Article Text

Abstract
Objective This study sought to investigate the joint effect of household cooking fuel type and urbanicity (rural–urban residency) on anaemia among children under the age of five in sub-Saharan Africa.
Design We analysed cross-sectional data of 123, 186 children under the age of five from 29 sub-Saharan African countries gathered between 2010 and 2019 by the Demographic and Health Survey programme. Bivariate (χ2 test of independence) and multilevel logistic regression were used to examine the effect of urbanicity-household cooking fuel type on childhood anaemia. Results were reported as adjusted odds ratios (aORs) with 95% CIs at p<0.05.
Outcome measures Anaemia status of children.
Results More than half (64%) of children had anaemia. The percentage of children who suffered from anaemia was high in those born to mothers in Western Africa (75%) and low among those born in Southern Africa (54%). Children from rural households that depend on unclean cooking fuels (aOR=1.120; 95% CI 1.033 to 1.214) and rural households that depend on clean cooking fuels (aOR=1.256; 95% CI 1.080 to 1.460) were more likely to be anaemic as compared with children from urban households using clean cooking fuel. Child’s age, sex of child, birth order, perceived birth size, age of mother, body mass index of mother, education, marital status, employment status, antenatal care, wealth quintile, household size, access to electricity, type of toilet facility, source of drinking water and geographic region had significant associations with childhood anaemia status.
Conclusions Our study has established a joint effect of type of household cooking fuel and urbanicity on anaemia among children under the age of five in sub-Saharan Africa. It is therefore critical to promote the usage of clean cooking fuels among households and women in rural areas. These should be done taking into consideration the significant child, maternal, household, and contextual factors identified in this study.
- anaemia
- public health
- community child health
Data availability statement
Data are available in a public, open access repository. Data for this study were sourced from Demographic and Health surveys (DHS) and available here: http://dhsprogram.com/data/available-datasets.cfm.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The major strength of this study is the use of recent nationally representative surveys, with relatively large sample sizes. This makes the findings generalisable to all under-five children in the countries we included in our study.
Also, we employed rigorous statistical modelling to assess the effect of urbanicity-type of cooking fuel on childhood anaemia while controlling for theoretical and practical confounders.
The study, however, is limited by the cross-sectional nature of the design employed for the data collection. Due to this, it is impossible to detect temporality of sequence.
Considering that several proximal, intermediate and distal factors could moderate the effects of household cooking fuel type and urbanicity on child anaemia, we acknowledge that those considered in this study are not exhaustive. Based on data availability, practical relevance and parsimony, the variables included in this study were chosen.
Introduction
In low/middle-income countries (LMICs), anaemia remains a major public health problem which causes childhood mortality and morbidity.1 Anaemia is a condition in which the haemoglobin (Hb) level is lower than the body’s required amount for physiological activities.2 According to WHO,3 about 273.2 million children suffer from anaemia globally with a general prevalence of 42.6%. However, its effects are disproportionate across regions, with sub-Saharan Africa (SSA) being one of the most affected with a startling prevalence rate of 62.3%.4
Anaemia is a major contributor to some of the serious adverse health conditions in children and affects their cognitive, behavioural and physical development.3 5–7 The notable causes of anaemia in children are multifactorial and include deficiency of iron, and other micronutrients such as folate, vitamin B12 and vitamin A; malaria, HIV and chronic diseases such as sickle cell disease.8
Apart from these causes, a major environmental cause of anaemia is indoor air pollution as a result of biomass fuel use in cooking in households.9 Household biomass fuel is a global air pollution issue that harms human health, the climate and the environment. About 3 billion people use biomass fuels such as plant residues, animal dung, wood and charcoal for daily domestic use.10 Inefficient combustion of these fuels could release harmful gases such as sulphur dioxide (SO2), carbon monoxide (CO), nitrogen dioxide (NO2), and particulate matter (PM).11 12 According to WHO,13 households that use biomass fuels are often exposed to peak indoor particulate matter (PM10) levels greater than the air quality guidelines. The mechanism by which biomass fuels use could contribute to childhood anaemia are unknown. However, it has been postulated by Accinelli et al14 that biomass fuel exposure causes lung inflammation with elevated levels of interleukin 6 (IL-6), which produces in the liver hepcidin, a negative regulator of iron stores. However, studies have shown that biomass fuel expels high carbon monoxide levels which bind with Hb, form carboxyhaemoglobin and reduce the level of Hb in the blood, which could lead to functional anaemia, with an adequate Hb level. For instance, studies in India9 and Swaziland11 found the prevalence of anaemia to be significantly high among children in households that rely on biomass fuels for cooking.
Apart from anaemia, evidence of other adverse health outcomes spanning respiratory illnesses, cancer and eye problems from indoor air pollution due to inefficient burning of biomass fuels for cooking in poorly ventilated settings exist.15–17 A majority of the burden is suffered by women who by custom are responsible for cooking and other household chores, and their children, especially, those below the age of 5.17 18 The prevalence of the burden is relatively low in urban areas where clean fuels like liquefied petroleum gas or natural gas and electricity are typically used. However, most rural residents mainly depend on biomass fuels.19 These fuels include among others wood, animal dung, twigs, and dry leaves, and crop residues such as straw and rice husks.20 The high burden of adverse health outcomes among rural residents is that most of them often depend on unclean cooking fuels.16 21 22
The associations between household biomass fuel use in cooking and important health variables of women and children such as adverse pregnancy outcomes (low birth weight, stillbirth)15 23 women health (body mass index (BMI), anaemia),15 24 and the health of children under 5 years of age (child weight, child anaemia)16 23 have been examined. Few studies have examined the association between household biomass fuel use, a notable source of indoor air pollution in LMICs and childhood anaemia in SSA. Further, critical to our understanding but absent in such subregional analysis by studies is the joint impact of household biomass fuel use and urbanicity on child anaemia in SSA. This study, therefore, investigated the joint effect of household biomass fuel use for cooking and urbanicity on anaemia among children under the age of five in SSA.
Methods
Data and sampling
Nationally representative data from the Demographic and Health Surveys (DHS) Program for 29 countries in SSA from 2010 to 2019 were acquired for analysis in this study. The DHS Program provides large secondary data gathered from surveys using probability sampling methods, following standard protocols that are internationally accepted. Different sets of questionnaires designed and pretested to ensure reliability and amenability for comparison of data gathered on various spatial and temporal scales are used in the survey. Some questionnaires the Program uses include the ‘children’s questionnaire’ ‘mother’s questionnaire’, ‘men’s questionnaire’ and ‘household questionnaire’. These questionnaires cover a broad range of variables cutting across demographics and anthropometrics, water and sanitation, health, wealth, nutrition among others. The Program recruits and trains field officers to collect accurate data and measurement of weight, height, anaemia using recommended guidelines and instruments. Data on other important variables such as household cooking fuel, urbanicity, wealth, water and sanitation are taken at the household level. The dataset used in this study are: Children’s Data—Children’s Recode, and Household Data—Household Recode (variable names: caseid; v000; v001 v007; v013; v102; v113; v116; v136; v149; v151; v152; v190; bord; b4; b8; m19; hw2; v457; v005; hhid; hv001, hv000; hv226).
Study countries
A sample of 123, 182 was drawn from 29 countries (figure 1) accros the five geographic regions—Western, Eastern, Central and Southern Africa in SSA. For a country to be selected, it must meet the following criteria: should be found in SSA based on the United Nations regional groupings; it must have a DHS dataset with standardised questions and observations on anaemia level of children under 5 years as well as household cooking fuel type, urbanicity, source of drinking water and type of toilet facility. Where multiple datasets exist for a country, the most recent dataset is used.
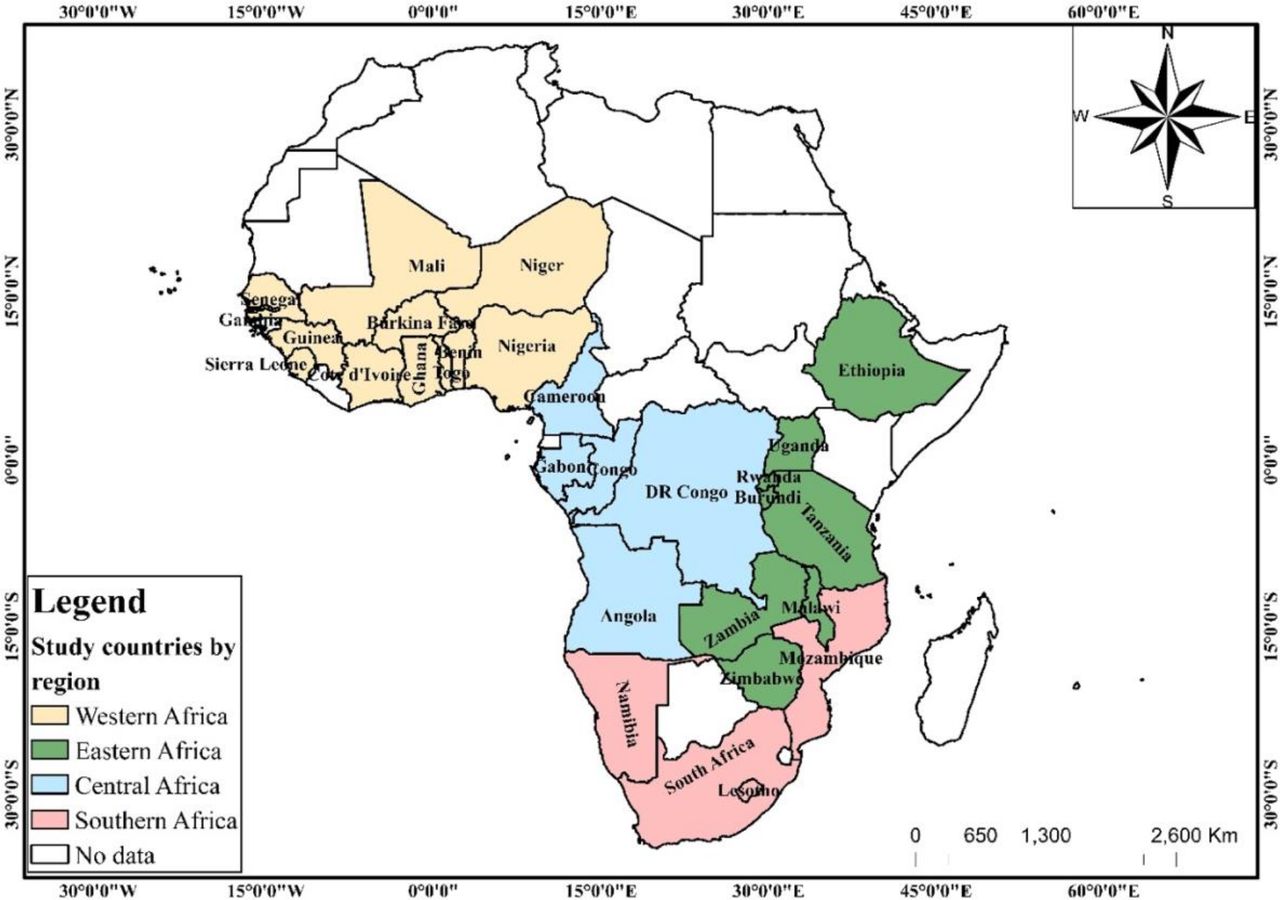
Map of study countries.
Definition of important variables
The dataset provided information on household cooking fuel type, source of drinking water and toilet facility type at the household level. The observations for household cooking fuel were classified into ‘clean’ and ‘unclean’ (polluting fuels) following the criteria used in previous studies25 26 (see table 1). The weight of the child at birth named as ‘birth weight’ was categorised as ‘underweight’ (<2.5 kg) and ‘normal’ (≥2.5 kg) (see Yaya et al27). Also, the observations for the household source of drinking water and type of toilet facility were classified into ‘improved’ and ‘unimproved’ using the revised definitions by the WHO/UNICEF Joint Monitoring Programme report.28 The improved and unimproved drinking water sources and toilet facilities categorisation as described by Armah et al29 are summarised in Table 2.
Classification of the source of drinking water and toilet facilities under the WHO/UNICEF Joint Monitoring Programme and cooking fuel
Distribution of child anaemia status by predictor variables
Measures
Outcome variable
Anaemia status of children is the outcome variable considered in this study. According to DHS, the anaemia status of living children within the age bracket 0–4 years before the survey night was taken. It has its responses classified into four categories according to the WHO recommendation as (i) ‘not anaemic’ for children with Hb count (g/L) measuring above 110 g/L; (ii) ‘mild anaemia’ for Hb count of 100–109 g/L; (iii) ‘moderate anaemia’ for Hb count between 70 and 99 g/L and (iv) ‘severe anaemia’ for Hb count less than 70 g/L. Children with no observations for anaemia count (not tested) and those whose mothers were not listed in the household questionnaire were excluded. Observations under mild, moderate and severe were combined and recoded as ‘1’ for ‘anaemic’ and observations under not anaemic was recoded as ‘0’ ‘normal’ (see Chandran and Kirby30). This produced the dichotomous outcome variable ‘anaemia status’.
Main predictor variable
The predictor chosen for this study is a composite variable derived from household cooking fuel type and urbanicity. The selection of the predictor variable was based on parsimony, literature review, theoretical relevance as well as practical significance. Household cooking fuel type and urbanicity both had two categories since the former was classified as ‘clean’ and ‘unclean’ and the latter measured as ‘rural’ and ‘urban’ per the DHS. This, therefore, gave four mutually exclusive groups: unclean-urban (households relying on ‘unclean’ cooking fuel and found in urban areas); unclean-rural (households relying on ‘unclean’ cooking fuel and found in rural areas); clean-urban (households using ‘clean’ cooking fuels and found in urban areas) and clean-rural (households using ‘clean’ cooking fuels and found in rural areas). This variable combination technique has been widely applied in previous studies.29 31 Out of the four responses, ‘clean-urban’ was chosen as the reference category in the models. Even though urban residents are commonly exposed to outdoor pollution, emissions from household cooking fuels (indoor pollution) is a major problem to rural residents owing to their relatively high dependence on unclean cooking fuels32 33 This formed the basis for the choice of reference category.
Covariates
There is a plethora of evidence on the independent associations between the type of household cooking fuel and urbanicity with childhood anaemia.14 22 33–35 Even though the UNICEF categorisation of the factors that influence the association between household cooking fuel and child anaemia—proximal, immediate and distal factors serves as a useful framework, for parsimony, practical and theoretical considerations, we categorise independent variables drawn from literature under ‘individual-level characteristics’, ‘household characteristics’ and ‘contextual factors’ (see Nambiema et al4 and Amadu et al36). The individual-level characteristics considered in this study are child age in years (0, 1, 2, 3 and 4); sex of child (male, female); birth order (1, 2, 3 and above); perceived birth size (larger than average, average, smaller than average, don’t know); birth weight (underweight, normal); age of the mother (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49); body mass index (BMI) of the mother (thin, normal and obese); education (no formal, primary, secondary and tertiary); marital status (never married, married, living with a partner, widowed/divorced/separated); employment status (no, yes); number of antenatal care (ANC) by mother (no, yes); and number of postnatal care (PNC) by mother (no, yes).
The relevant household-level factors included in this study are wealth status (poor, middle, rich); household size (‘small’ for those with 1–5 members; ‘medium’ 5–10 members and ‘large’ for more than 10 members); age of household head (‘young-aged adults’ for those age below 35; ‘middle-aged adults’ for those between 35 and 64 years and ‘old-aged adults’ for those 65 years and above); sex of household head (male, female); access to electricity (no, yes); type of toilet facility (improved, unimproved); and source of drinking water (improved, unimproved).
Finally, we adjusted for the effect of the contextual factor ‘geographic region’ (Western Africa, Eastern Africa, Central Africa, Southern Africa). Variables in this category of factors relate to the attributes of respondent’s neighbourhood, and opportunities and services that are space-bound.37 38
Data analyses
The Stata V.14.0 MP (Stata Corporation) software was used for the analysis of data. The data were first declared as a survey dataset to prevent potential errors that could arise from the complex survey design using the ‘svyset’ command with the cluster, weighting and strata variables. To understand the distribution of childhood anaemia and the influence of predictive factors on anaemia, descriptive analysis was performed. Using ArcGIS V.10.6, the data were integrated with ESRI Shapefiles to construct a map of the study countries showing the distribution of childhood anaemia. We then determined the associations between the anaemia status of children under five and the relevant predictors using the χ2 test of independence. These relationships were further examined by implementing five multilevel logistic regression models. The first model (model 0) with no independent variable indicated the variance in child anaemia as a result of clustering of the primary sampling units. In model I, only the main predictor variable (urbanicity-type of cooking fuel) was included. Model II adjusted for the individual-level characteristics. The effects of both individual-level and the relevant household-level factors were adjusted in model III. Model IV controlled the individual-level and household-level characteristics, and the contextual-level factors. The Akaike’s Information Criterion was the model comparison metric estimated. Results were presented using adjusted ORs (aORs) at p<0.05 and 95% CIs.
Patient and public involvement
Patients and the public were not involved in the design and conduct of this research.
Results
Descriptive analysis
The study included 123, 182 children under the age of 5 years from 29 countries in SSA. The percentage of children who suffered anaemia was 64%. The prevalence of anaemia was high in children born to mothers in Western Africa (75%) and low among those born in Southern Africa (54%) (figure 2). A majority (68%) of the children included in the survey were in rural households that used unclean cooking fuels, 24% were aged 1, 51% were male, 48% were of second birth order and 50% were of average size at birth. Most of the children included in the survey were born to mothers aged 25–29 (27%), mothers with normal BMI (67%), mothers with no formal education (40%), married mothers (72%), employed mothers (64%), mothers who attended ANC (91%) and mothers who did not attend PNC (56%). A majority of the children belonged to poor households (45%), households with medium size (46%), households with middle-aged adults heads (44%), households with male heads (81%), households with no access to electricity (70%), households with an unimproved toilet facility (56%) and households with improved drinking water (65%). Most of the children included in the study were in Western Africa (40%) and Eastern Africa (40%). Significant differences in the distribution of anaemia status were found in all the in-predictor variables, except PNC attendance (table 2).

{kind=link}
{kind=link}
Map of study countries showing the distribution of children under age 5 years anaemia status.
Multivariate analysis
Table 3 shows the multilevel logistic regression results on the joint effect of urbanicity and type of household cooking fuel on childhood anaemia in SSA. In model IV, the final model that controlled for all the variables including georaphic region, it was found that children from rural households that depend on unclean cooking fuels (aOR=1.120; 95% CI 1.033 to 1.214) and rural households that depend on clean cooking fuels (aOR=1.256; 95% CI 1.080 to 1.460) were more likely to be anaemic as compared with children from urban households using clean cooking fuel.
Multilevel logistic regression results on the joint effect of urbanicity and type of household cooking fuel on childhood anaemia
The odds of childhood anaemia decreased with the age of the child. It was found that children aged 4 had the lowest odds (aOR=0.264; 95% CI 0.247 to 0.283) of suffering from anaemia compared with those less than 1 year (0). Female children were less likely to be anaemic compared with male children (aOR=0.857; 95% CI 0.829 to 0.887). Children with three or more birth orders were more likely to be anaemic compared with first birth order children (aOR=1.269; 95% CI 1.179 to 1.367). Children with smaller than average birth size were more likely to be anaemic compared with those who were larger than average (aOR=1.075; 95% CI 1.020 to 1.132).
The odds of anaemia in children under five were lower among those born to mothers aged 45–49 compared with those aged 15–19 (aOR=0.559; 95% CI 0.484 to 0.645). Children born to mothers with normal BMI were less likely to be anaemic compared with born to children with thin mothers (aOR=0.923; 95% CI 0.870 to 0.979). Children born to mothers with tertiary educational level were less likely to be anaemic compared with those whose mothers had no formal education (aOR=0.534; 95% CI 0.480 to 0.595). Children born to widowed/divorced/separated mothers were more likely to be anaemic compared with those who were never married (aOR=1.102; 95% CI 1.003 to 1.211). Children born to mothers who attended ANC were less likely to be anaemic compared with those who never attended ANC (aOR=0.931; 95% CI 0.874 to 0.991).
The odds of anaemia in children under five was lower among children born to mothers in rich households compared with those born to mothers in poor households (aOR=0.888; 95% CI 0.844 to 0.935). Children born to mothers in larger households were more likely to be anaemic compared with those born to mothers in small households (aOR=1.240; 95% CI 1.163 to 1.321). Children born to mothers in households with access to electricity were less likely to be anaemic compared with those born to mothers in household without access to electricity (aOR=0.896; 95% CI 0.853 to 0.941). Children born to mothers who lived in households with improved source of drinking water were less likely to be anaemic compared with those born to mothers who lived in households with unimproved source of drinking water (aOR=1.046; 95% CI 1.008 to 1.086). Compared with children born to mothers who live in Western Africa, those born to mothers who live in Southern Africa were less likely to be anaemic (aOR=0.497; 95% CI 0.451 to 0.548) (see table 3).
Discussion
In this current study, our principal aim was to investigate the joint effect of household cooking fuel use and urbanicity on anaemia among children under the age of five in SSA. The study showed that children from rural households that depended on unclean cooking fuels were more likely to be anaemic compared with children from urban households using clean cooking fuel. This is in line with previous studies in various parts of the world such as Timor-Leste21 and India.16 22 Although this study was cross-sectional and could not claim causality, some studies16 have explained that exposure to unclean cooking fuels may lead to systemic inflammation which is regarded as a popular cause of anaemia, mediated by inflammatory cytokines such as tumour necrosis factor-alpha, IL-1, IL-6 and interferon-γ.16 39 The pathways by which these causes anaemia is that IL-6 increases with alveolus inflammation related to biomass pollution and hepcidin goes down, that stops the movement of Fe, causing anaemia by inflammation.16 39 Apart from the key independent variable, we controlled for other key factors associated with anaemia among children under five which are worth discussing in light of previous evidence.
We found that the birth weight of the child had a statistically significant association with anaemia. Specifically, children with normal weight had lower odds of being anaemic compared with underweight children. This aligns with previous studies in Ethiopia40 and Brazil.41 Some previous studies espoused that there is a direct link between food consumption and anaemia. Due to this, in a household where there is no food security, it can affect the nutritional status of children, which could contribute to anaemia.42 43 Relatedly, we found that children in large households had higher odds of suffering from anaemia compared with those in a small household. This finding confirms a previous study in Ethiopia.44 Insufficient consumption of appropriate quantity of nutrients due to the high numbers in the households could possibly account for this observation as explained by Asresie et al.44
The study also established that the socioeconomic status (education and wealth) of women had a statistically significant association with childhood anaemia. Specifically, it was found that children whose mothers are in the rich wealth status, as well as those with tertiary level of education, have lower odds of being anaemic. This corroborates several previous studies in SSA and other countries such as Brazil,45 Switzerland,46 Myanmar (Burma)47 and India.48 There are three pathways to the explanation of this finding. First, on the supply side, children from households with high-socio economic status can buy nutritious foods for their children, unlike the poor ones who might not be able to afford three square meals a day. In other words, the poor might lack the resources to purchase nutritious foods for their children. Second, evidence also suggests that mothers in poor households are also anaemic and the probability of their children also being anaemic is high. Third, in terms of education, mothers who are highly educated can translate the health education they receive during child welfare clinics into practice. Besides, those who are highly educated can recognise danger signs related to childhood illnesses that warrant emergency care.44 49
Another major finding in our study was that the odds of suffering from anaemia decreased with the age of the child. This finding is supported by other studies conducted in Ethiopia,40 42 50 51 Ghana52 and Uganda.53 This observation is expected due to the fact that children have their least Hb value at 6 months and they continue increasing their values as they age.54 We also observed a statistically significant association between maternal age and child’s anaemia. Specifically, children whose mothers are aged 45–49 and those aged 30–34 had the lowest odds of being anaemic. This is consistent with previous studies in Ethiopia.44 It is possible that as mothers advance in age, they gain experiences with childcare and also, they are more likely to be exposed to education on appropriate practices on childhood nutrition compared with those who are adolescents. In line with a previous study,55 we also found that children in female-headed households, middle-aged adults, old age adults were more likely to be anaemic compared with those in male-headed households; and households headed by young adults. Surprisingly, our study showed that children in households with an improved source of drinking water had higher odds of being anaemic. This is contrary to other empirical studies in Bangladesh,56 India,22 Benin and Mali.57 Longitudinal case–control studies coupled with qualitative evidence are needed to unravel this counter-intuitive finding.
It is worthy to discuss the methodological limitations inherent in this study. First, although we controlled for several confounders, we could only control for those that were in the datasets. Second, various contextual issues could possibly explain the results we obtained from this study, nonetheless, we used multi-level analysis to account for the contextual variations. The study is also limited by the cross-sectional nature of the design employed for the data collection. Due to this, it is impossible to detect the temporality of sequence.58 There is also the possibility of error in measurement of the Hb levels, however, this is likely to be minimal since DHS uses standardised instruments across surveys and also uses experienced and well-trained data collectors. We did not also control for the dietary pattern and nutritional intake because the data are available for only children aged 6–23 months. In addition, we did not control for child’s fever, diarrhoea and acute respiratory infection with anaemia since there are variations in the context, year and season of data collection across the surveys.58 59
Conclusion
Our study found a joint effect of household cooking fuel and urbanicity on anaemia among children under the age of five in SSA. Apart from this, we also found that birth weight of the child, age of the child, maternal age, sex of household head, age of household head, maternal education, wealth status, size of household, type of source of drinking water and country of residence are associated with childhood anaemia. The following recommendations are therefore made for policy and practice. First, it is critical to promote clean fuel usage among households and women in rural areas. This could be done by governments in various countries by enhancing access and subsidising the cost of natural and or, liquified petroleum gas and cylinders. It is, therefore, imperative to also improve road networks which can easily lead to accessible markets. Second, it is also important to advocate for improvement in female education which could lead to an improvement in the socioeconomic status of women. Third, there is the need for the installation of improved biomass stoves. Also, maternal education by community health nurses on the risk factors of anaemia is also strongly suggested. Stakeholders that seek to improve maternal and child health could also consider these associated factors.
Data availability statement
Data are available in a public, open access repository. Data for this study were sourced from Demographic and Health surveys (DHS) and available here: http://dhsprogram.com/data/available-datasets.cfm.
Ethics statements
Ethics approval
We used datasets provided by the Demographic Health Surveys programme and have not had any form of contact with the study participants. The programme obtains approval from the Ethics Boards of the various partner organisations and countries such as the Ministries of Health. The DHS programme recognises and adheres to established international and local ethical standards and protocols in its surveys. The ICF International’s Institutional Review Board (IRB) through The DHS programme’s reviewed and approved all survey procedures and instruments used before implementation. The board aside from providing technical assistance to the programme ensures that the survey complies with the US Department of Health and Human Services regulations for the protection of human subjects CFR 46 as well as the laws of the individual countries. Further information regarding the DHS data usage and ethical standards can be accessed online (https://dhsprogramcom/data/Access-Instructionscfm).
Acknowledgments
We acknowledge the Demographic Health Surveys for providing us with the data upon which the findings of this study were based. Special thanks to Mr Eric Duku for his support in the spatial representation of child anaemia.
References
Footnotes
Contributors IA conceptualised and designed the study. IA and A-RA performed the analysis. IA, A-AS, A-RA, BOA and SY drafted the initial draft. AS, AA, BOA and SY provided technical support and critically reviewed the manuscript for its intellectual content. SY had the final responsibility to submit for publication. All authors read and amended drafts of the paper and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer Ethics approval was not required for this study since the data are secondary and are available in the public domain. More details regarding DHS data and ethical standards are available at: http://goo.gl/ny8T6X.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.