Article Text

Abstract
Objectives Identify the proportion of patients attending fracture clinics who had suffered intimate partner violence (IPV) within the past year.
Design Powered cross-sectional study using validated participant self-reported questionnaires.
Setting and participants Adult trauma patients (no gender/age exclusions) attending one of three Scottish adult fracture clinics over 16-month period (from October 2016 to January 2018).
Primary outcome measure Number of participants answering ‘yes’ to the Woman Abuse Screening Tool question: ‘In your current relationship over the past twelve months, has your partner ever abused you physically/emotionally/sexually?’
Results Of 336 respondents, 46% (156/336 known) were women with 65% aged over 40 (212/328 known). The overall prevalence of IPV within the preceding 12 months was 12% 39/336) for both male and female patients. The lifetime prevalence of IPV among respondents was 20% (68/336). 38% of patients who had experienced IPV within the past 12 months had been physically abused (11/29). None of the patients were being seen for an injury caused by abuse. Two-thirds of respondents thought that staff should ask routinely about IPV (55%, 217/336), but only 5% had previously been asked about abuse (18/336).
Conclusions This is the first study worldwide investigating the prevalence of IPV in fracture clinics for both male and female patients. 12-month prevalence of IPV in fracture clinic patients is significant and not affected by gender in this study. Patients appear willing to disclose abuse within this setting and are supportive of staff asking about abuse. This presents an opportunity to identify those at risk within this vulnerable population.
- orthopaedic & trauma surgery
- epidemiology
- social medicine
Data availability statement
Data are available upon reasonable request. Due to the sensitive nature of the raw data and the presumed consent process followed, the authors have decided not to make the raw data for this study publicly available. We are happy to consider requests to access the dataset from individual researchers with appropriate permissions in place.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is an inclusive, multicentre study that is powered to detect 12-month prevalence of intimate partner violence (IPV) in male and female patients within a trauma population in Scotland.
Questionnaires were completed anonymously, which helped to protect participant safety and confidentiality.
The study was designed with significant input from a regional ethics committee and patient and public involvement group, helping to protect and include this vulnerable patient population in research.
Participants were asked whether healthcare staff had ever discussed IPV with them to validate results from a previous study from the perspective of staff in the trauma clinic.
To protect anonymity, no prior screening of clinics was undertaken, and therefore, minimal data on response rates are available.
Key messages
What is already known on this topic:
Intimate partner violence (IPV) is common fracture clinic attenders, with 12-month prevalence rates of 15%–32% in female participants reported in the international literature.14 15
Fracture clinic staff report high rates of asking about abuse (74%, 77/104), but few are trained to deal with a disclosure of IPV.13
No study to date has focused on the IPV rate in male participants in the fracture clinic setting, and this urgently needs to be remedied.
What this study adds:
This study demonstrated that the IPV prevalence in fracture clinic patients was 12% within the past 12 months and had affected 20% of participants within their lifetime.
Rates of abuse were comparable between male and female participants, but a quarter of patients did not feel comfortable disclosing their gender.
Only 5% of respondents had been asked about abuse in this study, which conflicts with previous evidence in the same centres suggesting that staff routinely asked about abuse when suspicious.13
Introduction
Approximately one in three women and one in six men have experienced intimate partner violence (IPV or domestic abuse) during their lives.1 Recent estimates of current abuse (ie, from a current partner within the past 12 months) suggest that IPV can affect 8% of women and 4% of men at any one time.2
Guidance from the National Institute for Clinical Excellence in the UK recommends that it is the role of all frontline healthcare staff to identify and help those experiencing abuse.1 This does not only include those presenting to healthcare with injuries resulting from abuse but also identifying those with risk factors for IPV and providing them with appropriate support and privacy and trained staff to action any disclosures of abuse.
Historically, research has highlighted the role of emergency department (ED) in identifying vulnerable patients and has focused primarily on female patients experiencing IPV.1 3 4 Studies indicate that patients find screening to be acceptable in the acute care setting but that screening should include all patients, including men, and not be seen to ‘select out’ high-risk individuals.4–6 Patients experiencing IPV are more likely to disclose this if they are asked directly,7 and there is some suggestion that disclosure rates are higher with questionnaire-based studies rather than via face-to-face interviews.4 8
However, the majority of patients in the UK are seen and discharged from the ED in under 4 hours, and many victims of abuse never present as an emergency.9 10 Less than a quarter of such patients (24%) feel able to confide about abuse within the ED,7 and an excellent recent review highlighted a lack of privacy and confidentiality around disclosure in this setting.4 Some of the barriers to routine screening by healthcare staff in the ED include lack of experience, lack of time, concerns about the process of asking patients and uncertainty about the benefit of disclosure.11 Many of these barriers can potentially be addressed within other acute secondary care settings.11 12
We believe that the fracture clinic is an ideal site for identifying and helping vulnerable patients at risk of abuse. Not only are these patients likely to sustain a musculoskeletal injury,12 but these clinics provide access to a group of relatively young, fit patients who might not otherwise be involved with healthcare services. This raises the questions of whether patients are willing to disclose abuse in the busy fracture clinic setting and whether staff are equipped to manage such a disclosure.
We previously conducted a national survey of multidisciplinary fracture staff awareness of IPV.13 Staff reported high rates of asking about abuse (72%, 75/104) when suspicious but a low prevalence of routine assessment (2%, 2/104).13 This is commonly seen in the literature in other secondary care settings.4 6
Our study also showed that the majority of orthopaedic staff felt it was important to ask about IPV (74%, 90/121) but had poor knowledge of how to manage a disclosure (24%, 29/121 knew about available support13), which again is a common finding.4 6
IPV in the fracture clinic has been the focus of Canadian and international multicentre studies by Professor Bhandari’s group.14 15 They found a 12-month IPV prevalence of 16%–32% and a lifetime prevalence of 35% among female participants.14 15 These studies have provided comprehensive evidence that patients do appear to be willing to disclose abuse within this setting but have focused mainly on female patients. They also demonstrated that 74% of both male and female respondents in the fracture clinic setting agreed that fracture clinics were an appropriate place for healthcare staff to screen for IPV.16
To compare previous results to a UK population and in order to address the question of IPV prevalence in male IPV patients, we conducted a cross-sectional survey in three Scottish orthopaedic centres. The primary objective was to ascertain the prevalence of IPV among fracture clinic attendees for trauma over the past 12 months in a current relationship (‘current’ IPV). It was hypothesised that 12-month prevalence would be 15%–20% as for a comparable Canadian cohort.14
The secondary objectives were to assess the lifetime prevalence of IPV and to characterise this population in comparison to fracture clinic attendees who were not currently experiencing abuse. We also sought to explore whether there was any difference in frequency or type of IPV for male versus female participants, whether participants had been asked about abuse by staff and whether they thought it was acceptable to ask about IPV in this setting.
Methods
Study design
This was a cross-sectional questionnaire-based study of the prevalence of IPV in patients presenting to orthopaedic fracture clinics at three centres in Scotland, the UK, from October 2016 to January 2018.
Three centres across the country were chosen to provide a broad perspective of IPV in fracture clinic patients. These centres were a large university teaching hospital in Dundee, a district hospital in the affluent city of Perth and a rural hospital in Inverness within the Scottish Highlands.
Recruitment & data collection
Participating clinics were chosen on a non-random basis according to the availability of the research team to provide support to fracture clinic staff should it be required. Data collection took place over the following dates:
Centre 1: Ninewells Hospital (Dundee) from October 2016 to October 2017.
Centre 2: Perth Royal Infirmary (Perth) from January 2017 to January 2018.
Centre 3: Raigmore Hospital (Inverness) from April 2017 to July 2017.
At each participating fracture clinic, all adult patients were given a questionnaire pack on checking into clinic. This pack contained the validated questionnaire (online supplemental figure 1) along with a participant information sheet and information leaflet (online supplemental figure 2) detailing sources of advice and support for victims of IPV. Due to the desire to maintain anonymity in participants and stipulations in ethics committee approval, consent was presumed through completion of the anonymous questionnaire.
Supplemental material
Supplemental material
The questionnaire was a self-reported tool assessing multiple indicators of IPV previously validated in a multicentre study.15 The questionnaire contained several screening tools (the Woman Abuse Screening Tool (WAST) and the Partner Violence Screen)17 18 in addition to general questions about IPV and patient demographics including age, ethnicity, injury and sexual orientation. Participants were asked to describe their gender, and it was left to them to decide whether to identify based on biological or social preference.
The questionnaire pack could be completed and returned within the fracture clinic setting or taken home and returned via prepaid post. It was intended that any risk of coercion would be minimised as any patients who did not want to participate could simply return the blank questionnaire within the sealed envelope without the healthcare team’s knowledge.
Inclusion and exclusion criteria
All adult patients (man and woman) attending and participating fracture clinics were given questionnaire packs and were eligible to participate. During data analysis, respondents were excluded for age less than 18 years old (zero participants) and for a non-trauma-related orthopaedic condition (elective patients, 60 participants). Although not actively excluded, it is likely that patients who would not complete the questionnaire would include those who felt uncomfortable disclosing abuse within the fracture clinic setting, those who found the issue unimportant and those who were unable to read and write in English.
Outcomes
The primary outcome was the combined percentage of participants answering yes to the following question: ‘In your current relationship over the last 12 months, has your partner abused you physically/emotionally/sexually?’ (as per the WAST tool, these were asked as three separate questions). This was taken to indicate current IPV.
Secondary outcome measures included the combined percentage who answered yes to the following question: ‘Have you ever been physically/emotionally/sexually abused by a partner?’ which was taken to indicate lifetime prevalence of IPV. All of the participants who had been abused within the past 12 months also reported that they had been abused within their lifetime with the exception of one, who left the entire second page blank. This has been reported as ‘unanswered’ in the analysis.
Sample size
Based on sample size calculations used in previous studies,14 15 an estimated 12-month IPV prevalence of 15%–20% among fracture clinic attendees was chosen. With a confidence level of 95% and error margins of 4–4.5, a sample size of 183–199 was required. This was rounded up to 250 to compensate for missing data. If true prevalence was much lower than 15%, a sample size of 278 would provide 95% CIs with error margins of 1.58 and was deemed acceptable.
Data analysis and missing data
Descriptive data are reported as frequencies and percentages for categorical variables within the dataset. Parametric data are presented as mean and SD and non-parametric as median and IQR. Where study groups have been directly compared with one another, dataset analysis comprised the χ2 test for categorical variables and Student’s t-test or non-parametric Wilcoxon test as appropriate for continuous variables (significance p<0.05).
Confidentiality
No screening of participant records took place to identify potential participants for the study. Fracture clinic reception staff handed out questionnaire packs to all adult patients attending and participating fracture clinics. Participation was entirely anonymous, with no way of contacting the patient or their general practitioner at a later date. This method was based on stipulations from ethics committee approval.
Regional ethics committee (REC) approval
The initial plan was to interview fracture clinic participants and gain formal consent as per a previous multicentre cross-sectional study recruiting in the USA, Canada and Europe11. The Prevalence of Abuse and Intimate Partner Violence Surgical Evaluation (PRAISE) Study screened fracture clinics for eligible patients and approached them to consider participation in the study when deemed safe to do so. The plan to repeat this method was given an unfavourable opinion at ethics committee review due to the perceived risk of patient harm by an abusive partner discovering that the participant had been selected out and approached for participation in the study. Under support from a second ethics committee, the study was redesigned. Participation was made completely anonymous with all clinic attendees given a questionnaire pack to consider participation without prior screening of clinic lists. A favourable opinion was granted by the North of Scotland REC on 31 August 2016 (Ref.: 16/NS/0078).
Results
Demographics
Between October 2016 and January 2018, 61 clinics were used to hand out 524 questionnaires (figure 1). We are unable to provide details of non-respondents due to ethics committee stipulations, but all 61 clinics included were non-specialist trauma clinics, with even recruitment by weekday and month (see online supplemental figure 3). Three hundred ninety-six completed questionnaires were returned, generating a 76% response rate. Seventy-two out of three hundred ninety-six (18%) questionnaires were returned by post, and of the remainder, there was an uneven spread between the three centres, with 189 returned locally to centre 1 (47%), 27 to centre 2 (7%) and 108 to centre 3 (27%). Although the planned sample size was 280, questionnaire packs were handed out in groups of 50 to participating fracture clinics, and those returned by post underwent some delay in collation and analysis. For this reason, recruitment was concluded at 396 respondents. This initial group included 60 participants who were attending an orthopaedic clinic for an elective condition. These non-trauma patients were excluded from the main analysis but reviewed separately. The final trauma group numbered 336 participants.
Supplemental material

Flow chart summarising study participant identification and demographics.
Of the 336 orthopaedic trauma patients who participated, 46% were women (156/336, table 1). Of the remaining half, 29% were men (99/336), and 24% did not disclose their gender (81/336). There was a range of ages among respondents with almost two-thirds over 40 (63%, 212/336). Sixty-eight percent of participants were currently in a relationship (227/328, eight unanswered, median 16 years and IQR 5–34 years).
Table comparing demographic data for current intimate partner violence (IPV) (12-month IPV) and non-IPV groups
Orthopaedic trauma patient study population
Combined lifetime prevalence of IPV among respondents was 20% (95% CI 16.1% to 24.9%, 68/336, 36 unanswered). Sixty-seven participants had experienced emotional abuse (20%), 37 physical abuse (11%) and 15 sexual abuse (4%, figure 2). Over the previous 12 months, 10% of participants had experienced emotional abuse, 4% physical abuse and 0.6% sexual abuse (34, 12 and 2, respectively, figure 3). The overall current prevalence of IPV violence was 12% (95% CI 8.4% to 15.5%, 39/336, 54 unanswered).

‘Have you ever been physically/emotionally/sexually abused by a partner?’ bar chart showing lifetime prevalence of intimate partner violence in orthopaedic trauma patients. Of 68/336 participants (20%) who disclosed having been abused by a partner at some point in their lives, 67 had experienced emotional abuse (20%), 37 physical abuse (11%) and 15 sexual abuse (4%).

(Over the last 12 months) ‘Has your partner abused you physically/emotionally/sexually?’ bar chart showing 12-month or current prevalence of intimate partner violence in orthopaedic trauma patients (primary aim of study). Thirty-nine out of three hundred thirty-six participants (12%) had been abused by a partner at some point within the past 12 months. Of these, 34 had experienced emotional abuse (10%), 12 physical abuse (4%) and two sexual abuse (0.6%).
Further comparison was made between two groups within the respondents, the ‘12-month IPV’ group (those who had experienced abuse within the past 12 months, 39/336) and the ‘no recent IPV’ group (those who had not experienced abuse within the past 12 months, 243/336) for the following analyses.
IPV study population
Age and gender were comparable between the 12-month IPV and no recent IPV groups, with 42% and 44% female gender (p=0.744) and 62% and 64% aged over 41 (24/39 and 155/243, p=0.797), respectively (table 1). Also comparable between the IPV and non-IPV groups was country of birth, ethnicity, home circumstance, children, education and sexual orientation (NS for all; see table 1). Compared with the non-IPV group, participants in the 12-month IPV group were more likely to describe some tension within their relationships (38%, 15/39, vs 12%, 29/243, p<0.0001) and some difficulty in working out arguments (38%, 15/39, vs 12%, 29/243, p<0.0001). Arguments were more likely to result in hitting, kicking or pushing in the IPV group (10%, 4/39, vs zero in the non-IPV group, p<0.0001), and 4% felt frightened by their partner sometimes or often (23% 9/39 and 0.8%, 2/243, respectively, p<0.0001).
Five percent (18/336) of all participants had previously been asked by healthcare staff about abuse (18%, 7/39, IPV group and 4%, 9/243, non-IPV group, p<0.001, 37 unknown). Both groups felt that it was important to ask patients about abuse on a routine basis (79%, 31/39, and 69%, 168/243, respectively, p=0.355; 65%, 217/336 overall, 39 blank).
Gender analysis
Since gender was undisclosed in a quarter of patients (22%, 75/336), the data for all participants, man and woman, have been presented for the 12-month IPV versus non-IPV group analyses.
There was no significant difference in IPV disclosure rates for lifetime IPV for female versus male patients (22%, 34/156 woman, and 16%,16/99 man, p=0.131, figure 4A). There was also no significant difference in prevalence by gender for 12-month IPV (11%, 17/156, and 10%, 10/99, respectively, p=0.420, figure 4B).
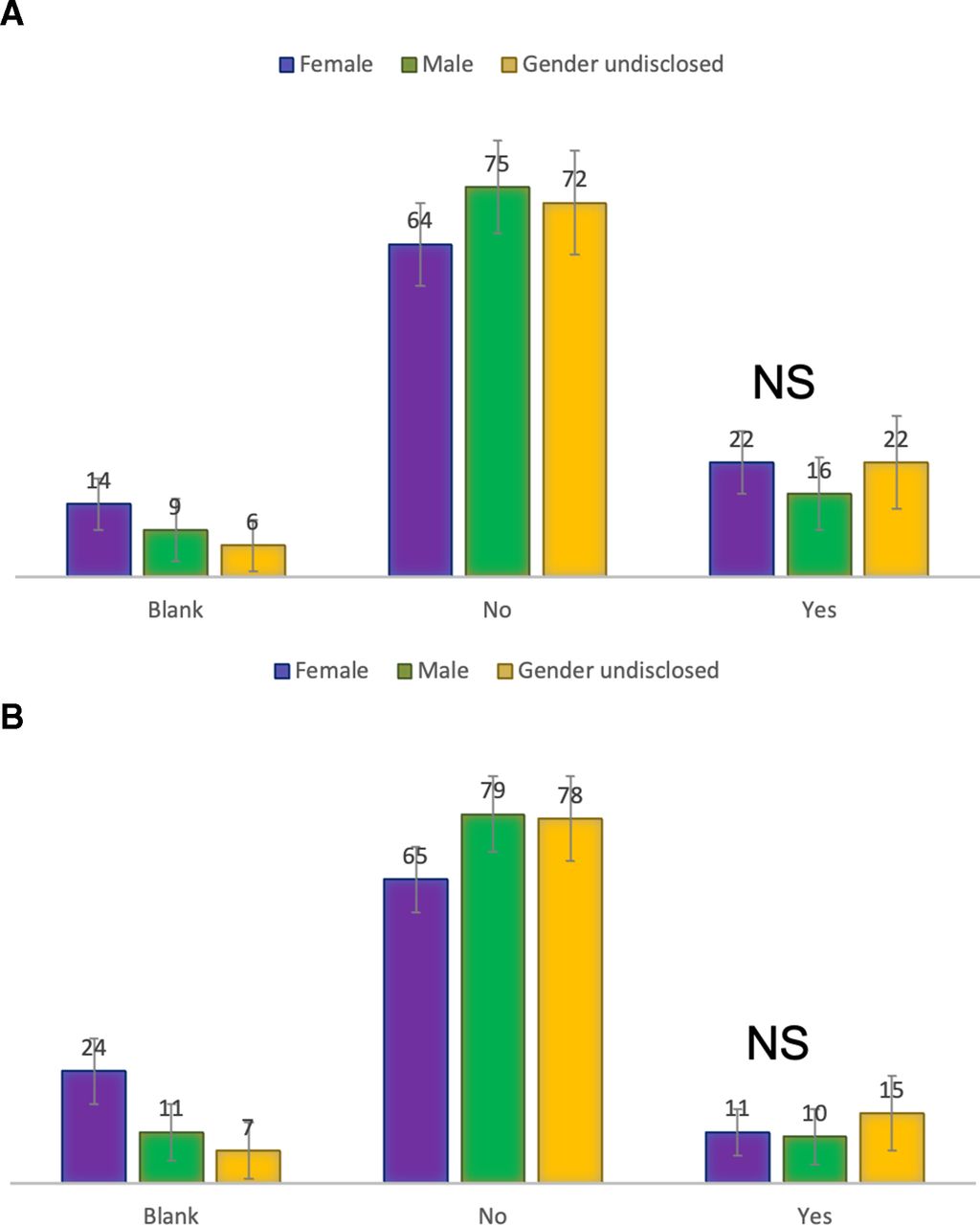
Bar charts demonstrating prevalence of intimate partner violence (IPV) by gender (man, woman or undisclosed). (A) Lifetime prevalence of IPV by gender. There was no significant difference between female and male participants who disclosed previous abuse (22%, 34/156, and 16%, 16/99, respectively, p=0.131, χ2 test). (B) Twelve-month or current prevalence of IPV by gender. There was no significant difference between female and male participants who disclosed current abuse (11%, 17/156, and 10%, 10/99, respectively, p=0.420, χ2 test). NS: ‘not significant’ = p>0.05.
There was no difference in IPV disclosure rates for 12-month IPV for female versus male patients (11%, 17/156, and 10%, 10/99, respectively, p=0.420, figure 4A). There was also no significant difference in prevalence by gender for lifetime IPV (22%, 34/156 woman, and 16%, 16/99 man, p=0.131, figure 4B). Comparison of type of IPV (emotional, physical or sexual) by gender of respondent was made, and female respondents were significantly more likely to have experienced sexual abuse within their lifetime compared with male and gender-undisclosed participants (p=0.027, figure 5A). There were no significant differences in type of IPV by gender for 12-month abuse (figure 5B).

Bar charts demonstrating type of intimate partner violence (IPV) including physical, emotional and sexual abuse by gender (man, woman or undisclosed). (A) Lifetime type of IPV by gender. Female respondents were significantly more likely to report sexual IPV (p=0.027, χ2 test). All genders were equally likely to report physical and emotional IPV (p=0.151 and p=0.992, respectively, χ2 test). (B) Twelve-month type of IPV by gender. There were no significant differences in type of IPV by gender for physical, emotional or sexual IPV (p=0.718, p=0.536 and p=0.673, respectively, χ2 test).
Elective orthopaedic patients
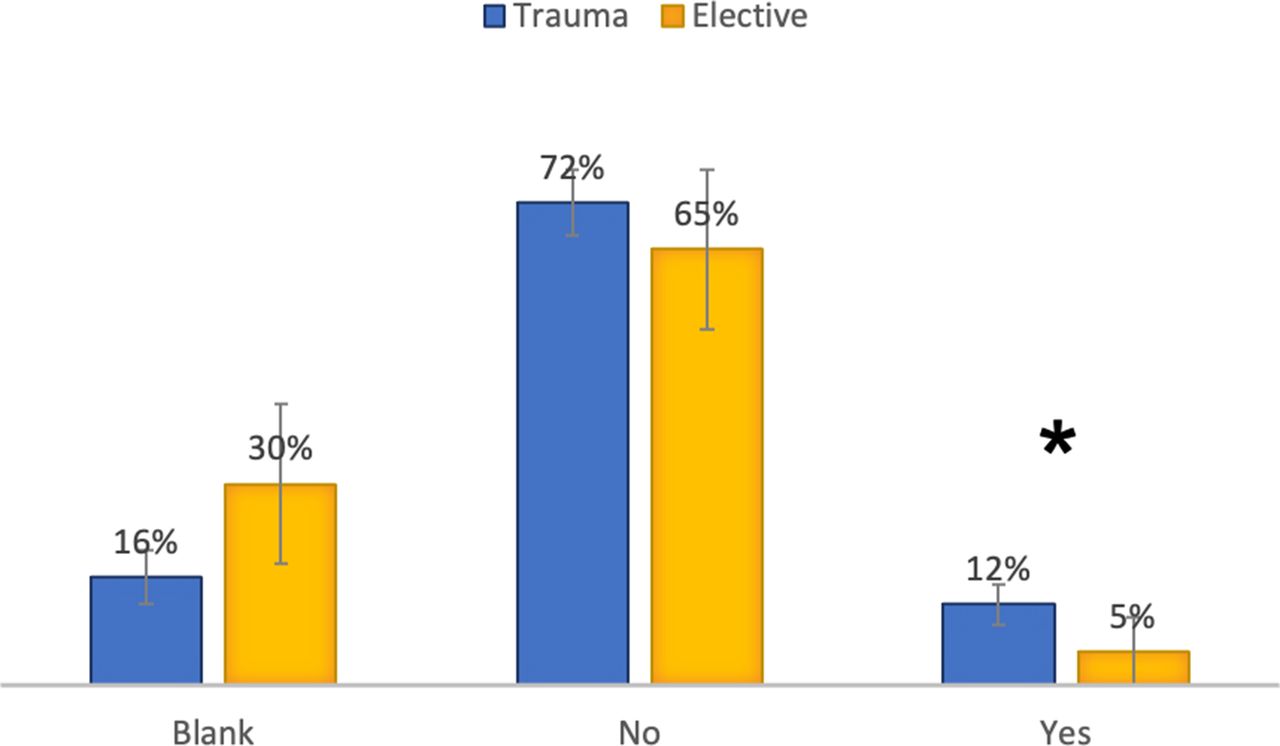
Sixty participants attending for elective conditions with no history of trauma returned completed questionnaires but were analysed separately (see Methods section). Gender was comparable in this group to the trauma group (53% woman, 32/60, and 28% man, 17/60, compared with 61% woman, 156/255 known, and 39% man, 99/255 known, respectively). The elective patients had a higher overall age, with 87% over 40 (52/60) compared with 63% (212/336) in the trauma group. Elective orthopaedic patients had a significantly lower rate of current IPV compared with trauma patients (5%, 3/60, vs 12%, 39/336, p=0.025, figure 6).
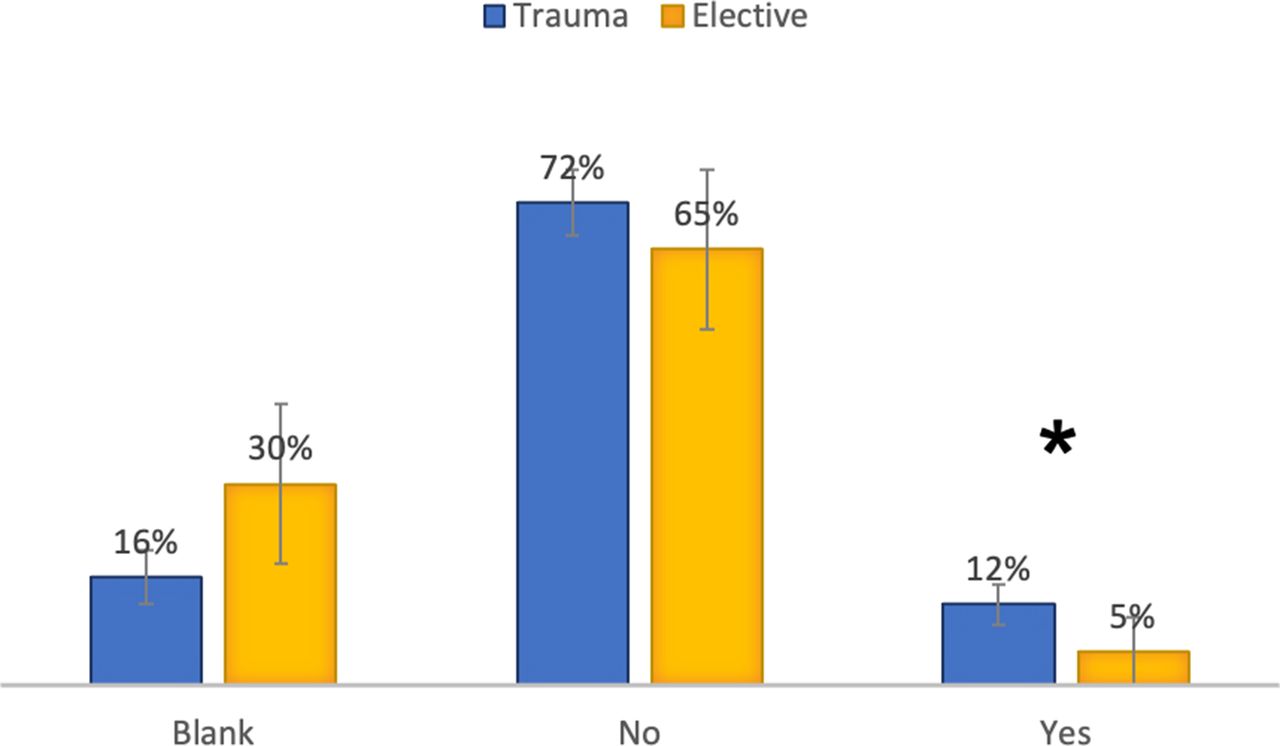
Bar chart showing prevalence of 12-month or current intimate partner violence (IPV) in the group of orthopaedic trauma patients (trauma group) versus a separate group of elective orthopaedic patients (elective group). Participants within the trauma group were more likely to be suffering from current IPV than elective participants (12%, 39/336, and 5%, 3/60, respectively, p=0.025).
Discussion
The 12-month prevalence of IPV among fracture clinic attenders in this study of three Scottish trauma units was 12%, and lifetime prevalence was 20%. Although over a fifth did not disclose their gender, there was no significant difference between rates of current IPV among female and male participants (22% and 16%, respectively) and lifetime IPV (11% and 10%, respectively). The majority of IPV disclosed was emotional abuse, with physical and sexual abuse less likely to be reported, a trend seen in the majority of centres in the PRAISE Multicentre IPV Study15 (table 2 and figure 7). As can be seen from figure 7, the prevalence of IPV within Scotland is comparable to current and lifetime IPV rates in other European countries like Denmark and the Netherlands. The 12% 12-month prevalence of IPV seen in our study is significantly lower than that seen in the USA and earlier Canadian studies (p<0.0001 for both, χ2 test). It should be noted that the difference in recruitment methods used between our study and the PRAISE study should lead to caution in making direct comparisons between prevalence rates of IPV compared with our population. Our response rate of 76% is lower than the 85% reported by the PRAISE investigators,19 which is perhaps unsurprising given the difference in recruitment methods (face-to-face questionnaire in PRAISE compared with anonymous questionnaire completion in this study), but we have already reported evidence that patients may prefer anonymised questionnaire formats in identifying domestic abuse.4 8
Table comparing intimate partner violence (IPV) prevalence across different countries as published by Bhandari et al14 and the Prevalence of Abuse and Intimate Partner Violence Surgical Evaluation investigators15 (female participants only) with the data from this study (female and male participants).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
It should be noted that the WAST screening tool used in this study identifies abuse in somewhat general terms (see online supplemental figure 1). It is possible that participants could answer yes to some of the questions and be incorrectly identified as suffering from abuse, particularly emotional abuse. However, we used the question ‘has your partner abused you physically/emotionally/sexually’, which will allow the participants to determine whether they are being subjected to IPV or not.
The gender spread and trend towards age over 40 in our participant population were comparable to the general fracture population within the UK.20 This allows us some confidence in extrapolating our results to the general fracture clinic population, within the limits of the lack of data on response rates, which was a limitation of the study design (see Limitations and future work section).
None of the injuries in this study were due to IPV, despite the relatively high prevalence of current abuse within the group. This may reflect the high rates of emotional abuse and low rates of physical abuse disclosed by participants and is supported by the literature, which suggests that rates of physical and sexual violence are higher in female victims of IPV (compared with heterosexual male victims) but that rates of emotional, coercive and controlling abuse appear to be equally prevalent and may even be more commonly reported by male victims14.
The final aim was to establish whether, as reported in our previous study,13 orthopaedic staff ask trauma patients about IPV and whether they are educated and equipped to manage a disclosure of abuse. In the current study, only 5% of our participants reported having been asked about IPV by healthcare staff, although 59% felt that it was important to ask about abuse routinely. It is worth noting that in a questionnaire where a large number of questions were left blank by participants (see table 1), the response rate for these two questions was very high at 97%.
Low rates of healthcare staff enquiry about abuse are well documented, reported by 16% of abused participants within the Canadian IPV Study and 14% in the PRAISE trial.14 15 It is clear that if staff are not routinely asking about abuse (even in patients who are suffering from IPV), this will translate to fewer at-risk patients being identified and a missed opportunity for helping this vulnerable group. In a study of prevalence of IPV in ED trauma clinics, of the 12% of participants who disclosed abuse within this setting, two-thirds (63%) were sent home without a safety assessment and 79% without input from social services.21
The justification for orthopaedic fracture clinics as a potential site for identifying and intervening in the care of these patients has been well established.9 13 22 Evidence from this study and previous studies does seem to suggest that patients are willing to disclose abuse within this setting, but previous work suggests that up to 50% of patients would not make a disclosure unless asked directly in the presence of a physician or senior healthcare staff member.7 14
This is the first study worldwide to investigate the prevalence of IPV among male orthopaedic trauma patients. The large number of participants who did not disclose their gender (22%) suggests there is ongoing difficulty in admitting to domestic violence in relation to gender, and we have chosen to analyse participants en masse to avoid unfair exclusion of this large group of participants whose gender is undisclosed. In this study, we found no significant difference in 12-month or lifetime prevalence between male or female participants. It is unknown whether the reasons for non-disclosure of IPV (and, indeed, gender in this study) vary between male and female patients. It is possible that a number of participants chose to leave this section blank as they did not identify as male or female, and it is important to recognise that the reported rate of IPV is high among transgender individuals.23 Future work should incorporate patient feedback, explicitly including male and female patients, regarding barriers to disclosure of abuse within the secondary care setting.22
Finally, we chose to focus on the fracture clinic population for this prevalence study to provide insight on IPV in a population of young, otherwise fit patients who might not otherwise present to healthcare services on a regular basis. For this reason, the 60 participants with elective orthopaedic conditions were excluded from the primary analysis. Although not formally powered, the elective subgroup analysis did demonstrate a population of orthopaedic patients with a higher average age and lower rate of IPV compared with trauma patients (5% and 12% 12-month IPV prevalence, respectively, p<0.0001, χ2 test).
Limitations and future work
There is the risk of selection bias in the study group due to recruitment through orthopaedic fracture clinics, which tend to see patients who are younger and fitter than the general population.20 24 The current and lifetime IPV prevalence reported in this paper should be considered therefore to apply to the Scottish fracture clinic population, and caution should be used in applying this to the general public.
In addition, this study contains limited data on response rates and composition of participating fracture clinics due to restrictions placed by the ethics committee during review for the purposes of protecting the safety of vulnerable participants. It is therefore not within the scope of this study to comment on how many patients given the anonymous questionnaire packs were willing to complete these within the setting, and we can only comment on the responses received. It is possible that the results are subject to selection bias (patients who do not consider the issue important/relevant to them may not participate) or that patients who are being abused are less likely to participate due to fear of their abuser finding out. If this is the case, then the true prevalence of IPV may be much higher than that reported in this study.
Participants within the 12-month IPV group were more likely to have been asked by healthcare staff about abuse than the non-IPV group (18% and 4%, respectively). Although this may reflect recall bias, published evidence does suggest that healthcare staff are more likely to enquire about abuse in those deemed at high risk.4 13 22 However, there is an increasing call for routine enquiry when screening for abuse to occur in acute situations like the fracture clinic to identify those suffering from occult or ‘incidental abuse’ (not related to the current presentation).25 Indeed, none of the 39 participants currently being abused in this study had presented with an injury related to abuse, and many would likely be considered ‘low risk’ by staff. We would recommend that staff in acute settings (such as trauma) should consider enquiring about abuse in every patient on a routine basis to reduce stigma, identify occult cases and increase healthcare staff awareness on this vital topic.25
It should be noted that this study covers IPV exclusively, without covering other methods of domestic violence such as abuse by a family member. The questionnaire used in this study was designed to detect IPV only, but any healthcare staff education should cover other types of domestic violence to maximise the number of vulnerable populations that can be identified by an increased rate of awareness of this issue.
Finally, it should be noted that this study was not powered to detect lifetime prevalence of IPV. With estimated lifetime rates of 16%–53% in the literature,14 15 a significantly larger sample size (approximately 700–1000 participants) would be required to power such a study. As such, our lifetime IPV prevalence should be considered as the basis for future work to validate this estimate. In addition, the current study is not powered to investigate the role of patient characteristics (eg, gender and education) in identifying those at increased risk of abuse via multivariate analysis. This again is not the objective of this study as the increasing emphasis in the literature is to screen all patients including those perceived to be at ‘low risk’ (such as male patients) in an effort to improve rates of identification; reduce stigma; and prevent rare, significant complications such as significant injury and murder.4 5
Implications
In summary, IPV was common in the three orthopaedic fracture clinics who participated in this study, with a 12% 12-month and 20% lifetime prevalence. Although the true rate of IPV may be much higher, patients do appear to be willing to make a disclosure of abuse within this setting. Rates of abuse were not significantly different between male and female participants, but a quarter of patients did not feel comfortable disclosing their gender.
Despite 74% of orthopaedic healthcare staff reporting that they would ask about abuse in trauma patients,13 only 5% of patients overall report having been asked about abuse in this study.
Evidence from the literature and this study suggests that the orthopaedic fracture clinic is an appropriate place to identify those at risk of abuse, and we would recommend that training needs to be made available to ensure that healthcare staff know the benefits of routine enquiry and are equipped to manage a disclosure of IPV. In addition, it is vital that screening does not just involve staff ‘just asking the questions’ but about creating a supportive environment where patients can disclose safely and staff are adequately trained to support individuals.26–28
Future work should focus on whether increased awareness and better training can lead to increased rates of abuse identification, better care and reduced risk to this vulnerable group. We do not wish to add to the work of busy fracture clinics, but with a lifetime prevalence of one in five and a current prevalence of one in eight in both men and women, our staff need to at least be aware of this issue and how to manage it.
Data availability statement
Data are available upon reasonable request. Due to the sensitive nature of the raw data and the presumed consent process followed, the authors have decided not to make the raw data for this study publicly available. We are happy to consider requests to access the dataset from individual researchers with appropriate permissions in place.
Ethics statements
Ethics approval
North of Scotland Research Ethics Service 16/NS/0078 IRAS Project ID 167864.
Acknowledgments
The authors would like to thank the members of the intimate partner violence advisory group for their input into the planning stages of this project: Jenna Breckenridge, Fiona Duncan and Cheryl Sutherland Stewart. We would also like to thank the North of Scotland Research Ethics Committee for their support in the redesign of this study: without their valued input and advice, this study could never have been completed.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SD: conceptualisation, methodology, formal analysis and writing and original draft preparation. IK: Data collection, writing and reviewing and editing. KM: methodology, data analysis, writing and reviewing and editing. MB: methodology, writing and reviewing, editing, and supervision. AJ: conceptualisation, methodology, writing and reviewing, editing, and supervision.
Funding The authors gratefully acknowledge research grants from AO UK (2016) and the Bridge of Earn Trust (2016) without which this project could not have been completed. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf, and the authors had financial support from AO UK and the Bridge of Earn Trust for the submitted work, no financial relationships with any organisations that might have an interest in the submitted work in the previous three years and no other relationships or activities that could appear to have influenced the submitted work.
Patient and public involvement statement The final protocol was approved by a study advisory group comprising a gender-based violence nurse advisor, doctoral researcher in intimate partner violence and research manager with Scottish Women’s Aid.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.