appeal of the shoe was important to facilitate social interaction with peers with this statement receiving 100% agreement among the panel on initial consideration in round 2.
Section 3
The 87 consensus statements concerning children’s mobility impairments suitable for off-the-shelf stability therapeutic footwear intervention resulted in consensus recommendations for the prescription criteria and outcome measures for five of the initial seven conditions: cerebral palsy (92% agreement), mobile symptomatic pes planus (86% agreement), Duchenne muscular dystrophy (92% agreement), spina bifida (80% agreement) and Down’s syndrome (85% agreement) (tables 3–4). Five further conditions were suggested and reached a consensus among the panel: Charcot-Marie-Tooth (92% agreement), hypermobility (Ehlers-Danlos type) (92% agreement), developmental coordination disorder (100% agreement), Rett’s syndrome (80% agreement) and chronic lateral ankle instability (77% agreement) (online supplemental appendix S6). However, the prescription criteria and outcome measures for the treatment of these further conditions were unable to be explored without further extending the Delphi survey and risking panellist fatigue.14
Prescription criteria for off-the-shelf stability therapeutic footwear
Clinical outcome measures for off-the-shelf stability therapeutic footwear in children with mobility impairment
In relation to the prescription criteria for off-the-shelf stability therapeutic footwear, there were three areas that reached a general consensus for the five conditions:
The footwear provides mediolateral stability at the foot and ankle in walking and standing. Meaning it could act as both a walking aid and transfer aid (range 79%–88% agreement) (table 3).
The provision of off-the-shelf stability therapeutic footwear should only be issued to children with mobility impairment after a critical assessment of the child’s mobility needs in respect to other assistive aids or footwear modifications and with clear clinical outcomes (range 86%–92% agreement). Panellists voiced their concern that this footwear had been historically uncritically prescribed in the conditions exampled. Panellists felt foot orthoses serving similar function are less obtrusive and potentially cheaper. Consequently, a consensus (86% agreement) was reached that off-the-shelf stability therapeutic footwear should only be used as a secondary line of intervention for symptomatic pes planus where foot orthoses had failed to resolve symptoms.
In relation to the suitable age range for off-the-shelf stability therapeutic footwear intervention, a pragmatic approach to initiation and endpoints reached consensus in that it should be based on the functional ability and the mobility needs of the child rather than a specified age (range 77%–94% agreement).
Other areas suggested by panellists were concerning the use of this footwear as a sole aid or adjunct to other assistive devices. Most indications for the use of off-the-shelf stability therapeutic footwear was as an adjunct to other assistive devices (range 77%–92% agreement) to aid mediolateral stability in walking and standing (table 3). These other assistive devices included foot orthoses, AFOs, knee ankle foot orthoses (KAFOs), hip knee ankle foot orthoses and walking and standing frames. Indications for off-the-shelf stability therapeutic footwear as a sole aid were limited to low-grade cerebral palsy with no tonal issues (81% agreement) and the early walking stage of individuals with Down’s syndrome (94% agreement). It was also noted by panellists that the foot anatomy of children with Down’s syndrome presents a challenge with footwear fitting. Therefore, the practitioner should consider available last adaptions to accommodate the dimensions of these children during prescription (85% agreement).
Two of the seven originally proposed conditions suggested from the scoping review toe walking and intoeing failed to reach any consensus statements concerning the suitability and clinical indications for stability footwear intervention. However, it must be noted that idiopathic toe walking moved closer towards consensus statements for clinical indications (range 60%–67% agreement) than intoeing (range 25%–44% agreement).
Outcome measures proposed by the panellist were broadly aligned to biomechanical, physiological, gross motor proficiency and quality of life (QoL) measures. In relation to biomechanical measures, ankle range of motion reached consensus as an outcome measure for cerebral palsy, symptomatic pes planus and Duchenne muscular dystrophy (range 80%–88% agreement). Spatiotemporal outcome measures including walking velocity, 6 min walk test and Timed Up and Go reached consensus among the five conditions (range 77%–90% agreement). Kinematic outcome measures also achieved consensus among the five groupings (range 77%–90% agreement); these were in relation to optimising gait movement patterns of the foot and ankle against disease-specific scores, Edinburgh Gait Score and Hoffer Ambulation Score or normal available data sets. None of the suggested kinetic outcome measures achieved a consensus level of agreement (range 60%–67% agreement). Physiological outcome measures concerning cardiovascular and metabolic exertion were proposed and reached consensus (range 75%–91% agreement) for cerebral palsy, spina bifida and mobile pes planus. Outcome measures based on the child’s ability to perform activities via measures of gross motor skills reached a consensus among the five conditions (range 75%–88% agreement) (table 4). Consensus was also reached by the panel in that suitability of physical outcome measures must consider the stage/grade of Duchenne muscular dystrophy and the capability of the child to perform the tasks (88% agreement). QoL measures, pain and activities of daily living outcome measures for off-the-shelf stability footwear intervention reached consensus agreement for all five conditions to a relatively high level (range 79%–100% agreement). With the majority of QoL outcome measures reaching consensus on initial consideration in round 2.
Discussion
Despite the historical and relatively common usage of clinical footwear interventions in children with mobility impairment,5 6 there has been a lack of common understanding of how to define and characterise this intervention. The collective opinion of the expert panel and the consensus formed through the inductive and iterative process of this study allowed novel ideas to be synthesised alongside previously published information. Clinical footwear interventions for children with mobility impairment reached a common understanding and were collectively grouped and defined under the overarching term therapeutic footwear. This allowed the identification and categorisation of one of the more potentially effective of these interventions, stability footwear9 as a subgrouping of functional footwear. The process also provided a consensus understanding of the ideal design characteristics for off-the-shelf stability therapeutic footwear and how this intervention may be used in a range of childhood mobility impairments. As stated, only one previous study had explored expert opinion on footwear as a clinical intervention for children.4 The current study has provided a more detailed synthesis of expert opinion providing consensus on terms and definitions for children’s clinical footwear interventions in addition to identifying the specifics and purpose of off-the-shelf stability therapeutic footwear design and criteria for clinical prescription for children.
Section 1 sought to obtain consensus on definitions terms and groupings for clinical footwear interventions in children. Although this represented the smallest section in the total number of statements and open-ended questions in round 1, it received the most detailed and rich comments for qualitative analysis, underlining the potential contentiousness of this section. However, this was the only section that received a consensus statement for each area presented to the panel. It is highlighted that a consistent language of terms and definitions is required in healthcare practice to improve interprofessional communication, healthcare research and provide optimal patient outcomes.8 27 The suggested terms definitions and groupings, incorporating children’s footwear interventions from this study, have been obtained using a valid consensus approach.15
The survey also sought to focus on off-the-shelf stability therapeutic footwear, which is a potentially effective footwear intervention for children’s mobility impairment9 The survey provided consensus agreement of a number of ideal design characteristics that should be offered on off-the-shelf stability therapeutic footwear for children, and the purpose of these. Identification of the key design specifics of an assistive aid affords an understanding of how and where the aid should support and assist mobility and has been used to help develop interventions such as AFOs.27–29 However, the panellists pointed out there was a limited evidence base to support these stability design characteristics. Some panellist proposed potential neurodynamic properties of the footwear through proprioceptive feedback at the heel counter and extended topline. However, panellists felt that further evidence was required to justify this claim. In comparison with stability features of the footwear, the panellists appeared more certain with their opinion on ergonomic factors as this achieved consensus in earlier rounds and is probably due to the established body of work in footwear science that relates comfort and fit to function.30–33 Although there is a lack of evidence to substantiate the design characteristics purported to offer stability, the identification of these areas may inform further mechanical testing of off-the-shelf stability therapeutic footwear.
In addition to the design characteristics of children’s off-the-shelf stability therapeutic footwear, the survey sought to gain opinion and consensus on the clinical criteria for providing this footwear and the outcome measures to ascertain its effectiveness. Uncertainty on prescription criteria and goals of treatment can lead to inconsistent practice and lack of confidence in providing assistive aids to mobility-impaired children.34 35 This section initially started with the least number of statements in round 1 but went on to generate a total of 149 statements for panellist consideration. Criteria for prescription were largely to improve mediolateral stability in mobility and standing. Off-the-shelf stability therapeutic footwear may often be prescribed by clinicians as a first-line intervention based on historical practice. However, expert consensus recommends that prescription of this footwear be assessed critically against the mobility needs of the child and the evidence base of other assistive devices, with the most suitable intervention being issued. Off-the-shelf stability footwear was to be used simultaneously with other assistive devices (AFOs KAFOs walking frames) in more severe gradings (Gross Motor Functioning Classification Score (GMFCS) 2–4) with only minor gradings indicated for sole line treatment with off-the-shelf stability therapeutic footwear (GMFCS 1). The exception to this was symptomatic pes planus where it may be used only as a secondary line intervention after foot orthoses had failed to resolve symptoms. Body structure and function outcome measures were chiefly focused on spatiotemporal and kinematic measures in addition to the physiological cost. Kinetic measures did not reach consensus; however, this was largely due to the perceived compliance with in-shoe measurement devices and availability of force plates in clinical settings rather than the validity of these outcome measures. It was, therefore, uncertain if the panellists considered if outcomes were inclusive of research settings as well as daily clinical practice. QoL measures appeared to be considered an important outcome for off-the-shelf stability therapeutic footwear intervention in children with mobility impairment as these reached a higher frequency of strongly agree and in earlier rounds compared with the other outcomes. Conversely, the current body of research is limited, exploring the effects of footwear interventions on the QoL of children.9
Idiopathic toe walking and intoeing did not achieve any consensus for clinical criteria of off-the-shelf stability therapeutic footwear provision. Idiopathic toe walking was not felt by the panel to be completely unsuitable for off-the-shelf stability therapeutic footwear intervention. It was noted that it presented with a nebulous aetiology with variable responses to many interventions.36 The establishment of criteria therefore required more complex stratification than the closed-ended statements offered in the current survey. Intoeing again was cited as heterogeneous in nature37; however, this achieved the highest frequency of panellists scoring disagree or strongly disagree with panellists reaching a general consensus there was no clear evidence base to indicate off-the-shelf stability therapeutic footwear for this clinical presentation even in the subcategories suggested by the modified statements offered across rounds 2 and 3.
Five further conditions were suggested through consensus of the panellists; however, it was beyond the capacity of the current survey to explore the clinical criteria and proposed outcomes for off-the-shelf stability therapeutic footwear intervention in these additional conditions. This will require further exploratory work among experts in the area of clinical footwear provision to establish this.
The Medical Research Council38 provides a list of recommendations in developing and evaluating complex interventions. Paramount to the development process is that an intervention should be able to be fully defined in what it is expected to do and under what situations. There should be a full understanding of the components of the intervention and how these should act, who the intervention is aimed at and what the salient outcome measures expected to be achieved.7 38 The results of the Delphi consensus process have outlined and defined the spectrum of roles footwear may play as a clinical intervention. Further to this, the results of the study provided an expert consensus of off-the-shelf stability therapeutic footwear including the identification of the design characteristics purported to enhance mediolateral stability in children’s gait, the childhood mobility impairments that may benefit from stability footwear intervention and the necessary outcomes to evaluate the footwear’s effectiveness in these children. While this consensus has identified several design characteristics, which the experts considered pertinent for off-the-shelf stability therapeutic footwear, further consideration should be given on how to assess these characteristics using mechanical testing procedures and in turn link them to International Organization for Standardization (ISO standards.
The Delphi technique has limitations in that it does not necessarily produce the right or definitive answers; instead, it produces a valid consensus of expert opinion.21 The method uses both qualitative and quantitative analysis in a mixed-method approach; however, the data provided from Delphi’s are of inductive level 5 evidence39 and are not authoritative requiring further deductive empirical research to support the findings of the work.15 The recruitment to the Delphi panel was limited to countries with English as their first language, and potential differences in expert opinions may exist outside the selected experts’ countries (Australia, UK and USA). We actively sought a range of professionals from both the clinical and manufacturing sectors to have a full, balanced understanding of the design specifics and purpose of the footwear. While there is a possibility of unconscious bias among the participants’ response as a result of their personal affiliations with either the clinical and commercial sectors, it has certainly not affected the credibility of the results. Although we did not require a formal declaration of conflict of interest, the professionals were required to state their role in children’s footwear intervention and any conflict of interests has been detailed on the table of participant characteristics.
The themes were derived by content analysis performed by one author. This may potentially have introduced some bias in interpretation of the expert opinions; however, this was mitigated by a collective agreement of statement generation between the authors from the themes, and the opportunity for panellists to correct any misrepresentation or omission of their opinions in the subsequent Delphi rounds.
This study has achieved an expert consensus on defining and grouping clinical footwear interventions for children, where none previously existed. Additionally, the ideal design characteristics for off-the-shelf stability therapeutic footwear for children with mobility impairment and suitable clinical populations for their provision have been identified.
The consensus will facilitate:
A common understanding of therapeutic footwear terminology to facilitate communication between clinicians, researchers and manufacturers.
Research-informed evidence for selection of appropriate off-the-shelf stability therapeutic footwear based on identified design characteristics.
Research-informed evidence for dispensing off-the-shelf stability therapeutic footwear to suitable clinical populations.
Standardised outcome measures for clinical assessment of the effectiveness of off-the-shelf stability therapeutic footwear interventions.
Conclusion
The current study is the first to establish a structured synthesis of expert opinion on defining and grouping children’s therapeutic footwear, in addition to identifying the design characteristics of off-the-shelf stability therapeutic footwear and relevant criteria for clinical prescription. Also, this study, through clear terminology and definitions, provides a framework for the development of appropriate mechanical testing methods for off-the-shelf stability therapeutic footwear.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The authors will share the data for this work on request.
Ethics statements
Ethics approval
Staffordshire University Research Ethics Committee. Approval number: LSE:22102019.
Acknowledgments
The authors wish to acknowledge the expertise and time offered in this study by the Delphi panel: Dr Helen Banwell, David Buchanan, Simone Cranage, Frank Crewdson, Nina Davies, Dr Nicola Eddison, Dr Christopher Hovorka, Dr Alicia James, Jason McKellen, William Munro, Steven Osborne, Steven Seccombe, Jonathan Tebbut, Dr Cylie Williams, Douglas Young and Joshua Young.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @AoifeCHealy, @nachic
Contributors All authors equally contributed to the conception and the design of the study. MH completed the data acquisition and analysis, with all authors involved in the interpretation of data. MH was responsible for the original drafting of the work with all authors revising it critically for important intellectual content. All authors had final approval of the version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. NC is the manuscript’s guarantor.
Funding This study was supported by Staffordshire University Research Studentship.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.