Article Text

Abstract
Objective To map the physician approach when determining disposition for a patient who presents without the level of definite medical acuity that would generally warrant hospitalisation.
Data sources/study setting Since 2018, our US academic county hospital/trauma centre has maintained a database in which hospitalists (‘triage physicians’) document the rationale and outcomes of requests for admission to the acute care medical ward during each shift.
Study design Narrative text from the database was analysed using a grounded theory approach to identify major themes and subthemes, and a conceptual model of the admission decision-making process was constructed.
Participants Database entries were included (n=300) if the admission call originated from the emergency department and if the triage physician characterised the request as potentially inappropriate because the patient did not have definite medical acuity.
Results Admission decision making occurs in three main phases: evaluation of unmet needs, assessment of risk and re-evaluation. Importantly, admission decision making is not solely based on medical acuity or clinical algorithms, and patients without a definite medical need for admission are hospitalised when physicians believe a potential issue exists if discharged. In this way, factors such as homelessness, substance use disorder, frailty, etc, contribute to admission because they raise concern about patient safety and/or barriers to appropriate treatment. Physician decision making can be altered by activities such as care coordination, advocacy by the patient or surrogate, interactions with other physicians or a change in clinical trajectory.
Conclusions The decision to admit ultimately remains a clinical determination constructed between physician and patient. Physicians use a holistic process that incorporates broad consideration of the patient’s medical and social needs with emphasis on risk assessment; thus, any analysis of hospitalisation trends or efforts to impact such should seek to understand this individual-level decision making.
- qualitative research
- general medicine (see internal medicine)
- health services administration & management
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- qualitative research
- general medicine (see internal medicine)
- health services administration & management
Strengths and limitations of this study
Focuses on admission decision making for a population of patients without the level of definite medical acuity to warrant inpatient care but considered for hospitalisation for other reasons.
Makes use of a novel approach that captures in-the-moment decision making as documented by the physician involved in admission evaluation, thereby avoiding the pitfalls of other retrospective or criteria-based methods.
Examines written narratives from the physician using a qualitative approach to thoroughly capture what factors are considered as well as how the decision is made.
Single-site study conducted in the US where use of triage hospitalists is relatively common, thus findings may not be broadly applicable elsewhere.
Research protocol based on written database entries from one physician’s perspective lacks the ability to probe or clarify information as in an interview process or to integrate multiple physician perspectives.
Introduction
The emergency department (ED) serves a complex role in the US as both the primary route of entry to inpatient hospitalisation and a site of treatment and coordination for patients unable to access care elsewhere.1 2 Identifying which patients require hospitalisation is a key activity that occurs in the ED and has important implications. Incorrectly discharging a patient may risk clinical worsening leading to readmission3 or even death,4 while admitting a patient who does not necessarily require inpatient-level care may risk in-hospital adverse events5 and contributes to overall boarding/crowding and system strain.6
Sizeable variation in admission rates exist by hospital and physician.7 8 While there are differences in individual physician practice styles,9 10 admission rates seem to be more closely linked to community-level and patient-level sociodemographics and comorbidities such as poor perceived access to care,11 low socioeconomic status,12–14 membership in a racial or ethnic minority population,15–17 comorbid cognitive and physical limitations,18 19 as well as substance use or mental health disorders.20 21 Understanding these patterns requires deeper analysis of admission decision making especially for those who present without the severity of illness that would automatically warrant admission; literature in this area is relatively sparse.22–24
It has been reported that factors not directly related to the patient’s acute medical illness such as lack of social support or follow-up, departmental constraints and poor information flow influence hospitalisation,25–29 but there remains need for more comprehensive understanding of the process as a whole. How is the admission decision arrived at and how are various contributing factors integrated into the decision? Additionally, most of the current literature focuses on ED physician perspective even as internal medicine trained hospitalists increasingly serve in the role of ‘triage physician’ providing an inpatient-based acute care screening and approval for admissions.30 31 We propose that hospitalists can provide a useful vantage point from which to learn more about this phenomenon.
In this report, we map the hospitalist triage physician disposition decision-making process for the population of ED patients referred for admission to the acute care medicine service for whom the triage physician assesses that the patient does not have the degree of definite medical acuity to automatically warrant inpatient hospitalisation.
Methods
Study setting
This study took place at a 400-bed, urban, safety-net public teaching hospital and level 1 trauma centre in the US that sees over 60 000 ED visits per year. At our institution, a hospitalist ‘triage physician’ receives all calls for admission to the acute care medical service, reviews details of the referred case and works collaboratively with the referring provider to determine appropriate disposition. The triage physician may make this determination from information relayed by the referring provider, review of relevant data from the clinician record and/or by in-person direct evaluation of the referred patient, if necessary. All triage physicians at our site are faculty within hospital medicine who have completed internal medicine residency training.
Data collection
All admission calls received by the triage physician are logged into a triage database using a standardised REDCap survey32 to capture details, including the triage physician’s assessment of admission appropriateness captured via the question ‘Based ONLY on the medical reason for hospitalization, in your opinion how appropriate is this admission to Medicine floor service?’ followed by the response options ‘Severity of medical problems alone may not require inpatient hospitalization’, ‘Meets ICU criteria/inappropriate or borderline for floor’ or ‘Better served on a different primary service’. In addition, three free-text boxes throughout the tool capture narrative description of the case: one box requests the ‘Chief Complaint’, one box requests ‘Explain’ if the selection ‘Other’ was chosen from a list of contributors to admission and one box solicits general information by asking ‘Issues to address regarding this case?’. All allow unlimited character entry.
Faculty members at our site are introduced to the tool as part of their orientation process with ongoing reminders at regular team meetings, and documentation of admission calls has become integrated into daily shift activities. Description of the triage database tool and its use at our site, including characterisation of overall call volumes, appropriateness assessments and disposition outcomes, has been previously published.33 In addition, we have published analysis of specific factors associated with admission versus discharge from the ED for patients without definite medical acuity27 as well as risk of in-hospital adverse events experienced by this population.5
Entries from the triage database were considered for inclusion in our study if all of the following conditions were met: (1) the admission call originated from the ED between 1 March 2018 and 1 September 2019; (2) the triage physician responded that the admission was potentially inappropriate for admission and selected ‘severity of medical problems alone may not require inpatient hospitalization’; and (3) at least one of the free-text comment boxes contained a response. A total of 300 entries met inclusion criteria, and the corresponding text responses were exported verbatim to Dedoose version 8.036 (SocioCultural Research Consultants, LLC) for qualitative analysis. Light editing was performed to ensure readability and to protect any potential patient identifiers. Entries were not linked to individual triage physician identity.
For clarity, throughout this manuscript, we will refer to the patient cohort as ‘without definite medical acuity’ to reflect the criteria used for selection and to acknowledge that the presence of medical concerns may vary throughout the cases; some individuals may have had no medical issues contributing to hospitalisation decision, while others may have had medical illness that contributed but not to the degree that it was an obvious or compelling reason that definitely required hospitalisation.
Data analysis
Qualitative analysis allows for deep exploration of complicated events, making it well suited to address challenging questions within healthcare and health services research.34 35 We used a grounded theory method to analyse data because this approach is rooted in developing meaning from the data itself without a prespecified hypothesis and focuses on inductive and iterative development of theory to explain findings.36
Members of the entire research team (TT, AE and MB) began by reading the first 25 entries and then reconciled findings to generate an initial code list. Two team members (TT and AE) then continued to independently read and code the remaining entries. During weekly team meetings with the principal investigator (MB), discrepancies were identified and reconciled. In addition, new entries to the codebook were suggested for emerging themes that had not previously been captured. Once thematic saturation was achieved, a comparison sample between coders measured inter-rater reliability with Cohen’s kappa score 0.79. After completion of the first round of coding as the group reviewed and organised the findings, we agreed that enough information was available to encompass what factors were being considered by the triage physicians and how they affected decision making and any additional actions the triage physician took. We revised the codebook slightly to fit this shift in focus and applied the final version to all entries. From here, we built a conceptual model by mapping themes and subthemes into phases of decision making.
To address our reflexivity, we included a research team member who was very familiar with the triage process with previous direct experience serving as a triage physician (MB) and team members who were neither physicians nor familiar with the triage process prior to this analysis (TT and AE).
Patient and public involvement
We did not directly involve patients or the public in this study.
Results
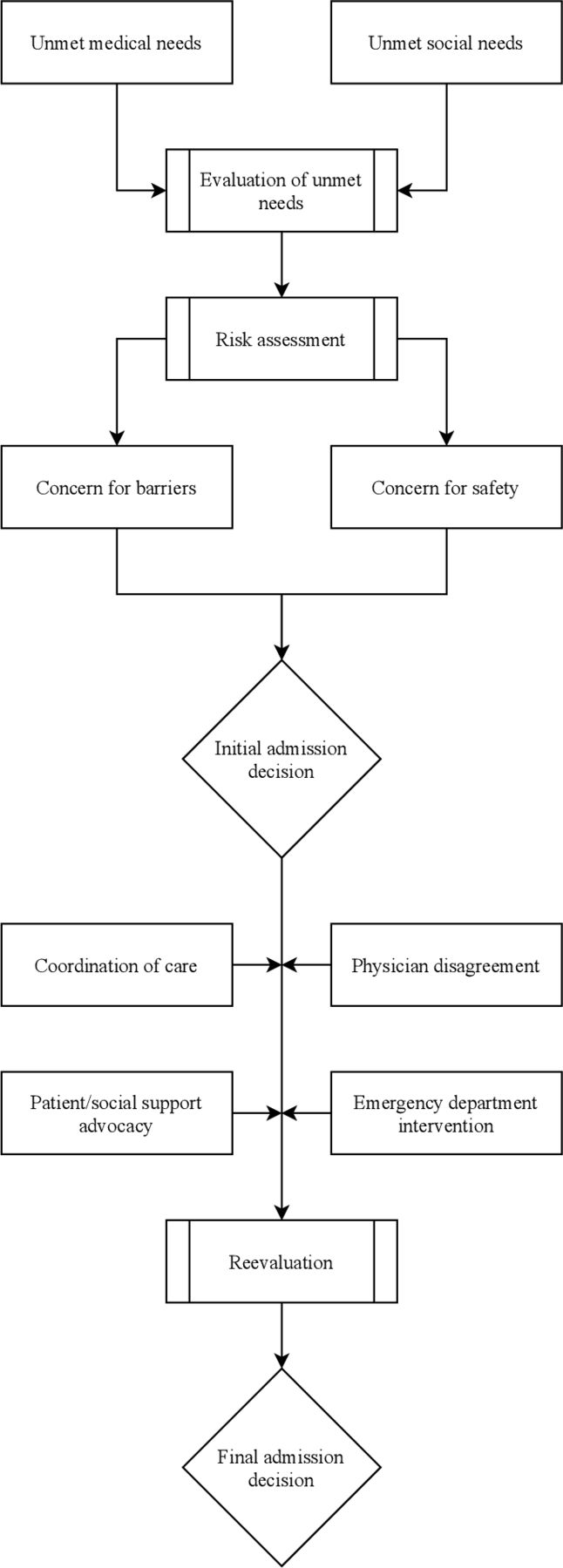
Admission decision making for patients without definite medical acuity proceeds through three main phases (figure 1). First involves obtaining a thorough understanding of the patient’s medical condition and social situation in order to identify unmet needs. This information provides the basis for the second phase, determination of the patient’s overall risk if discharged, during which both barriers to treatment as well as general safety are considered. From here, an initial disposition decision—whether or not to admit to the hospital—is generally made. Subsequently, a third phase may occur in which influences or events external to the patient and triage physician alter that initial decision. Each phase is discussed in more detail below.

{kind=link}
Conceptual model of admission decision making.
Phase 1: evaluation of unmet needs
The admission decision-making process begins with a comprehensive view of the patient’s clinical picture, functional status and living environment. Unmet needs, either medical or social, are identified. See table 1 for representative quotations.
Phase 1: evaluation of unmet needs
Unmet medical needs
The need for clinical services not easily accomplished in the outpatient setting, either because of access or urgency, was considered as part of triage decision making. System-level issues such as lack of specialist availability or inability to coordinate a procedure were common.
New presentations of previously undiagnosed illness with desire for prompt workup (eg, malignancy) and presentations of worsening chronic illness (eg, venous stasis wounds) were both noted. Triage physicians commonly mentioned patient characteristics such as age, functional status or frailty, complex medical history, or concurrent psychiatric or mental health disorder that augmented the way unmet medical needs were viewed, usually making hospitalisation more favoured. In addition, a patient recently or frequently seen in the healthcare setting (ED or hospital) served as an indication to triage physicians that needs from previous visits may not have been appropriately met and prompted additional consideration.
Unmet social needs
The need for support in activities of day-to-day life was considered as part of the triage decision making. Patients presenting for ‘placement’ without specific medical needs who ideally would be cared for in an outpatient setting with services independent of the healthcare system were particularly challenging cases to navigate. Hospitalisation often served as a last resort for connection into a higher level of care or resources unable to be otherwise accessed: ‘Patient does not care for self; admitted for placement but is not a candidate for skilled nursing facility; tried to refer to respite via ED but was declined; need a better resource for patients who need housing’ (#18).
Overlapping unmet needs
There was considerable overlap in cases with both unmet medical and unmet social needs. Unmet medical needs were sometimes driven by a lack of reliable access in the outpatient setting caused by an unmet social need. This could be an explicitly demonstrated lack of access: ‘[patient with brain metastases] just arrived from [foreign country] and needs malignancy workup; not connected into insurance or care’ (#81). Or, sometimes the lack of access was assumed by the physician based on history: ‘[symptomatic anemia] patient seemed to have cognitive impairment and had missed other outpatient appts for work-up; didn't have case manager or anyone at home to remind him to seek care, so it seemed better to admit him and complete his w/u’ (#84). Living alone and lacking sufficient supports to independently manage an illness was cause to consider hospitalisation. In some instances, the medical need was thought to be relatively minor but unable to be provided outside of the hospital due to other social barriers: ‘Patient has COPD, was desatting with ambulation, but probably not much different from his usual baseline. Unfortunately, he lives at [homeless shelter] and cannot be set up with home oxygen’ (#58). Reciprocally, medical illness also served as a barrier to social stability and in fact could create or contribute to an unmet social need: ‘Patient is actually near her baseline from CKD/CHF standpoint, but cannot ambulate to the bathroom quickly enough and is incontinent; was kicked out of her motel and shelters for wetting the bed’ (#215).
Phase 2: assessment of risk
Once a comprehensive picture was created of the patient’s needs, the triage physician used this information to assess the potential risk of harm to the patient if not admitted. Typical areas of concern included any barriers to appropriate treatment as well as any direct threat to the patient’s safety outside of the hospital. See table 2 for representative quotations.
Phase 2: assessment of risk
Concern for barriers
Triage physicians often referenced the unmet needs identified in the first phase of decision making as they interpreted the potential risk the patient faced if discharged. Specifically, they strongly considered whether any unmet medical or social needs would impede the patient’s ability to complete appropriate treatment for their medical issues: ‘if patient were housed and not with [schizophrenia/psychosis], could have discharged [with oral] meds, but patient is not reliable enough to do this safely’ (#69). Previous patterns of action also contributed to concern and shaped admission decisions: ‘has no-showed to clinic visits and has been repeatedly going to the ED instead. We admitted for expedited workup given his inability to follow through’ (#100). Depending on the presenting medical issue, confidence in the ability to contact the patient with results also played an important part of decision making.
Concern for safety
Regardless of medical acuity, many times physicians expressed safety concerns driven by situational context such as what living conditions a patient would return to and incorporated this concern into their decision making. Time of day, specifically discharge late at night, compounded the concern; this was especially common with patients experiencing homelessness if the admission decision was being made at a time after access to homeless shelters had closed. In addition to chronic vulnerability, an acute decrease in functional status (eg, intoxication) raised concern for safety. External threats to safety such as return to an unsafe living environment in the case of domestic violence or neglect were also noted.
Phase 3: re-evaluation
After the first two phases, the triage physician generally had an admission decision in mind. However, patient care is not a unilateral interaction, and external influences or opinions could cause a change in plan. We identified these factors to be coordination of care, patient and/or social support advocacy, physician disagreement and ED interventions. See table 3 for representative quotations.
Phase 3: re-evaluation
Coordination of care
Physicians commonly consulted with or involved other parties in providing care to ensure the patient could be safely discharged; this was often used when the triage physician saw an opportunity to avoid hospitalisation. In cases where coordination of care was attempted, the discharge outcome was determined more by the success or failure of the coordination attempt rather than the triage physician’s assessment of appropriateness. Patients who might otherwise have been admitted for an unmet medical need often could have their course changed if the specialist was able to evaluate the patient or perform a necessary procedure in the ED. Coordination of care was also used to address the perceived risk of discharge. Triage physicians described communicating with outside providers in order to satisfy the concern about ability to follow-up. In some cases, this was helpful to provide confidence that the patient would have ongoing support, and in others, it provided additional information that corroborated the concern.
Patient/social support advocacy
At times, patients, their families and/or their outpatient network contributed to the discussion of appropriateness of admission. If a patient or someone in their support system was strongly in favour of admission, this was heavily weighted in the decision.
Physician disagreement
Different members of the care team may come to different risk assessments and ultimately different admission decisions. Because each of the patients in this study was called for admission to the acute care service, the ED physicians were generally in favour of admission, while the triage physicians questioned whether the admission was necessary. At times, specialists, primary care physicians or other physicians were also involved in the discussion. While consensus was usually able to be found through shared decision making between all parties, some triage physicians voiced that these situations were ‘not worth fighting over’ (#180) or that they ‘gave in to the ED’ (#269) by deferring to ED decision making. Lack of triage physician time or competing demands also contributed to a reversal of the triage physician’s initial disposition decision: ‘didn’t have time to actually go down to ED to deal with [admission discussion] due to overflow census issues…’ (#283).
ED intervention
Finally, activity that occurred within the ED had the ability to change the course of the admission decision. An adverse event such as medication reaction in the ED while awaiting an admission decision usually resulted in hospitalisation. In contrast, sometimes with additional monitoring or interventions, the patient’s condition improved or stabilised enough for discharge. The triage physician suggested these additional interventions at times, but they also could be part of the management provided by the ED team.
Discussion
This study analysed free-text entries by triage physicians describing their admission decision making for patients they considered not to have the degree of definite medical acuity that would generally warrant hospitalisation. We found that the decision-making process occurs in three main phases: evaluation of unmet needs, assessment of risk and re-evaluation. Our study highlights that patients who present to the ED without a definitive medical reason for admission may still raise concern and that physicians take a holistic approach to admission decision making in this setting. This work builds on previous studies by describing the decision-making process in its entirety and by demonstrating how contributing factors are integrated into the decision.
Our findings are congruent with previous research indicating that physicians commonly operate outside the guidance of clinical risk scoring tools that stratify patients into those appropriate for admission vs discharge.37–39 Clinical uncertainty40 has been posited as a key underlying driver in these guideline-discordant admissions; our findings take this one step further and suggest that the mechanism by which uncertainty leads to hospitalisation is via the concern for an unmet need that leads to perception of elevated risk if discharged. Furthermore, we propose that our model provides deeper context to understand findings in healthcare utilisation literature. For example, despite focused attention, so-called ‘inappropriate’ admissions (in which patients do not receive inpatient level care and therefore are thought not to have benefited) continue to be prevalent.41–44 We found that physicians thoroughly considered the provision of a safe disposition; when structures around patients were inconsistent or unreliable and this placed the individual at risk, hospitalisation was considered but generally not until other options had been significantly explored. Thus, the term ‘inappropriate admission’ is an oversimplification of the phenomenon and requires broadening to encompass the full capacity of concerns being addressed at time of admission.
Likewise, the model proposed in this manuscript expands on the notion of what has been called ‘unwarranted variation’ or ‘variation that we couldn’t explain based on the basis of illness, patient preference, or medical science’45 by identifying that physicians make decisions with their patients in a broader context than the purely biomedical. Sutherland and Levesque’s46 analytic framework published in 2020 describes ‘warranted variation’ through the three key perspectives of capacity (intractable resource constraints and unpredictable events; proficiency-based service delivery), agency (patients’ needs; patients’ informed expectations) and evidence (judgement used to interpret and apply evidence in local context; equivocal evidence or diffusion of innovation). In this light, much of the admission decision-making process outlined in this study reflects components of warranted variation. Each individual healthcare site and surrounding community has its own mix of resources that influence provision of care for any unmet medical and social needs identified. Each patient has a unique set of individual circumstances, social factors, environmental details and health requirements. Each provider must navigate these complex situations to determine the appropriate risk/benefit litmus for admission versus discharge. In a space in which there exist such wide-ranging considerations, very little comprehensive guidance, and a potentially high-stakes decision, then, it is not entirely surprising to see prognostic variability and decision-making heterogeneity, manifested in our study as both the initial discrepancy between referring ED provider (who called for admission) and triage physician (who questioned the definite need for such) as well as the ‘physician disagreement’ identified as a phase 3 theme.
The discordance between providers in making this decision has been consistently noted elsewhere in the literature33 47 48 and appears to be multifactorial. This may be associated with hospitalists increasingly taking on duties that historically have been within the scope of either an ED physician or primary care physician. In the triage physician role, hospitalists serve as an intermediary of sorts to review the call for admission, problem solve as able and efficiently move the patient along to ultimate disposition. As we describe, they often attempted to intervene in aspects of care coordination with varying degrees of success. Importantly, the locus of control did not rest solely within their purview, and they were significantly impacted by the opinions and actions of other physicians in the care continuum. Additional study of this role, its relationship with other important members of the admission process and formulation of best practices is warranted.
This study is limited in its focus on one institution and may not be generalisable to all sites. We focused on patients without definite medical acuity and did not include those with severe medical illness. Because of the study design, we did not evaluate all patients in the ED without definite medical acuity, only those who were referred to the acute care medical ward for admission, and thus this reflects a smaller sample of the patients overall. We used free-text responses entered around the time of the decision, and this in-the-moment capture is a strength of our method. However, we were unable to probe for more depth or understanding through interactions such as what would be allowed during an interview format.
We conclude that the intertwined nature of our healthcare and social support systems cannot be unlinked from the admission decision-making process and that understanding physician determination of unmet needs and assessment of risk is central to full conceptualisation of this phenomenon. Any interventions aimed at affecting hospital utilisation must take these considerations into account.
Data availability statement
No data are available.
Ethics statements
Ethics approval
This study was approved under expedited review/minimal risk by the University of Washington Institutional Review Board (Study #6948), and the requirement for consent was waived.
References
Footnotes
Presented at An abstract summarising this work was accepted to the Society of Hospital Medicine 2020 National Conference but was not presented due to COVID-19.
Contributors MB was primarily responsible for initial conception of the project. TT and AE performed the majority of initial coding and data analysis with oversight by MB. All three authors collaboratively interpreted the findings, and all are responsible for the contents of the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.