Article Text

Abstract
Objective To identify, summarise and evaluate evidence on the correlation between perceived and actual neighbourhood safety (personal and road danger) and diverse forms of outdoor active mobility behaviour (ie, active play, exercise, and travel) among primary-school-aged children.
Design A systematic review of evidence from observational studies exploring children’s active mobility behaviour and safety.
Data sources Six electronic databases were searched: Google Scholar, PubMed, Scopus, Science Direct, ProQuest and Web of Science from study inception until July 2020.
Data extraction and synthesis Study selection and quality assessment were conducted independently by two reviewers. We expanded on a quality assessment tool and adopted a vote-counting technique to determine strength of evidence. The outcomes were categorised by individual, family and neighbourhood levels.
Results A total of 29 studies were included, with a majority of cross-sectional design. Higher parental perceived personal safety correlated with increased children’s active mobility behaviour, but most commonly in active travel (eg, independent walking or cycling to a local destination). Increased concerns regarding road danger correlated with a decrease in each type of children’s active behaviour; active travel, play and exercise. However, these correlations were influenced by child’s sex/gender, age, car ownership, neighbourhood types, across time, and proximity to destination. Limited or inconclusive evidence was found on correlate of children’s outdoor active mobility behaviour to ‘stranger danger’, children’s perceived personal safety, race/ethnicity, socioeconomic status or measured safety.
Conclusion Children are restricted by perception of safety. Encouraging children’s active travel may require future strategies to address characteristics relevant to types of the neighbourhood that promote a high sense of personal safety. Children and parents may embrace other types of active mobility behaviour if road danger is mitigated. Sex/gender and age-specific interventions and redesign of public places could lead to child-friendly cities. Future studies may benefit from adopting validated measurement methods and fill existing research gaps.
- public health
- epidemiology
- sports medicine
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This systematic review adapted a methodological quality appraisal that integrated studies’ reporting and measurement methods along with a vote-counting technique to understand the strength of the evidence.
To our knowledge, this is the first systematic review that comprehensively synthesises evidence on neighbourhood safety correlates to forms of primary school-aged children’s outdoor active mobility behaviours.
Peer-reviewed studies published in languages other than English were excluded, and meta-analysis review was not possible due to the heterogeneity in studies measurement methods and outputs.
Introduction
Children’s daily active mobility behaviour is linked with profound long-term positive outcomes.1 Recommended daily level of children’s physical activity is primarily achieved through various forms of structured (ie, organised sport) or unstructured active behaviour (ie, active play in open spaces, walking, cycling or scootering to school and other local destinations).2 3 Neighbourhood, the place where a child’s majority of daily routines occur, has been identified as a primary venue for children to meet the daily physical activity recommendations.2 However, variability in the neighbourhood (ie, residential, commercial, industrial and agricultural) have been found to affect types and extent of children’s various shapes of active behaviour.4 5 For example, different types of neighbourhood were linked to changed levels of active transportation in children aged 10–11 years living in Finnish urban areas.6 Canadian children travel longer distance actively in residential or commercial areas than other types of neighbourhood.5 Urban and road structures in The Netherlands reversed the negative effect of reduced active travel with longer distances.7 Nevertheless, neighbourhood impact on other aspects of children’s behaviour such as play and peer interaction is mixed.8
Safety, including personal and road danger,9 10 is a complex concept.3 Perceived (by parents or children) or measured safety (actual crime and traffic danger) may create obstacles resulting in children’s lower confidence in exploring their surroundings,2 or contributing to their community.11 Lack of safety may have contributed to urban streets and public spaces becoming increasingly inhospitable environments. With more people living in urban settings than ever before,12 and increasing safety concerns, children’s territory for active outdoor mobility behaviour, such as walking, playing, cycling and scootering, has shrunk.13–16 The damage caused by restricting children’s active mobility behaviour may extend beyond their immediate physical health,17 to overall social skills18 and healthy brain development.19
Nevertheless, reviews that addressed neighbourhood safety and children’s active behaviour have reported conflicting results. The disagreements could be due to: narratively investigating safety,3 examining one shape of active behaviour such as active school travel9 20–23 or independent mobility24 or combinedly addresses safety with other environmental correlates and from a wide age range of children age (three or five to 18 years).16 25 26 Over and above that, variability in measurement methods and output adds complexity in evaluating available evidence.20 22 The absence of suitable checklists that account for measurement methods when assessing the quality of observational studies,24 called research for alternatives approach to increase confidence in the synthesis of studies outcome20 22 and inform evidence-based policy decisions. On the other hand, active school travel is a significant contributor to overall child active behaviour,27 but other forms of activity incorporated into children’s daily routines24 are vital contributors to children’s daily movement targets.28 No review up to now has exclusively focused on the varying impact of measured and perceived safety in urban settings across primary-school-aged children’s various forms of daily active mobility behaviours. Thus, this review aims to (1) systematically synthesise evidence of correlations between primary-school-aged children’s outdoor active mobility behaviour (COAMB) and neighbourhood measured and perceived safety, and (2) derive the strength of the evidence by evaluating quality and methodological measurement method for each study and vote counting technique as justified from previous reviews.
Method
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). The corresponding PRISMA checklist was completed during the review, as illustrated in online supplemental file 1. Though the search was planned, no protocol was registered.
Supplemental material
Search strategy
A keyword search was designed and conducted to identify all relevant studies in six electronic databases: Google Scholar, PubMed, Scopus, Science Direct, ProQuest and Web of Science. All databases were searched between March 2019 and July 2020. The search algorithm included all possible combinations of keywords. Terms pertaining to this review were grouped by (1) target population, (2) AND active behaviour, AND (3) neighbourhood safety, OR (4) moderators and mediators, OR (5) spatiotemporal aspects (Global positioning system, GPS, geographic information system, GIS, out of school hours). The entire search thesauruses and strings are available in online supplemental file 2. Additional papers were identified from the citation lists of individual and review papers.
Supplemental material
Eligibility criteria
Studies were included for review if they were: published in peer-reviewed journals, in English, were observational studies that collected data directly on participants aged between five and 12 years (primary-school-aged children), assessed neighbourhood safety (personal and road safety) either as perceived by parents and/or children or measured (crime or road conditions), and reported or measured children’s active mobility outside school hours. Included publications were not restricted to a single geographic location or a specific time. Studies were excluded for failing to meet the inclusion criteria. Systematic, scoping, or narrative reviews, opinion and editorial pieces, and other non-original research publications were also excluded.
Study selection process
Using search terms developed for this review, one reviewer (RZ) screened titles and abstracts to identify those works that met the inclusion criteria. Abstracts of the downloaded papers were then reviewed by two independent reviewers (RZ, CX) against the selection criteria. The final list of included studies was agreed by consensus involving a third reviewer (RN). Studies that met inclusion criteria were reviewed in full by RZ.
Data extraction process
The first author (RZ) extracted, into an excel datasheet relevant information on: author(s) year of publication, year of data collection, location of study, sample size (separated by gender), age/school grade, characteristics regarding methods of measuring or assessing neighbourhood safety (perceived or measured), children’s active behaviour and outcome measures (eg, body mass index (BMI) or medium-to-vigorous physical activity (MVPA)), child’s neighbourhood, other variables accounted in studies analysis including cofounders (eg, sex/gender/family characteristics) and summary of findings. The data were collated into a systematic narrative summary table of the relevant papers.
Patient and public involvement
No patients involved.
Data synthesis
Correlates between COAMB and safety were organised according to aspects of the socioecological framework (ie, individual, family, and neighbourhood). This framework is frequently used in active health behaviour research29 as a conceptualisation tool. This tool provides a structure for organising and understanding multiple factors that cause changes in health behaviour. Additionally, to enable the review investigating influences specific to forms for active behaviour, the outcome of correlates were compared by grouping findings into one of four categories: active travel; school travel; active play; active play, travel and exercise. The subgrouping corresponds to children’s main types of structured and unstructured active behaviour outside of school hours.30
Quality assessment
Two independent reviewers (RZ, BJ) appraised the selected studies using priori defined quality criteria. Previously practised quality assessment by Schoeppe et al24 for active travel, Marzi and Reimers31 on independent mobility, and by Lubans et al27 on active school travel, were reviewed. We adopted 13 existing criteria used earlier that covers all pertinent studies quality reporting characteristics. We expanded on six items to the checklist based on findings from a recent systematic review of which methodological measures in observational studies were assessed and found to be fundamental to increase reliability in children’s active behaviour research.32 Those measures were covering: COAMB (objective or subjective), temporality elements such as change in time of day, weekdays or weekends (addressed in both perceptions of safety as well as COAMB), the delineation of the neighbourhood area (arbitrary or measured) and accounting for cofounders. We adopted the scoring system applied by Marzi and Reimers31 and Schoeppe et al24 to quantify study robustness. Each criterion in the quality assessment checklist was given the assigned score if coded ‘yes’, 0 if coded ‘no’ or unclear, and half the score if coded ‘partial’. A total overall score out of eight points was assigned, showing in table 1. As included studies have employed a variety of tools and sometimes composite techniques to measure active behaviour, we adopted Marzi et al method for criterion number fourteen that was scored on a scale ranging from 0 to 1. For example, if a study employed an accelerometer and GPS, the study accumulates 0.5 points. However, when the study only used one measurement tool, it was assigned 0.25 points. A study variable that was measured appropriately but was not applicable to a specific criterion used for the quality assessment was discounted in the sum of total points used to derive quality score.24 For example, the quality assessment criterion related to temporal and spatial measurement was not applicable for a paper where the primary outcome measure was BMI. In that instance, the criterion was removed from the total quality score of that paper.24 The quality score for each study was calculated by converting the total accumulated score into a percentage (total accumulated score/8 (maximum possible score) × 100).24 Adopting Schoeppe et al cut-off for levels of studies’ quality, a percentage score of ≥66.7% was deemed robust, a score between ≥50 and<66.6% was considered moderate, and <50% was rated poor.
Criteria for quality assessment and scoring for each criterion adapted from previous published systematic reviews
Evidence synthesis and strength
Evidence synthesis described by Rothman et al22 and Ikeda et al20 was used in this review. Each correlation and its direction (positive (+), negative (−), or inconclusive/no correlation(0)) was identified and coded in terms of statistically significant or non-significant findings organised by the socioecological levels. To facilitate synthesis of evidence, we performed a reverse coding of the original direction of associations (ie, positive to negative or vice versa) as necessary, depending on the wording used in each work.20 A minimum of five studies with significant or non-significant findings was adopted to generate a consensus.20 22 Evidence with less than five studies available for synthesis was rated as limited,24 and with three studies was rated insufficient. Deriving strength of evidence was also adapted from previous reviews24 27 using the proportion and quality of studies reporting a significant association. The ratio of studies found with robust quality in this review to those found in an earlier review24 was used to rescale the quality thresholds. In a minimum of five studies, if ≥27% of the total synthesised significant evidence that agrees in a direction (ie, +, − or 0) was of robust studies, the evidence was rated strong, from ≥20%–<27% was moderate strength, and at <20% was rated weak.
Results
Study selection
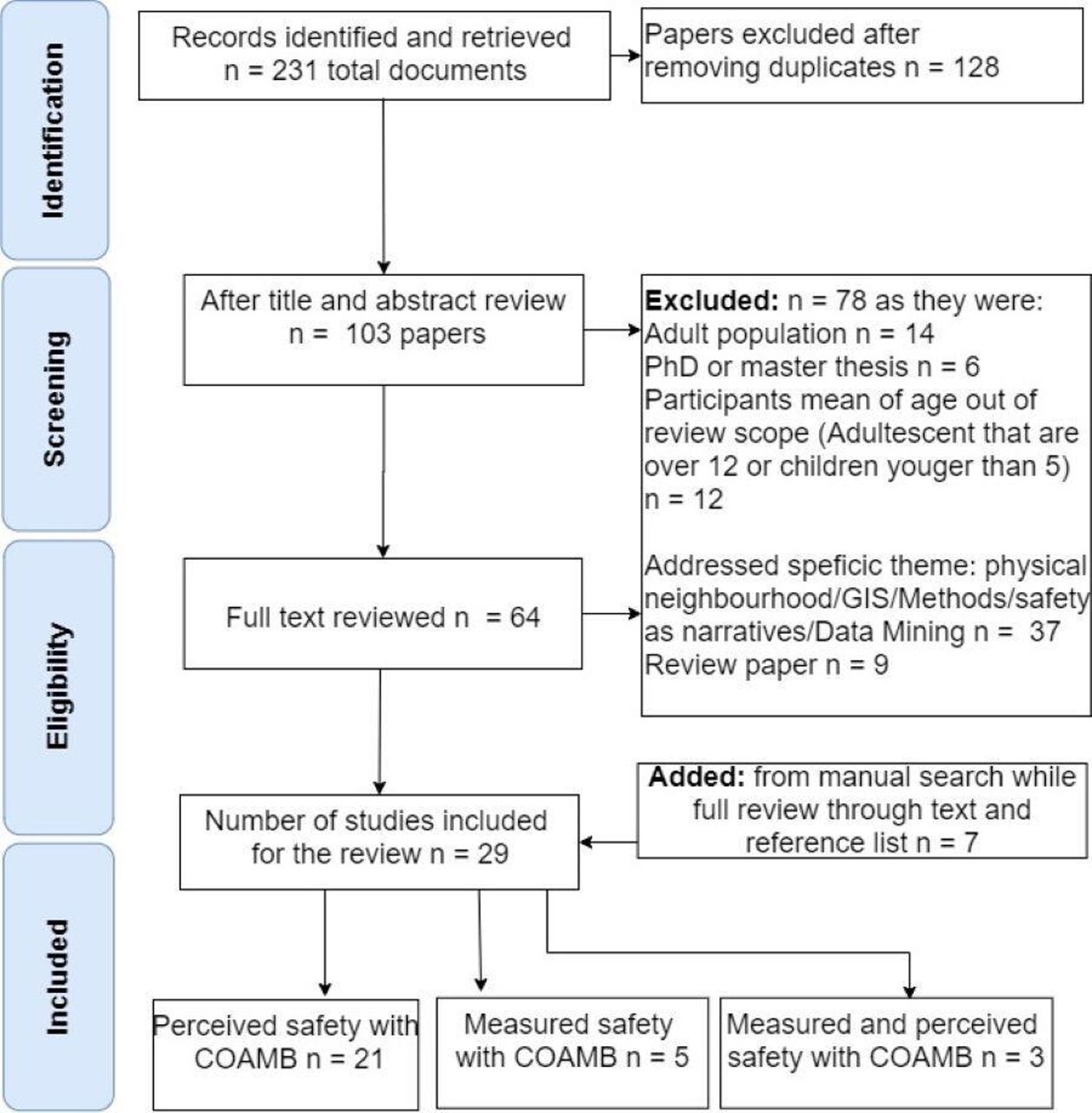
Following the title screening, a total of 231 papers across the six databases were initially identified that deemed potentially relevant. After removing 128 duplicates, the abstract review resulted in 64 articles that underwent a full-text review. Seven additional studies were identified from a manual search of individual reference lists. Following full-text review, a total of 29 studies met inclusion criteria, figure 1.
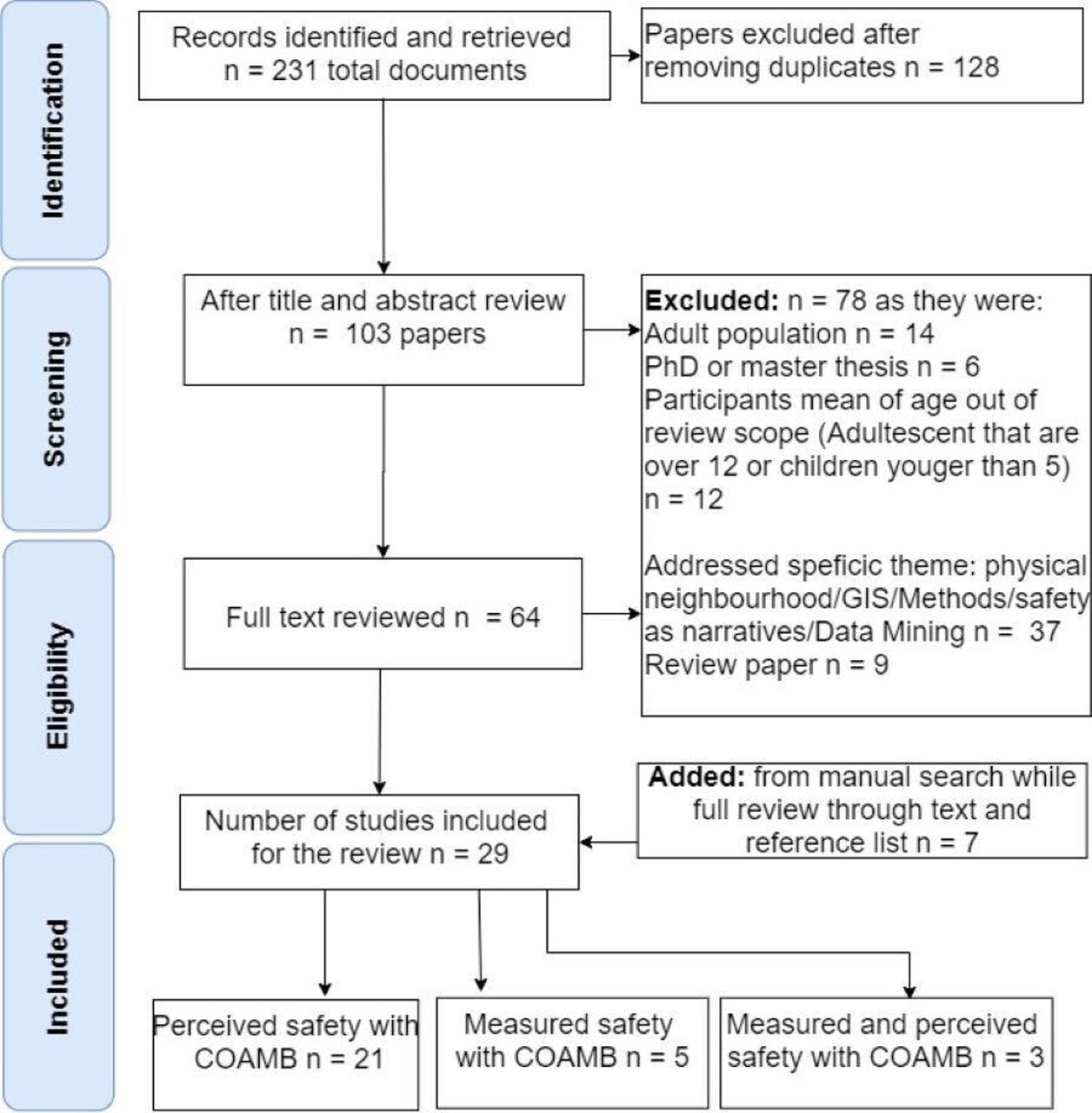
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram for scoping review of neighbourhood safety correlates to children’s outdoor active mobility behaviour (COAMB). GIS, geographic information system.
Study characteristics
The characteristics of the 29 studies, including settings, measurement methods and evidence output, are summarised in table 1 in online supplemental file 2. There were three longitudinal studies,10 33 34 and the remaining (25 studies: 86%) had a cross-sectional design. Twelve of the 29 studies (41%) featured analysis using data from other larger scale or government projects (eg, the Children Living in Active Neighbourhoods study,35 36 the Built Environment and Active Transport project37 and the Spatio-Temporal Exposure and Activity Monitoring (STEAM) project38). Populations varied across studies, with both parents and children represented. The sample sizes ranged from 35 children6 to 31 000 households.39 Studies alternatively used age groups or school grade to refer to children’s age, but the mean ages were within the specified range of 5–12 years. Included works examined associations between forms of COAMB and perceived safety (21 of 29 studies; 73%), measured safety (5 of 29; 17%) or both measured and perceived safety (3 of 29; 10%). Collectively, the publications spanned Asia, Europe, North America and Oceania, Diagram 1 of online supplemental file 2. Aside from two Iranian studies,40 41 and one from Malaysia,42 the remaining publications (26 of 29; 90%) addressed populations in developed countries, with five each from the USA34 43–46 and the UK10 47–49; four each from Canada5 33 37 50 and Australia35 36 51 52; two each from New Zealand53 54 and the Netherlands,7 55 and one each from Portugal,56 Finland6 and Austria.57 Except for one study,58 remaining papers were published between 2007 and 2020. Two studies used BMI34 48 as a measure of children’s active health indices, yet one article has combined BMI with self-reported physical activity. Subjective assessment was the most common method of measurement of children’s active behaviour. Ten of 29 studies (34%) employed objective measures such as accelerometers,35 36 45 pedometers,52 GPS6 alone or in combination with an accelerometer,37 50 53 or GIS loggers.33 In view of the heterogeneity in the measurement methods, disparity in studies’ units of outcome were apparent as exhibited in Diagram 2 of online supplemental file 2. Of 24 studies which examined personal safety, the majority assessed safety as perceived by parents; however, 7 studies featured safety perception among children.5 41 47 49 51 52 58 Five studies7 10 36 50 53 examined objective measures of road safety and 12 studies assessed road danger as perceived primarily by parents. The findings in 25 of the 29 studies (86%) were reported separately for boys and girls.
Methodological quality assessments and strengths in evidence
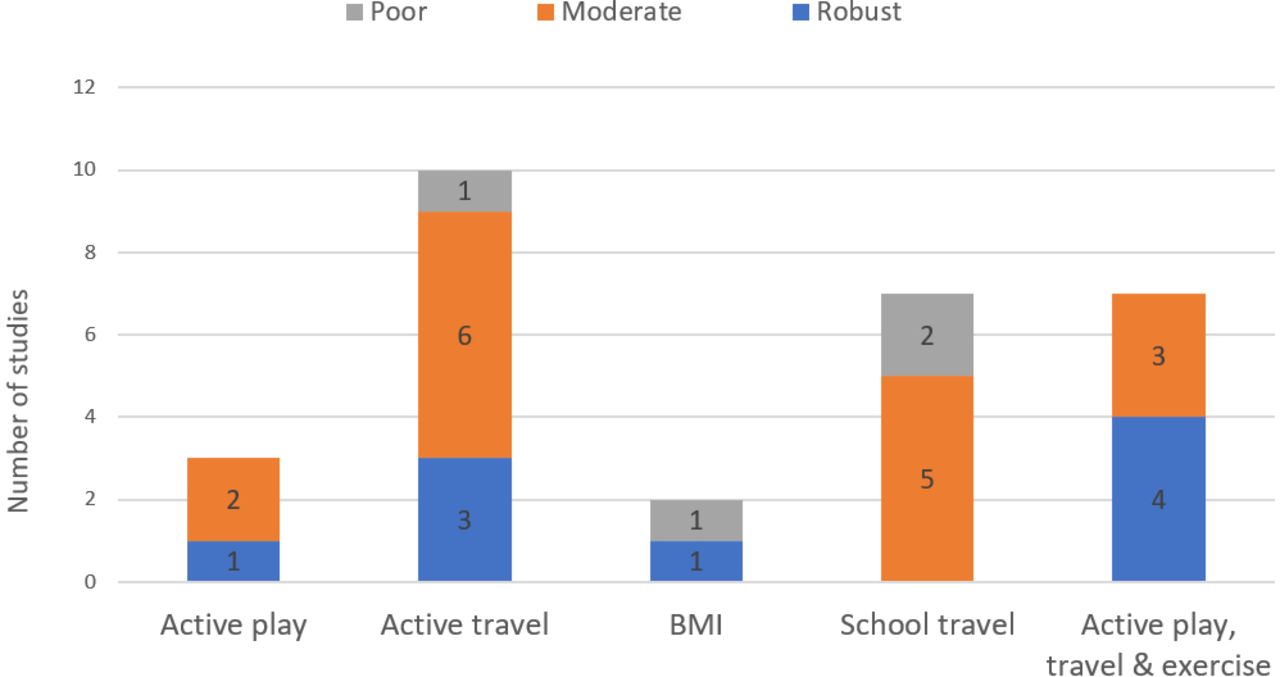
Nine of 29 studies (31%) were rated of robust quality, 16 studies (55%) were of moderate, and four (14%) were rated as poor quality, as presented in table 2 in online supplemental file 2. Most studies focus on correlates of safety to active travel behaviour, such as independent walking or cycling to local destinations. Table 3 in online supplemental file 2 showed that active school travel was the focus in seven of 29 (24%), ten of 29 (34%) addressed active travel, and seven of 29 (24%) addressed active play, active school travel and exercise. Active play alone was investigated in 3 of 29 (10%) studies, and two (8%) used BMI, but one study combined BMI with self-reported physical activity, figure 2.
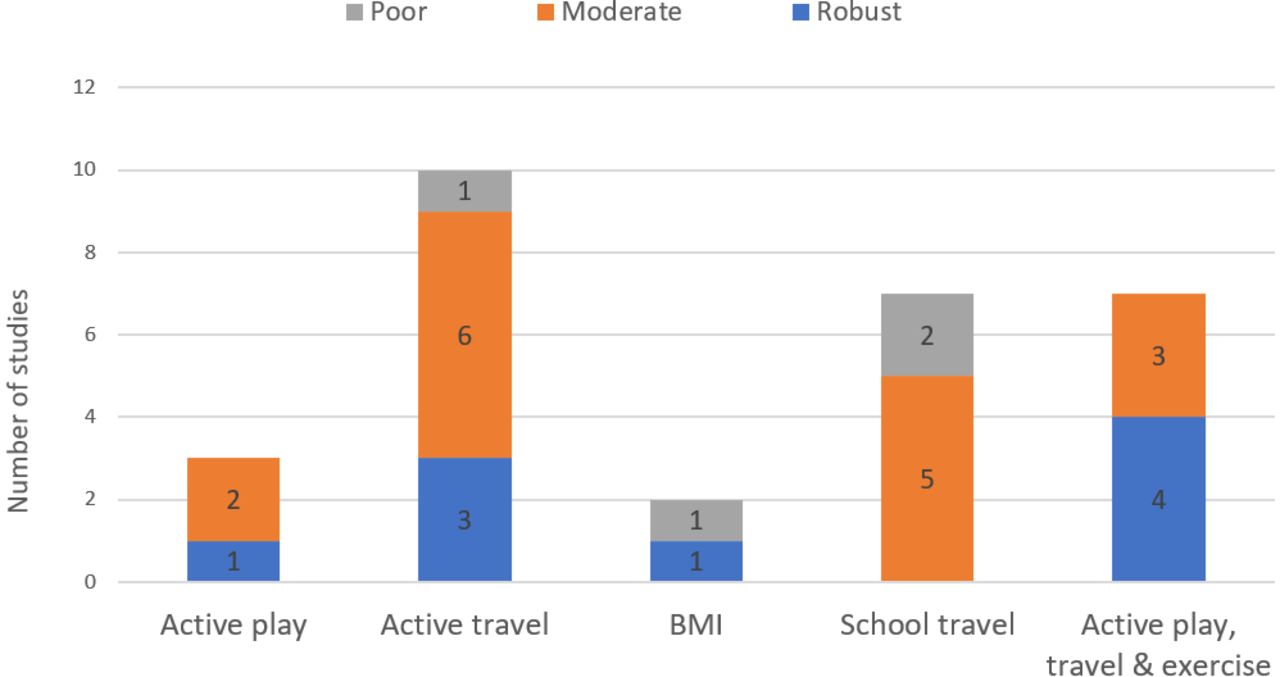
Studies grouped by the type of active behaviour indicating studies’ level of methodological quality assessment. The x-axis represents studies as grouped by type of active behaviour examined in each study. y-axis denotes the number of studies giving the different levels of evidence ‘strength’ when total methodological review score was summed. Strength of evidence was robust when summing total score was ≥66.66% moderate sum was ≥50–<66.6% and poor when an accumulated score was <50%. Adapted from previous review by Schoeppe et al.24
Synthesis of the evidence
Derived from table 4 in online supplemental file 2, we summarised below statistically significant and non-significant correlations in 29 studies examining influences on COAMB by aspects of socioecological levels that were.
Individual level
Without considering safety and supported by strong evidence (40% in 10 out of 15 studies reporting significance and agrees in the direction were of robust quality), we found a correlation between sex/gender and COAMB. A higher level of COAMB was accumulated by males than female children, figure 3. Boys had more active behaviour,44 took more active trips,35 accessed larger activity spaces,52 and increased their active travel of walking or cycling to school,10 or other destinations.52 However, this correlates influenced by: temporal variation between weekdays and weekends,37 time segments of the day (after dark)51 52 or actual distance travelled.6 Similarly, strong evidence (33.3% in 6 studies reporting a significant positive correlation were of robust quality) showed that children of older age groups or higher school grades accumulated more COAMB.

Correlation between individual (child) and family characteristics and children’s active mobility behaviour. The x-axis represents variables that accumulated the minimum number of studies to synthesise evidence of correlates between COAMB and sex/gender, age, access to a car, and ethnicity. y-axis denotes the number of studies that examined the correlation showing accumulated significance or non-significance. Note: *=in sex/gender, we saw variability by temporal characteristics (ie, changes between weekdays and weekends or time of the day (before and after school)) in three studies and reduced COAMB by distance travelled in one study. *=In Race/ethnicity, one study with a significant correlate depicted temporal change (i.e., weekend/weekdays).
Family level
Eight studies found that correlates of COAMB and car ownership were consistently associated with lower levels of COAMB. Despite that, the level of evidence was weak, with only 12.5% of the total studies were robust quality. The inconsistent finding across five studies suggests no clear correlation between ethnicity/race or socioeconomic status (SES) and COAMB. Children of minority groups in the UK achieved lower levels of active behaviour,47whereas children of minority groups in the USA accumulated higher levels of active behaviour.44 In New Zealand, children’s active behaviour differed by race/ethnicity and the day of the week: Indian/Asian background had increased their physical activity levels of medium-to-vigorous (MVPA%) on weekends while Pacific, European and Maori children accumulated higher (MVPA%) on weekdays.53 Findings on (SES) and COAMB were either: non-significant for female children (5–6 years); increased active behaviour in high (SES) groups42 51; inconclusive59; and increased BMI level in a high deprivation area yet reported higher self-physical activity.48
Neighbourhood level
We found strong evidence that increased parental perception of safety correlated with lower COAMB (29.4% of the 17 out of 18 studies reporting significant and agreeing in the direction were of robust quality), figure 4. We found limited and inconsistent evidence on the correlation of ‘stranger danger’ among parents to COAMB; no relationship,54 56 reduced MVPA,45 and has a temporal correlation (son weekdays).37 We found moderate evidence (25% of the 11 studies were rated robust) but consistent in the direction of correlates of higher parental road safety concerns and decreasing levels of COAMB, including one study finding a gender difference (girls). Weak evidence yet consistent (i.e., agree in the direction of the significance) of lower levels of COAMB correlate with children’s increased perception of danger from strangers, roads and personal safety. Limited (four studies) evidence related to children’s perception of personal safety,5 41 49 52 included a study that depicted variation by gender.52 Perception of ‘stranger danger’51 55 60 was insufficiently (three studies) addressed. Road danger47 49 51 52 58 depicted variation in two studies by sex/gender.49 58 Regarding measured safety (i.e., crime or road conditions) and COAMB, a definitive conclusion cannot be drawn despite robust evidence (six out of nine studies are of robust quality),. A synthesis of four studies showed inconsistency in the direction of the relationship with measured personal safety,33 34 45 46 as one study depicted increased active transportation in high crime areas.33 Road danger3 7 10 50 showed increased outdoor active play in highest traffic areas,50 and one study lacked correlation to measured roads environment.36 Other characteristics in the neighbourhood that are likely to be influenced by perceived safety were: strong evidence of distances travelled (perceived or objectively measured) with 10 studies and 40% of robust quality and variability in neighbourhood type (6 studies with 66.6% of robust quality). Other addressed variables demonstrated associations with COAMB, but insufficient evidence to conclude are in table 4 of online supplemental file 2.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Perceived safety (parents and children) of personal and road danger correlates to reported and measured children’s active mobility behaviour. The x-axis represents examined variables that accumulated a minimum number of studies to synthesise evidence for perceived personal and road safety by parents or children. y-axis denotes the number of studies that accumulated significant or non-significance. Note:*=Parents’ perceived neighbourhood safety showing significant correlates included three studies depicting temporal characteristics (weekdays/weekends or before and after school), three studies varied by child’s sex/gender and one study by age. *=For children, perceived personal safety varied by gender in one study.
Discussion
A review of 29 studies investigating multifaceted influences on COAMB and neighbourhood safety prompted the discussion over three primary topics.
Inequality in opportunity for children’s active behaviour
Differences in individual, family, and neighbourhood safety, created an unequal opportunity for COAMB that was ubiquitous across geographical regions, Diagram 3 of online supplemental file 2. Our review depicted variability of COAMB by sex/gender that was predominant in active play and exercise forms of active behaviour than in active travel. This explains lacking of agreement with previous reviews on independent mobility61 and active school travel,22 yet agreed with reviews on physical activity.15 62
Our review suggest that with more access to cars, parents conveniences,22 or other influences such as weather conditions, children at young age are more likely, regardless of their sex/gender, to be driven more often than actively travelling (eg, school trips). However, variability in sex/gender becomes more apparent in physical activity as it is an elective form of active behaviour behind school or government jurisdiction. Increased COAMB with age undetected in previous reviews15 62 could be owned to earlier reviews combining a broad range of children’s age (3–12 years61 or 3–18 years15). A longitudinal study suggested that some forms of active travel (such as school trip) become more prevalent with age, starting from 6 years.60
Studies variability restrained clear conclusions on family race/ethnicity or neighbourhood (SES) correlates to COAMB also concord with earlier reviews findings.20 22 Children from low SES areas in the UK48 were more active. However, children from wealthy families in Australia and Malaysia42 51 had increased active behaviour. Children from less affluent areas may be active by necessity, whereas more accessibility opportunities to open spaces and recreational centres are offered to children from high (SES) areas. A study on obesity rates showed that migrant children (in lower SES) were more active than resident children with higher (SES).63 This socioeconomic influence appeared to reverse its effect on COAMB by geographical location (between developed and developing countries). Nevertheless, we found variation in the correlates of COAMB to (SES) by gender (female children),51 55 60 age group55 and higher income people feeling safer, which in turn encouraged active school travel.55 Despite an agreement with earlier reviews,20 22 the decline in COAMB concerning family ownership of car conflicts with some studies suggesting that wealthier families are more active, thus calling for further investigation.
Every child is entitled to feel safe at all times. Nevertheless, findings of this review suggest a distinct inequality as children living in low perceived safe areas are declined the opportunity to be active. Our finding conflicts with two previous reviews on active travel16 and physical activity,15 respectively. The broad range of children age addressed in the two reviews may have contributed to the disagreements in findings. Parents have a larger influence on younger children’s active health behaviour9 and perhaps hold greater fears regarding road safety for younger children that may not contribute significantly in the older age group, as was explained by a longitudinal national study in the US.64 However, concerns regarding personal safety are nuanced by gender (females),6 35 52 temporal variations (on weekdays only53 or weekends,35 and intersect with gender (females) and temporality when after dark.6 The prevalence effect of ‘stranger danger’ on COAMB among studies surveying children suggests that vulnerability to strangers' harm is more significant for children, particularly for girls.
Influences on COAM are specific to the type of active behaviour
Child’s sex/gender is correlated to COAMB, but most apparent in active play and physical activity rather than active travel. This review also depicted that perceived personal safety risk is most significant in restricting children’s active travel, limiting their active space. This finding concurs with earlier research revealing shrinking children’s active space with the rise of personal safety fears.2 Nevertheless, parents’ concerns over road danger restricted all types of COAMB, Diagram 4 of online supplemental file 2. More active travel was regarded in the urban residential and commercial neighbourhood, was also concluded previously31 suggesting that dense urban area may offer a sense of safety, encouraging more active travel among children. The correlate was also confirmed by the reversed influence of reduced active travel correlates to perceived or measured distance occurred with changes to roads and infrastructure.55
Methodological challenges
The inconsistencies seen in studies investigating neighbourhood safety correlates to COAMB, limit the ability to draw definite conclusions in some areas. Our methodological quality assessment revealed that most studies fulfilled elements relevant to studies reporting but essentially lacked addressing components in the design, method of measurement, and analysis for evidence-based research on children’s active health.32 This may have resulted in the majority of studies were of moderate and poor quality. Subjective measures using questionnaires rely on human recall distant events.65 Yet, we found some inconsistencies among studies employing objective measures. Although a review of measurement methods is out of the scope of this paper, the discrepancies in some of the outcome necessitate highlighting some critical research challenges for future research attention yet were elaborated further elsewhere by Zougheibe et al.32 Study design is likely to affect the outcome. Longitudinal studies limit selection bias associated with cross-sectional design. Inconsistency in the direction of correlates among studies employed objective measures showed most problematic measurement methods were in (1) inconsistent inclusion of crime categories for measured personal safety studies or elements addressed roads conditions, (2) measuring COAMB using spatial activity tracking (i.e., GPS) was faced with an absence of standardised measurement protocols that caused variabilities in few areas such as the inclusion of surveyed days and threshold of counts per minutes of registered data, that could impact a true interpretation of results, (3) the spatial extent of the child’s neighbourhood to derive safety exposures was primarily defined arbitrarily. Still, studies that adopted spatial measures had employed diverse methods, (4) inconsistent accounting for cofounders and (5) infrequent accounting for temporal safety and behaviour characteristics. We found scarcity in research on correlates of COAMB to variation of safety perceived by parents to children residing in the same neighbourhood and actual crime.
Implications of findings
Successful implementation of any intervention strategy to encourage parents and children to embrace an active mobility culture require collaboration among all levels of children, families, schools, community-based organisations, city planners, policy-makers and researchers.28 66 The revealed multiple influences contributing to children’s active behaviour guided our recommendations below.
Interventions for vulnerable groups of the population
Ignoring gendered primary-school-aged children’s active mobility behaviour may result in only male adult’s regarding physical activity as essential or accessible. Therefore, strategies to increase active behaviour must be sex/gender and age specific. Additionally, the indication of influence on COAMB by diverse (SES) and race/ethnic backgrounds suggests that a subgroup of the population is constantly inactive. Parental involvement in educational programmes to promote children’s free play and active travel or children’s encouragement in school and community programmes to participate in active travel and leisure active play could be useful. Earlier evidence also supports the positive influences of active parents56 or positive peer influence.67
Promote child-friendly cities
Revitalise cities design may offer play opportunity and safer travel for children. Perceived low safety linked to declined children’s active travel and its associate to neighbourhood types suggests that current cities and roads designs are maybe seen as unsafe for children to be outdoors actively playing and travelling safely to local destinations independently. Most importantly, interventions intended to encourage children to travel further actively call for redesign of urban structures to enable active travel and safety at the same time. This may include upgrading local features that promote walkability in desirable neighbourhood characteristics (eg, schools, shops, libraries) and active playing in local parks or exercise in an ‘activity-friendly neighbourhood’.68 More voices are calling for children and families to be included in designing new urban spaces. Improvements in road safety may increase overall COAMB and enable children and families to embrace an active mobility culture. Existing streets design is seen as unsafe and unappealing for children and their parents. Prompt policy interventions to address most concerned roads conditions(eg, heavy traffic, fast drivers, high-speed roads, lack of road signals, availability of sidewalks and cycling infrastructure) may alleviate parents’ and children’s concerns over road danger.
Advancing research
Methodological improvements to reduce inconsistency in the outcome and increase reliability in future research can better inform evidence-based policy. Namely: encouraging longitudinal study design and adopting a three-dimensional conceptual framework in research as suggested earlier32 to account for critical elements of (1) what we measure: the determinants that affect the outcome and consistent accounting for cofounders (sex/gender, SES background, and ethnicity/race background), (2) how we measure: involves frequency and intensity for perceived safety69–71 (personal and roads) and active behaviour whether reported or measured consistency in addressing crimes only relevant to personal safety, and (3) spatiotemporal characteristics (i.e., locality of active behaviour or safety incident, spatial extents of children neighbourhoods, and time).72 Further research on COAMB correlates to variability in parents to their children safety perception or measured to perceived safety, and inequality in the neighbourhood (SES) would answer more profound research questions.
Strengths and limitations
This review was limited to English-language and peer-reviewed observational studies. Despite every effort to identify all relevant studies through a variety of terms used, some relevant studies may have been omitted due to multiple synonyms used in works. The observed heterogeneity in study measures prevented a straightforward meta-analysis; thus, we conducted quantitative vote counting to overcome existing disparities in outcome and methods. The majority of studies were cross-sectional design and were of moderate or poor quality. Despite these limitations, this review has important strengths. This work synthesised findings and derived a quantitative understanding of evidence strength by combining a measurement of study reporting quality, involving critical characteristics that may improve reliability in future observation studies. This paper has comprehensively addressed the impact of safety in primary-school-aged children’s active behaviour, eliminating inconsistencies resulting from a broad age range of study participants. To the best of our knowledge, this review is the first to consider the impact of perceived (by parents and children) and measured neighbourhood safety across multiple types of COAMB. Finally, this review was not limited to publication date or geographical region.
Conclusion
This systematic review of evidence revealed that there is inequality in COAMB by children’s sex/gender and age and some indication regarding race/ethnicity and (SES) despite the evidence being inconclusive with regard to the latter two examined variables. Compared with safer neighbourhoods, children living in perceived unsafe areas correlated with lower outdoor active mobility behaviour and reduced active play. However, perceived personal safety risk has primarily restricted children’s active travel to local destinations, whereas perceived danger from traffic reduced every type of COAMB. Nevertheless, the direction and strength of the correlates are affected by individual and family characteristics, distance travelled, and time (weekend/weekday/time of day). These findings were consistent across countries. There is a need to use validated measurement methods. Deeper understanding of safety (perceived or measured) correlates to race/ethnicity,(SES) variances and COAMB (spatial extent of active behaviour or intensity of physical activity) may answer more profound behavioural research questions. Current inequalities in children’s opportunities to engage in active mobility behaviour require sex/gender and age-based interventions. Most importantly, interventions aimed at improving personal safety and engaging children in urban design to promote child-friendly cities may prompt children to travel further actively. Improvements in road conditions may increase overall COAMB and enable children and families to embrace an active mobility culture.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Acknowledgments
The authors thank Jianhong (Cecilia) Xia (CX) for her assistance in assessing studies for inclusion. Additionally, the authors would like to thank the thoughtful comments made by the reviewers and editor from BMJ Open Journal that have helped improve the review considerably.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RZ carried concept/design, data retrieval, screening of the literature for inclusion, quality rating, synthesised the findings, drafted, and finalised the manuscript. BJ assisted in rating of studies quality and contributed to proof editing the overall manuscript. RN, OG and AD reviewed and approved the manuscript.
Funding The first author receives the Australian Government Research Training Program (RTP) scholarship; however, the research received no specific grant from any funding agency in public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.