Article Text

Abstract
Objective To evaluate the pattern of frailty across several of social stratifiers associated with health inequalities.
Design, setting and participants Cross-sectional baseline data on 51 338 community-living women and men aged 45–85 years from the population-based Canadian Longitudinal Study on Aging (collected from September 2011 to May 2015) were used in this study.
Primary outcomes and measures A Frailty Index (FI) was constructed using self-reported chronic conditions, psychological function and cognitive status and physical functioning variables. Social stratifiers were chosen based on the Pan-Canadian Health Inequalities Reporting Initiative, reflecting key health inequalities in Canada. Unadjusted and adjusted FIs and domain-specific FIs (based on chronic conditions, physical function, psychological/cognitive deficits) were examined across population strata.
Results The overall mean FI was 0.13±0.08. It increased with age and was higher in women than men. Higher mean FIs were found among study participants with low income (0.20±0.10), who did not complete secondary education (0.17±0.09) or had low perceived social standing (0.18±0.10). Values did not differ by Canadian province of residence or urban/rural status. After simultaneously adjusting for population characteristics and other covariates, income explained the most heterogeneity in frailty, especially in younger age groups; similar patterns were found for men and women. The average frailty for people aged 45–54 in the lowest income group was greater than that for those aged 75–85 years. The heterogeneity in the FI among income groups was greatest for the psychological/cognitive domain.
Conclusions Our results suggest that especially in the younger age groups, psychological/cognitive deficits are most highly associated with both overall frailty levels and the gradient in frailty associated with income. If this is predictive of later increases in the other two domains (and overall frailty), it raises the question whether targeting mental health factors earlier in life might be an effective approach to mitigating frailty.
- epidemiology
- geriatric medicine
- public health
Data availability statement
Data are available upon reasonable request. Data are available from the Canadian Longitudinal Study on Aging (www.clsa-elcv.ca) for researchers who meet the criteria for access to de-identified CLSA data.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The large population-based sample with sampling weights making the results generalisable to middle-aged and older community-living adults in Canada.
The use of multiple population stratifiers associated with social inequalities.
The use of the LMG statistic to assess the relative amount of heterogeneity in the Frailty Index explained by different social stratifiers adjusted for each other and relevant covariates.
The cross-sectional nature of the data does not allow for causal inferences.
Sampling bias may be present, as participants were generally healthy volunteers residing in the community.
Background
Frailty is recognised as a multidimensional concept with dynamic inter-related physical, psychological, social and environmental deficits associated with increasing levels of vulnerability and declining reserve.1 Frailty levels generally increase with age, are higher in women and are associated with an increased risk for both current and future disability, falls and fractures, mortality and other adverse health outcomes.2–4 Frailty level is also a strong predictor of health and social care utilisation such as emergency department visits and hospitalisations and hospital readmissions5 as well as receiving informal care.6 By 2050, the world’s population aged 60 years and older is expected to total 2 billion, up from 900 million in 2015, and 125 million people aged 80 years or older. With this demographic transition, frailty is an emerging public health priority7 8 and there has been an increasing interest to consider the importance of upstream social, in particular, socioeconomic status (SES) factors to help understand the heterogeneity in frailty across the population spectrum.9
Researchers have found a relationship between SES and health indicators with generally worse health associated with lower SES measured by different social determinants, such as income, wealth and education.10 11 Link and Phelan proposed that social factors such as SES are a ‘fundamental cause’ of disease.12 The magnitude of the gap between lower and higher SES groups, however, has been found to differ by sex and vary with age.13–15 There are two main theories regarding this changing relationship between SES and health indicators with ageing. The first is that the impact of SES is cumulative with increasing divergence between SES groups with ageing (cumulative disadvantage) while the second holds that early divergence is followed by convergence later in life (age-as-a-leveller).16
There is conflicting evidence on whether differences in frailty status across SES groups decrease, stay the same or increase with age.17–19 The conflicting evidence may be due in part to differences in the social stratifiers used to explain heterogeneity across studies. For example, Stolz et al18 found that health inequalities due to education, occupation and wealth (ie, the household net worth including real estate and financial assets) tended to persist throughout old age whereas the effect of income (ie, wages, pensions and social transfers) declined. In addition, the magnitude of the gap between physical health and psychological health indicators has been shown to differ with age.10 14 20 This is relevant as frailty is multidimensional and is often measured by the Frailty Index (FI) which incorporates deficits from a range of body systems, including chronic conditions, physical, psychological and cognitive factors, but the specific deficits included and the number of deficits per body system generally differ by study.21 To help understand what factors may be associated with the conflicting evidence, a comprehensive assessment of multiple social stratifiers and decomposition of frailty into subdomains including chronic conditions, physical, psychological and cognitive factors is needed.
Understanding why some people are frail while others are not, or the heterogeneity in frailty, has significant public health importance.22 Our recent context of the disproportional impact of COVID-19 on older adults and increasing evidence that social inequalities are profoundly impacting COVID-19 morbidity and mortality has heightened this importance.23 To understand this, however, requires a very large data set to disentangle which factors best explain the heterogeneity in frailty and whether the patterns across social stratifiers differ by sex and age group. In this study we examined the heterogeneity of a FI across several of social stratifiers associated with health inequalities in a population of over 50 000 middle-aged and older using the Canadian Longitudinal Study on Aging (CLSA). The items making up our FI could be categorised into three domains (physical function, chronic conditions and psychological/cognitive deficits). We further examined if the patterns differed by frailty domain.
Methods
Study design/setting
The CLSA is one of the largest and most comprehensive research platforms examining health and ageing.24 All study participants provided a core set of information on demographics and measures of lifestyle/behaviour, social, physical, psychological and health status. Of the 51 338 participants, 21 241 were randomly selected from the 10 Canadian provinces and provided questionnaire information through telephone interviews (referred to as CLSA tracking), The other 30 097 (CLSA comprehensive) had in-home interviews to collect information similar to that provided by the CLSA tracking participants and then visited one of 11 Data Collection Sites (DCSs) where they also underwent detailed physical assessments and provided blood and urine samples. Comprehensive participants were randomly selected from areas extending 25–50 km from each of the DCSs. The present analysis uses cross-sectional baseline data from all 51 338 CLSA participants. These data were collected between September 2011 and May 2014 for tracking and between May 2012 and May 2015 for comprehensive participants.
Participants
CLSA participants are community-living women and men aged 45–85 years at the time of recruitment. People who were living on federal First Nations reserves, full-time members of the Canadian Armed Forces, resided in institutions (eg, long-term care institutions), unable to respond in English or French or with cognitive impairment were excluded.
Variables
Frailty Index
The FI used in this study was constructed using the methodology described by Searle et al.21 Details on its construction have been provided elsewhere.25 In brief, each health deficit was recoded as ‘0’ if absent and ‘1’ if present. For non-binary variables, a gradient from 0 to 1 was created using equal steps (eg, if a deficit had three levels, it would be coded ‘0’, ‘0.5’ and ‘1’). The FI value for a participant was the sum of deficits present divided by the total number of deficits measured. Candidate deficits for the FI were selected based on the literature and expert input.25 Deficits were operationalised where possible using the same variables in both the tracking and comprehensive cohorts. An exception was physical functioning measures that were self-reported in the tracking cohort and performance-based in the comprehensive cohort. In previous research we have found that the magnitude of association with disability was similar across self-reported and performance-based measures.26 As well, the relationship between FIs and adverse health outcomes have been shown to be consistent regardless of the actual variables included if at least 30–40 health deficits are selected using Searle’s criteria.21 In total, 85 deficits comprised the FI for tracking and 76 for comprehensive participants (71 in common). The items making up the CLSA FI were grouped into three domains: chronic conditions (n=32), psychological function and cognition (n=20) and physical functioning (n=33 for the tracking and n=24 for the comprehensive participants). The creation of the three domains was informed by factor analysis and expert input.25 A summary of the operationalisation and descriptive statistics for each deficit overall and by cohort is in online supplemental eTable 1.
Supplemental material
Social stratifiers
The United Nations 2030 Agenda for Sustainable Development describes the importance of addressing social determinants of health.27 In this study we used social stratifiers identified by the Pan-Canadian Health Inequalities Reporting Initiative, reflecting key health inequalities in Canada.28 These included age, sex, income, education, retirement status, rural/urban status and material and social deprivation. Evidence suggests that health deficit accumulation is associated with higher mortality and health service even in middle age.29 In our study age was categorised as 45–54, 55–64, 65–74 and 75–85 years. Household income per annum was based on Canadian dollars and categorised as <$C20 000, $C20 000–$C50 000, $C50 000–$C100 000, $C100 000–$C150 000 and ≥$C150 000. Education was categorised into not graduating from a secondary school, secondary school graduation with no post-secondary education, some post-secondary education and post-secondary degree or diploma. Retirement was categorised as completely retired, partly retired and not retired. Rurality was classified by population density into census metropolitan areas (CMA) with a population of 2 million or more (large CMA), CMAs with population <2 million (other CMA) other smaller towns with population typically 10 000–120 000 (agglomeration) and areas with a population <10 000 (rural).30 Material and social deprivation quintiles31 were based on Canadian Census enumeration area data linked to CLSA by the Canadian Urban Environmental Health Research Consortium.32 Both are small-area based composite indices which reflect the deprivation of relationships among individuals in the family, the workplace and the community (social deprivation) and the deprivation of wealth, goods and conveniences (material deprivation). We did not include the following social stratifiers due to small cell sizes (cultural/racial background, immigration, visible minority and indigenous identity) and occupation type was not yet available.
Covariates
Covariates considered for adjustment were chosen based on the frailty literature.33 34 The following covariates were used for adjustment: marital status (married/common-law or other); smoking status (current/former daily smoker or other); nutritional risk (score <38 on AB SCREEN II Nutritional Risk35; low self-perceived social participation (yes or no); living alone (yes or no); and low physical activity (<75 min per week of vigorous-intensity or 150 min per week of combined moderate-intensity and vigorous-intensity physical activity.36
Statistical methods
Descriptive statistics were calculated as means and SD for continuous measures and percentages for categorical variables. In our analyses ‘heterogeneities’ refers to differences in aggregate measures of FI among population groups.22 The average frailty level and 95% CI were estimated for population subgroups based on social stratifiers using least squares means from linear regression. Frailty estimates were also adjusted for potential confounders and all other social stratifiers. The relative amount of heterogeneity in the FI explained by different social stratifiers was assessed using the LMG statistic.37 This statistic represents the relative contribution of each variable to the model R2. Analyses were further stratified by sex and age to examine if associations with social stratifiers were consistent or differed by these factors. While we found frailty was higher among women, the patterns across age-groups were similar for women and men and thus they were combined.
Inter-correlations were explored among domain-specific FIs (chronic conditions, physical function, psychological/cognitive). Because income was found to explain the most heterogeneity in the FI among the social stratifiers, the domain-specific regression analyses were restricted to income only. Regression analyses were adjusted for all potential confounders included in the overall frailty model and a final ‘fully adjusted’ model also included the other frailty domains. The CLSA has a complex sampling design, thus weights were calculated to create prevalence estimates that can be generalised to the Canadian population (inflation weights) and for estimating associations (analytical weights).38 Although the amount of missing data was relatively low, <6.5% for all variables, we anticipated that participants who were frailer might have more missing data. Multiple imputation was conducted using predictive mean matching to provide estimates little prone to bias.39 The results reflect the average frailty values calculated in 10 imputed data sets and combined. Residual analyses were conducted to assess model fit and appropriateness of underlying assumptions.
Sensitivity analyses included a complete case analysis and separate analyses for tracking and comprehensive cohorts. Because the FI tends to be right-skewed we conducted sensitivity analyses using the natural log of FI (In(FI)). Finally, more psychological/cognitive and physical functioning deficits had multiple categories (ie, were not binary) and used gradient coding. We conducted sensitivity analyses in which we forced a binary coding for all deficits to assess if higher FI values for these domains could be due to end-aversion bias.40 All analyses were conducted using SAS V.9.4.41 We used the Strengthening the Reporting of Observational Studies in Epidemiology cross-sectional checklist when writing our report.42
Patient and public involvement
There were no participants involved in the development of this study. The results of the CLSA are disseminated to the public through websites and webinars.
Results
Participants
Table 1 displays the characteristics of the CLSA population by age group. The mean FI was 0.131 for all participants and increased with age, from 0.114 for those 45–54 to 0.157 in those 75–85. The psychological/cognition domain had the highest mean values for all subgroups and showed less of an age gradient. Approximately 51% of CLSA participants were women, about 31% had an income less than $C50 000 and most had a post-secondary degree or diploma. About 56% of participants were either completely or partially retired and relatively few lived in a rural area.
Frailty level and demographic, socioeconomic and lifestyle characteristics for all participants of the Canadian Longitudinal Study on Aging (n=51 338) and by 10-year age groups
Frailty levels across subgroups
Figure 1a displays the average unadjusted FI across population characteristics. For each social stratifier except for rural/urban status there was a gradient of higher frailty associated with lower SES. The most heterogeneity in FI was explained by income (R2=13.3%) where the average FI for people making $C150 000 or more was less than half (0.088) of those making less than $C20 000 (0.201). Figure 1b shows the average FI across population characteristics adjusting for potential confounders and all other social stratifiers described above. In the fully adjusted model 24.3% of the variance in FI was explained by all social stratifiers and potential confounders. While SES gradients were attenuated by this adjustment across all subgroups, the heterogeneity across income groups was still apparent after adjusting for all potential confounders explaining 25.6% of the total model R2 (24.3%); the other social stratifiers explained between 8.2% (retirement status) to 0.5% (rurality) of the total model R2. In total after adjusting for marital status, social participation, living alone, smoking, physical activity and nutritional risk, the social stratifiers still explained 43.3% of the R2. Similar results were found when using In(FI) (data not shown). Because fit statistics were similar across models, we chose to present only FI results as they are more easily interpreted than In(FI).

(A) shows the unadjusted weighted least squares mean Frailty Index (FI), 95% CI and the associated model R2 for each social stratifier assessed. (B) shows the fully adjusted weighted least squares mean frailty and 95% CI by social stratifier. The variance in FI explained by all variables was R2=24.3%; the LMG represents the per cent of the model R2 explained by each social stratifiers assessed. The fully adjusted model included all social stratifiers shown in the Figure, as well as potential confounding variables: marital status (married/common-law or other); smoking status (current/former daily smoker or other); nutritional risk (score <38 on AB SCREEN II Nutritional Risk)34; low self-perceived social participation (yes or no); living alone (yes or no); and low physical activity (<75 min per week of vigorous-intensity or 150 min per week of combined moderate-intensity and vigorous-intensity physical activity. Points show the least-squared mean FI. CMA, census metropolitan area; LS, least square.
Frailty levels by income level stratified by age and sex
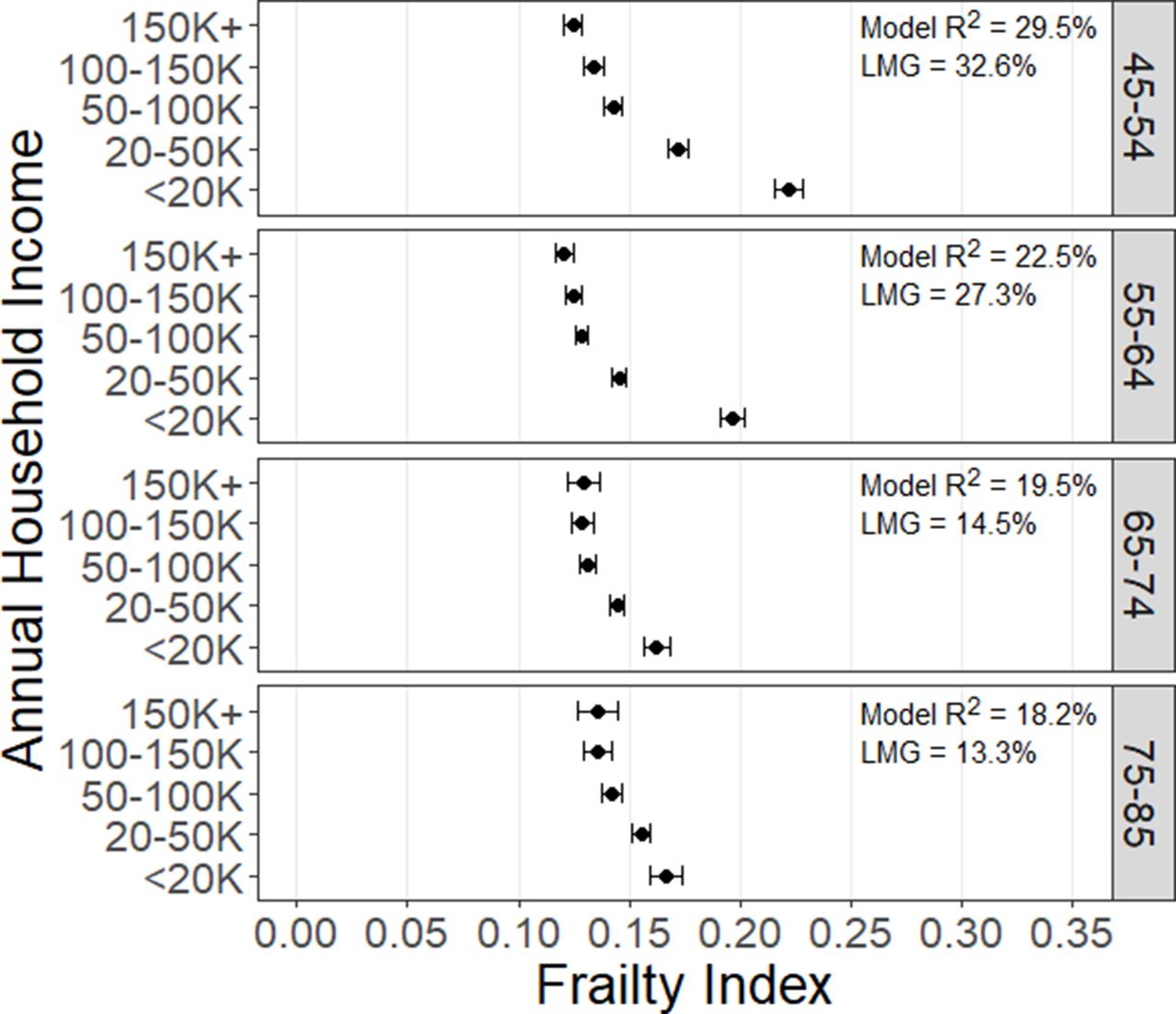
Figure 2 displays the income gradient from the fully adjusted model stratified by age group. While the income gradient was evident for all age groups, the amount of variability in FI explained by all variables in the model (R2) and the relative importance of income (LMG) decreased with age. The model R2 ranged from 29.5% (LMG 32.6%) for 45–54 years to 18.2% (LMG 13.3%) for 75–85 years. Women tended to have higher FIs than men overall, but a similar pattern between frailty level, age and income was found across sexes (online supplemental eFigures 1-2).

shows the adjusted weighted least squares mean Frailty Index and 95% CI for each level of income, by 10-year age categories and adjusted for all other social stratifiers (education, geography, retirement status, material and social deprivation indices), as well as potential confounding variables: marital status (married/common-law or other); smoking status (current/former daily smoker or other); nutritional risk (score <38 on AB SCREEN II Nutritional Risk); low self-perceived social participation (yes or no); living alone (yes or no); and low physical activity (<75 min per week of vigorous-intensity or 150 min per week of combined moderate-intensity and vigorous-intensity physical activity. R2 represents the proportion of variance in Frailty Index explained by all variables each model (one for each age group); LMG represents the proportion of the model variance explained (R2) that can be attributed to household income.
Domains of frailty
All domains of frailty were weakly to moderately correlated (psychological/cognition and chronic conditions (r=0.29), psychological/cognition and chronic conditions (r=0.39) and physical function and chronic conditions (r=0.46). Figures 3a-c display the income gradient for each domain of frailty–chronic conditions (3a); physical functioning (3b); and, psychological/cognition (3c) by age group. After adjustment for all other factors, including the other frailty domains, there was little income gradient for the chronic conditions domain, but there was a clear gradient of increasing deficits with age. The physical functioning domain had a similar pattern as the overall FI, with a consistent income gradient and the heterogeneity across income groups decreasing with age. The psychological/cognition domain had the strongest income gradient for all age groups, with less heterogeneity with increasing age. The average adjusted psychological/cognition domain score for 45–54 year olds with a household income <$C20 000 was about 0.3. In sensitivity analyses where all deficits were coded as binary similar patterns were seen, but the absolute values of frailty were lower for the physical functioning and psychological/cognition domain. The average psychological/cognition domain score for 45–54 year olds with a household income <$C20 000 was approximately 0.2, representing an endorsement of 20% of the deficits on average. Similar results were found in the complete case analyses and cohort-specific analyses (data not shown).

{kind=link}
{kind=link}
{kind=link}
(A-C) shows the adjusted weighted least squares mean domain-specific Frailty Index and 95% CI by level of household income and stratified by age group. (A) represents the chronic conditions domain, (B) physical domain and (C) psychological/cognitive domain. Each model is adjusted for the other domains of frailty, all other social determinants (education, geography, retirement, material and social deprivation indices), as well as potential confounding variables: marital status (married/common-law or other); smoking status (current/former daily smoker or other); nutritional risk (score <38 on AB SCREEN II Nutritional Risk); low self-perceived social participation (yes or no); living alone (yes or no); and low physical activity (<75 min per week of vigorous-intensity or 150 min per week of combined moderate-intensity and vigorous-intensity physical activity. R2 represents the proportion of variance in the domain-specific Frailty Index explained by all variables each model (one for each age group); LMG represents the proportion of the model variance explained (R2) that can be attributed to household income.
Discussion
Identifying how frailty levels vary across social stratifiers associated with health inequalities, and examining whether the associations found, differ across age groups can help guide public health interventions as there has been much focus on proximal causes and less of ‘fundamental causes’ associated with socioeconomic inequalities.12 Other than urban/rural status we found that mean FI values were associated with all the social stratifiers suggested by the Pan-Canadian Health Inequities Reporting Initiative28 that we could assess. This persisted after adjustment for potential confounders and other social stratifiers. The frailty gap across income groups was greatest in the younger age groups compared with those 65 years and older. In fact, we found the average frailty level for 45–54 year olds in the lowest income group is greater than that for 75–85 year olds in our study population. Furthermore, especially in the younger age groups, the heterogeneity among income groups was associated primarily with the psychological/cognitive deficits used to calculate the FI. While frailty levels were higher among women compared with men, the patterns across age groups and income were similar.
Our results agree with many studies examining the association between social determinants of health and frailty,43–46 frailty trajectories17 18 and the rate of deficit accumulation.19 47 48 Hajizadeh et al49 found persistent education-related and income-related inequalities in frailty were present in all regions of Canada. St John et al46 reported there was a gradient in frailty across several measures of social position (education, income security, home ownership and satisfaction with income). We found that household income had the strongest relationship with frailty heterogeneity both in an unadjusted analysis and in an analysis adjusted for all other social stratifiers and the patterns were consistent across sex. Using US data Yang and Lee48 found that men and women accumulated deficits at the same rate. Frailty levels for women were consistently higher than men and also paralleled sex-specific trajectories of frailty levels with ageing.48
While most studies did not examine the independent effect of each social stratifier after adjusting for others, Stolz et al18 using European data found that differences in frailty status associated with education, occupational class and wealth continued throughout old age, while differences related to income became smaller in comparison and converged over time. The age-as-leveller hypothesis predicts such a convergence because of universal biological decrements at older ages, retirement ending inequalities in the work context and possibly the impact of social policies.50 In our study we found the differences in FI among the income groups reduced at age 65, which coincides with the age at which Canada’s public retirement income system becomes available for most Canadians.51 While we also found less heterogeneity with respect to income in the older age groups, as noted, we did not examine heterogeneity with respect to wealth or occupational class. As well, this could reflect the increasing variability with ageing found among many health characteristics. Nguyen et al52 found both the mean and variance of frailty increased with age. It is also possible that proportion of variance explained by any individual factor, such as income, may decrease with age.
When we further divided frailty deficits into the domains of chronic condition, physical frailty and psychological/cognitive we found that after adjustment for the other domains, the heterogeneity among income categories was most evident in the psychological/cognitive and physical frailty deficits. Other studies have found different relationships between SES indicators and physical and psychological outcomes. Schöllgen et al11 examined the relationship between SES indicators and physical (number of chronic conditions), functional (SF-36) (physical functioning subscale) and subjective health (self-perceived health). They found that after controlling for confounders, income was significantly related to functional and subjective health but not to physical health based on the number of chronic conditions. They further found that the interaction between income and age was not significant for physical and functional health, but was significant for subjective health, due to the decreased influence of low income on subjective health at older ages. Kim and Durden20 examined SES indicators and physical impairment and depression and found that income-based gradients in physical impairment grew over time for all adult age groups while the one with depression converged at older ages. Franse et al45 examined the association between frailty domains and SES (education) and found that among all frailty components other than instrumental activities of daily living stronger associations were observed in persons 55–69 years (their youngest age group) compared with older age groups. The strongest association was found with psychosocial health. Interestingly, of the literature we reviewed examining health inequalities and frailty level, the per cent of psychological health/cognitive deficits was less than 10% in five studies,18 43 44 47 53 between 10%–25% in one study53 and >25% in three.17 19 48 Particularly when studies include younger participants it may be important to include more psychological items in the assessment of frailty.
This study used data from a large population-based study including middle-aged and older adults. The richness of the data and the magnitude of the sample size allowed us to examine many social stratifiers and adjust for numerous potential confounders. The sample size also allowed us to conduct stratified analyses to examine these relationships by policy-relevant subgroups (age and sex) that can be used to inform further research, policy and the development of potential interventions. We also conducted numerous sensitivity analyses to assess the robustness of our results to methodological decisions made throughout our study. Compared with other FIs creating from CLSA,52 54 our mean FI values tended to be slightly higher. This is most likely due to our inclusion of relatively more psychological/cognition deficits which were of a priori interest. This study, however, as with others also has limitations. Sampling bias may be present, as participants were generally healthy volunteers residing in the community. For many variables CLSA results have been shown to be similar to other population-based Canadian data sources, but CLSA participants tended to be more highly educated, have higher household income, have higher percentages of participants who are Canadian born.24 It should be noted that were not able to examine cultural/racial background, immigration, visible minority and indigenous identity in this study. We know that frailty prevalence and trajectories vary between ethnic groups, migrants and minority native groups.55 While our results may not be completely representative, the level of heterogeneity in frailty level among income groups that we found would likely be an underestimate. The data presented are also cross-sectional. We are not able to rule out reverse causation or disentangle potential cohort effects. It is possible that an increase in one’s level of frailty could affect their ability to work and thus lead to reduced income. Other longitudinal studies have also found income gradients with respect to frailty,18 19 49 though not all.47 Previous studies have also shown that there are cohort differences in frailty levels possibly attributable to differential survival of frail individuals.19
Clinical and public health importance
Reducing frailty and its negative health consequences is a priority for public health.7 Our results suggest that especially in the younger age groups, psychological/cognitive deficits are most highly associated with both overall frailty levels and the gradient in frailty associated with income. If this is predictive of later increases in the other two domains (and overall frailty), it raises the question whether targeting mental health factors earlier in life might be an effective approach to mitigating frailty. Longitudinal data are needed to explore both the time course and inter-relationships across the three domains. In particular, research is needed to examine how the FI domains evolve over time and how well this evolution predicts adverse outcomes.
Data availability statement
Data are available upon reasonable request. Data are available from the Canadian Longitudinal Study on Aging (www.clsa-elcv.ca) for researchers who meet the criteria for access to de-identified CLSA data.
Ethics statements
Ethics approval
This study was approved by the Hamilton Integrated Research Ethics Board (Ethics certificate #: 3152). Participants of the Canadian Longitudinal Study on Aging provided written informed consent to participate.
Acknowledgments
The Material and Social Deprivation Indices (MSDI), indexed to DMTI Spatial postal codes, were provided by CANUE (Canadian Urban Environmental Health Research Consortium) and provided by: Institut National de Santé Publique du Québec (INSPQ). Indiceses were compiled for 1991, 1996, 2001 and 2011 Census data by the Bureau d'information et d'études en santé des populations (BIESP) (https://www.inspq.qc.ca/en/expertise/information-management-andanalysis/deprivation-index). The AB SCREEN II assessment tool is owned by Dr Heather Keller. Use of the AB SCREEN II assessment tool was made under license from the University of Guelph.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @LaurenGriff1
Contributors LEG and PR designed the project with the input from all authors. All authors (LEG, PR, DK, DH, CP, AP, JR, AG, MT and EvdH) worked together to obtain funding for and deciding the scope and structure of the study. DK conducted all analyses with statistical input from MT and EvdH. LEG wrote the first draft of the manuscript. All authors (LEG, PR, DK, DH, CP, AP, JR, AG, MT and EvdH) contributed to the interpretation, writing and critical revision of the manuscript and approved the final manuscript.
Funding This research was made possible using the data/biospecimens collected by the Canadian Longitudinal Study on Aging (CLSA). Funding for the CLSA is provided by the Government of Canada through the Canadian Institutes of Health Research under grant reference: LSA 94473 and the Canada Foundation for Innovation. This research has been conducted using the CLSA dataset Baseline Tracking V.3.1 and Baseline Comprehensive V.2.0, under application number 150306. The CLSA is led by Drs. Parminder Raina, Christina Wolfson and Susan Kirkland. This study was supported by a Canadian Institutes of Health Research Catalyst Grant (FRN 151287). Lauren Griffith is supported by the McLaughlin Foundation Professorship in Population and Public Health. Parminder Raina holds a Tier 1 Canada Research Chair in Geroscience and the Raymond and Margaret Labarge Chair in Research and Knowledge Application for Optimal Aging.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.