Article Text

Abstract
Introduction Squamous cell carcinoma of the anus is a common cancer among sexual minority men, especially HIV-positive sexual minority men; however, there is no evidenced-based national screening protocol for detection of anal precancers. Our objective is to determine compliance with annual anal canal self-sampling or clinician-sampling for human papillomavirus (HPV) DNA.
Methods and analysis This is a prospective, randomised, two-arm clinical study to evaluate compliance with annual home-based versus clinic-based HPV DNA screening of anal canal exfoliated cells. The setting is primary care community-based clinics. Recruitment is ongoing for 400 HIV-positive and HIV-negative sexual minority men and transgender persons, aged >25 years, English or Spanish speaking, no current use of anticoagulants other than nonsteroidal anti-inflammatory drugs and no prior diagnosis of anal cancer. Participants are randomised to either receive a swab in the mail for home-based collection of an anal canal specimen at 0 and 12 months (arm 1) or attend a clinic for clinician collection of an anal canal specimen at 0 and 12 months (arm 2). Persons will receive clinic-based Digital Anal Rectal Examinations and high-resolution anoscopy-directed biopsy to assess precancerous lesions, stratified by study arm. Anal exfoliated cells collected in the study are assessed for high-risk HPV persistence and host/viral methylation. The primary analysis will use the intention-to-treat principle to compare the proportion of those who comply with 0-month and 12-month sampling in the home-based and clinic-based arms. The a priori hypothesis is that a majority of persons will comply with annual screening with increased compliance among persons in the home-based arm versus clinic-based arm.
Ethics and dissemination The study has been approved by the Medical College of Wisconsin Human Protections Committee. Results will be disseminated to communities where recruitment occurred and through peer-reviewed literature and conferences.
Trial registration number NCT03489707.
- gastrointestinal tumours
- epidemiology
- public health
- HIV & AIDS
- preventive medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This trial will randomise 400 persons at increased risk for anal cancer to home-based or clinic-based collection of anal canal exfoliated cells at 0 and 12 months to determine preference for either the home-based or clinic-based collection.
Persons in the clinic-based arm may choose to attend any one of the five geographically dispersed clinics in a medium size, US city.
At study end, all persons will be asked to receive high-resolution anoscopy to allow assessment of the association between high-risk human papillomavirus persistence and precancerous lesions.
Recruitment into this trial is by convenience sample and, thus, enrollment may favor persons concerned about anal cancer.
Introduction
Persistent infection with high-risk human papillomavirus (hrHPV) is virtually a necessary cause of squamous cell carcinoma of the anus (SCCA).1 In the USA, incidence of and mortality from SCCA has increased in recent decades,2 and is now a common cancer among sexual minority men (SMM) especially HIV-positive SMM among whom incidence is 40-fold to 50-fold higher than in persons overall.3–5 Since it will be decades before the benefits of HPV vaccines are fully realised,6 screening for anal precancers and invasive disease is needed.
Screening may include Digital Anal Rectal Examinations (DARE) for early detection of invasive SCCA among HIV+ SMM,7 while Pap cytology and biopsy-directed high-resolution anoscopy (HRA) have been used to identify precancerous lesions8 9; however, there is no consensus on the optimal screening strategy and few HIV+ SMM are screened.10
Cervicovaginal self-sampling increases use of cervical cancer screening and a similar approach may be useful for anal cancer screening.11 12 SMM are able to self-sample the anal canal and find it acceptable.13–16 Self-sampling may also address healthcare access barriers like embarrassment with anogenital physical examinations,17 or a history of poor healthcare due to having a minority sexual orientation,18 in addition to barriers to cancer screening imposed by the COVID-19 pandemic.19 However, there are few empirical data that assess return rates of home-testing swabs among SMM20–22 and, to our knowledge, none that also report the adequacy of the specimen for HPV DNA genotyping (table 1). Furthermore, transgender individuals who share behavioural risk factors for hrHPV with SMM may uniquely benefit from self-sampling options (eg, reduced gender discordance).23
Studies including self-collection of anal swabs with home-sampling return rates and/or specimen adequacy
In addition, there are no data on acceptability when anal cancer screening methods are repeated over time. Although one-time HPV DNA screening is of little or no value for SMM given hrHPV prevalence that often exceeds 50%,24 25 annual repeated screening allows detection of persons with potentially clinically relevant hrHPV persistence who are at increased vulnerability for anal high-grade squamous intraepithelial lesions (HSILs).26 Other biomarkers may also have utility in anal cancer screening including DNA methylation testing of HPV and human genes. Methylation patterns of host and virus accurately predict cervical HSIL, but are much less studied for anal HSIL.27 28
This study protocol is designed to test approaches that may inform future screening programmes. These approaches are focused on the following 4 of 10 screening characteristics that are considered essential for successful public health screening programmes29: (1) using a screening method that is acceptable, (2) using the screening method repeatedly, (3) having a suitably sensitive and specific test for detecting disease and (4) having a test that is considered cost effective.
Primary objective
To determine compliance with annual anal canal self-sampling or clinician-sampling for HPV among Milwaukee, Wisconsin HIV+ and HIV– SMM and transgender persons, aged >25 years.
We hypothesise that a majority of persons will comply with annual screening with increased compliance among persons in the home-based arm versus clinic-based arm.
Secondary objectives
To determine estimates of the relative ability of home-based screening to increase annual screening compliance.
To estimate the influence that home-based versus clinic-based screening has on the uptake of HRA-directed biopsy.
To estimate the cross-sectional association between hrHPV persistence and detection of anal high-grade squamous epithelial lesions.
To estimate the association between host and viral genome methylation patterns and detection of anal high-grade squamous epithelial lesions.
Methods and analysis
Trial status
Trial design
This is a prospective, randomised, two-arm clinical study to evaluate compliance with annual home-based versus clinic-based sampling of anal canal exfoliated cells for DNA-based testing among HIV+ and HIV– SMM and transgender persons. At study entry, persons randomised to arm 1 will receive a home-based collection swab in the mail at 0 and 12 months, and those randomised to arm 2 will attend a clinic where a clinician will collect the exfoliated cell specimen at 0 and 12 months. Then, all persons will receive a clinic-based HRA-directed biopsy to assess precancerous lesions by study arm. Study start date was 12 March 2019. The study is currently recruiting participants. Study enrollment began 9 January 2020, was suspended due to the COVID-19 pandemic on 14 March 2020 and then resumed on 3 November 2020. Study completion date is 31 August 2022.
Study setting
The Prevent Anal Cancer (PAC) Self-Swab Study is based in Milwaukee, Wisconsin, a Midwest US city with a metro population of 1.6 million. The city of Milwaukee is racially and ethnically diverse with 46.0% of the population white, 39.2% black and 18.2% Latino according to the US census 2015 estimate.
The trial will use the existing healthcare infrastructure in Milwaukee. Persons enrolled in the study can choose to attend one of the five geographically dispersed clinics in the Milwaukee area for anal canal sampling. Each participating clinic has a history of providing specialised medical care to SMM, transgender persons and/or persons with HIV.
Eligibility criteria
Inclusion criteria: Persons will be Milwaukee metro-area residents and >25 years of age. There is no upper age limit. Persons must identify as SMM or a transgender person who has sex with men and speak either Spanish or English. Persons are included without regard to anal cancer screening history, HIV status or HPV vaccination status.
Exclusion criteria: Persons are excluded if they report a prior diagnosis of anal cancer, the use of clopidogrel, warfarin, apixaban or another anticoagulant other than aspirin or non-steroidal anti-inflammatory drugs, a diagnosis of haemophilia, cirrhosis with bleeding varices or thrombocytopenia. Persons are also excluded if they are not willing to attend one of the five study clinics or have plans to move away from Milwaukee in the next year.
Participant recruitment
Persons in Milwaukee are encouraged to join a study of anal cancer screening, with no mention of self-sampling, to attract participants who may have diverse views about self-sampling. Study recruitment uses convenience sampling using the following strategies: (1) social media advertisements to reach persons outside of clinics and thus possibly benefitting more from home-based screening30; (2) recruitment in clinics that serve SMM and transpersons, (3) distribution of promotional materials in targeted businesses and non-profits; (4) a referral programme whereby enrolled participants receive incentives to recruit partners, friends and family; (5) word of mouth and (6) presentations to community groups. All persons are directed to a short online survey that assesses eligibility and basic demographics. The study’s recruitment targets are a minimum of 50% of participants will be HIV-positive, the median age will be ~50 years, and the racial and ethnic composition will reflect the population of Milwaukee.
Randomisation
Immediately after enrollment, persons are randomised in a 1:1 allocation to either the home-based or clinic-based sampling using a study-generated randomisation table within Research Electronic Data Capture (REDCap) (Vanderbilt University) which assigns a study arm to each participant. Given obvious differences of each arm, randomisation cannot be blinded to study staff or participants.
Interventions
At baseline, persons randomised to the intervention arm are mailed a ‘PAC Pack’ to their home which is a package lined with foam that contains supplies for self-sampling (figure 1). The PAC Pack design was informed by a community advisory board and was pilot tested. It includes a FLOQSwab (Copan Italia, Brescia, Italy), a vial of 2.0 mL of Standardized Transport Medium (STM; Digene Corporation), a biohazard bag, gloves and a device to record ambient temperature (LogTag Recorders, Auckland, New Zealand) and instructions for self-sampling based on the Darragh and Winkler31 protocol for anal canal sampling. Participants immediately immerse the used-swab in the vial of STM and are asked to return the swab as soon as possible. Return overnight postage is included for shipment to the Medical College of Wisconsin Tissue Bank. One week after the PAC Pack is sent to participants, they are reminded, via preferred method of communication (eg, text or email), to use and return the PAC Pack, after which an online computer-assisted self-interview (CASI)32 33 assesses participants’ acceptability of the PAC Pack.

Study activity: home and clinical flow activities. DARE, Digital Anal Rectal Examinations; HPV, human papillomavirus; HRA, high-resolution anoscopy; PAC, Prevent Anal Cancer.
At baseline, persons randomised to the control arm are asked to make an appointment at a participating study clinic for anal canal sampling. PAC study appointments can be scheduled throughout the week at times that are convenient to the participant. The attending clinician (either a physician or nurse) collects exfoliated cells with the same flocked swab as used in the PAC Pack while also using the Darragh and Winkler sampling protocol (eg, twirling the swab, counting slowly to 10 and applying pressure to the anal canal walls) in addition to performing a DARE.31 34 Participants are encouraged at the clinic to take advantage of other clinic services like sexually transmitted infection testing and HPV vaccination. Participants then assess clinician sampling acceptability using a CASI. The swab is then transported to a laboratory for processing and storage until biomarker assessment.
Twelve months after baseline, persons again complete the same primary study activities assigned to them at randomisation, that is, mailed a PAC Pack or asked to attend a clinic for sampling regardless of their compliance with study activities at baseline. In between the baseline and 12-month study activities, study staff contact participants in ways typical of medical clinics (eg, to send birthday greetings). We chose annual screening based on our studies estimating that 12% of SMM will have 12-month persistence with hrHPV (suggesting increased risk for anal cancer and thus needed HRA),35 expert opinion on anal screening intervals for HIV+ SMM,36 and because it is a familiar interval that may encourage repeat screening.
After 12-month study activities, all persons are asked to schedule an HRA regardless of compliance with home-based sampling or clinic-based sampling. All suspicious lesions are documented and biopsied. If no lesions are seen on HRA, then two biopsies are taken from two quadrants of the anal canal to assess sensitivity of the anoscopist’s negative findings. All anal biopsies will be interpreted by a single experienced pathologist using a two-tiered system (low-grade squamous intraepithelial lesion and HSIL, and further classified by the applicable anal intraepithelial neoplasia (AIN) subcategorisation (AIN1, AIN2 and AIN3) with subsequent p16 staining as necessary.37
Clinician training
Physicians and nurses seeing study participants complete mandated in-person training in anal canal sampling31 and DARE34 led by a nurse practitioner and the principal investigator. In addition to anal swab and DARE technique and documentation, clinicians are trained in anal cancer epidemiology and study objectives. The training includes DARE practice on a task mannequin (Kyoto Kagaku, Kyoto, Japan). HRA-directed biopsies at the Medical College of Wisconsin/Froedtert Anal Dysplasia Program are performed by the nurse practitioner with advanced HRA training and >300 HRAs completed.
Computer-assisted self-interviews
CASI data in English and Spanish are collected at four timepoints (study start, postbaseline swab, post 12-month swab and post-HRA) to provide data about modifiable and non-modifiable factors associated with annual screening. CASI items include questions about anal cancer susceptibility, PAC Pack and clinician screening acceptability, HRA acceptability, screening self-efficacy and anxiety, medical history, sexual behaviour, substance use, measures to inform cost-effectiveness and the COVID-19 pandemic. When possible, questions were adapted from validated cervical cancer screening instruments within the framework of Health Belief Model constructs38 like perceived susceptibility for anal cancer and barriers to and benefits of anal cancer screening. CASIs were refined through cognitive interviews and pilot testing.
Participants receive US$35 for completion of the baseline activities, US$45 for 12-month activities and US$50 for HRA.
Biomarker testing
Swab specimens transported to the Medical College of Wisconsin Tissue Bank are processed and then aliquoted into cryovials for transport to laboratories for genotyping and methylation testing. Cryovial specimens are blinded as to study arm.
HPV genotyping: At the Moffitt Cancer Center and Research Institute, DNA will be extracted from all specimens using the robotic MDx Media Kit (Qiagen), according to the manufacturer’s instructions. The HPV SPF10 PCR-DEIA-LiPA line probe assay system is used to detect 25 HPV genotypes by reverse hybridisation technology: HPV6, 11, 16, 18, 31, 33, 34, 35, 39, 40, 42, 43, 44, 45, 51, 52, 53, 54, 56, 58, 59, 66, 68/73, 70 and 74. Positive (CaSki and SiHa) and negative controls (C33A) are used during genotyping along with detection of human beta-globin to assess specimen adequacy.39
To avoid persistence misclassification, persons with hrHPV type-specific concordance at 0 and 12 months have specimens classified according to HPV-type variant at the Molecular Biology Laboratory, Centre of Translational Oncology, Instituto do Câncer do Estado de São Paulo, São Paulo, Brazil.40 41 HPV variants differ by mutations in specific positions within the viral DNA. Thus, HPV variant analysis will be performed by sequencing of viral DNA fragments amplified by PCR.
At Queen Mary University of London methylation assessment of the host tumour suppressor gene EPB41L3 will be done for all specimens regardless of HPV genotype positivity while all specimens that are hrHPV+ will also be assessed for viral methylation patterns. Assessment of methylation will be performed using sodium bisulfite conversion (EZ DNA Methylation Kit, Zymo Research, CA, USA) and pyrosequencing. Specimens will be evaluated using the S5 classifier DNA methylation panel42 with the S5 score determined using a weighted average of DNA methylation scores from CpG regions on EPB41L3 and HPV16, 18, 31 and 33 late regions.28
Clinical management
Regardless of study arm, participants receive a DARE at study start to rule out palpable masses or other symptoms that may indicate malignancy. Anal canal and perianal symptoms are recorded on standardised forms. During DARE and HRA procedures, standard clinic protocol is used for treating and/or referring for follow-up all persons with suspicious lesions or symptoms.
DNA testing for anal precancer screening is not approved at this time by the US Food and Drug Administration (FDA) and is rarely used in clinics to screen patients. This is especially true for high-risk populations like SMM given their high prevalence of anal HPV which results in low specificity for one-time HPV DNA screening43; thus, genotyping results are not given to participants with the following exception: participants with type-specific, persistent infection with a hrHPV genotype, as indicated by genotyping tests at both baseline and at 12 months, will be notified by the clinician and counselled to adhere to regular contact with a knowledgeable physician to assess future anal cancer risk. Methylation assay results will be compared with HPV testing performance and for their ability to detect high-grade lesions but will not inform clinical management.
Outcome measures
The primary endpoint is the return of a completed PAC Pack or the completion of a clinic visit at both baseline and 12 months. The secondary outcome measures are as follows: (1) factors associated with screening compliance at baseline and 12 months, (2) attendance at an HRA appointment, (3) the association between hrHPV persistence and HSIL and (4) the association between host/viral methylation and HSIL.
Power
Our primary outcome is compliance with sampling at both baseline and 12 months. We will compare the proportion of persons in compliance in the home-based arm and in the clinic-based arm using a Mantel-Haenszel test for difference in proportions in a stratified design. Assuming 200 persons in each arm, we can approximate a lower bound for our power assuming a χ2 distribution with 1 degree of freedom.44 We estimate 10% loss to follow-up (eg, moving away) at 12 months (n=180) and 80% of persons will return a home-collected swab (144) for 72% compliance at 12 months (ie, 144/200).20 Using the same algorithm with cervical cancer screening compliance data,45 we estimate 70% of clinic-based attendees at baseline and 60% at 12 months also with 10% loss to follow-up (200×0.9=180; 180×0.60=108 or 108/200=54% compliance). Using intent to treat, if 144 home-collected swabs (72%) and 108 clinic-collected swabs (54%) are returned at 12 months, and assuming two-sided tests and α of 0.05, we have 84% power to detect a difference (0.18) between arms (table 2).
Power to detect difference in proportion of DNA samples received: home-based versus clinic-based
Data plan
Data collection: Data are collected through (1) participant completion of CASIs; (2) staff recording of participant biometrics and (3) clinician recording of anal sampling and DARE results. CASIs are used during eligibility screening, at baseline, postsampling at 0 and 12 months (home and clinic), and post-HRA.
Data analysis: Our primary analysis is to compare the proportion of those who comply with 0-month and 12-month sampling in the home-based and clinic-based arms. Our primary endpoint, compliance, is categorised as ‘Yes’ if a swab is returned at 0 and 12 months and ‘No’ otherwise. The proportion of PAC Packs and clinic visits completed at 1, 3 and 6 months after the 0-month and 12-month timepoint will be assessed. The null hypothesis is that the proportion of those complying in each arm is the same with assessment by a Mantel-Haenszel test for difference in proportions. After randomisation, persons randomised to arm 1 who ‘crossover’ and attend a doctor’s visit for anal cancer screening, including DNA collection, without returning a home-base PAC Pack, will be counted as non-compliant. Under the intention-to-treat principle, all participants who are randomised are included in the analyses (both primary and exploratory). For sensitivity analysis, per protocol analysis will be performed with data from compliant participants. Compliance can be estimated without dependence on specimen adequacy or compliance with HRA.
To determine Health Belief Model constructs, for example, self-efficacy, that are associated with compliance, purposeful modelling strategies will be employed.46 Bivariate logistic regressions will be performed for each factor, and those factors with a p value <0.25 in the bivariate analysis will be included in a multivariable logistic regression model. Intermediate variables will be excluded from multivariate modelling in Aim 2.47 Associations in the multivariable model will be considered significant with a p value of <0.05. Adjusted and unadjusted ORs will be reported with 95% CIs. We will regress compliance on covariates after adjusting for potential confounders identified with directed acyclic graphs.48
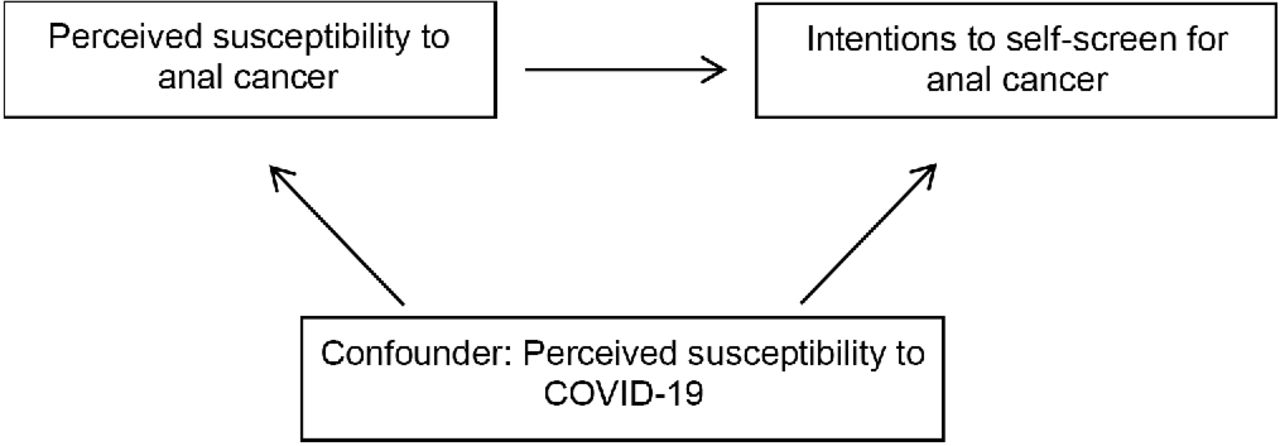
The COVID-19 pandemic is a potential confounder of the association between perceived anal cancer susceptibility and intentions to screen for anal cancer because COVID-19 may affect a person’s perceived susceptibility for diseases like anal cancer while COVID-19-induced changes in healthcare may, for example, boost home-based screening or add barriers to clinic attendance; thus, the association between perceived anal cancer susceptibility and intentions to screen for anal cancer may not be understood without adjustment for the threat of COVID-19 (figure 2).

{kind=link}
{kind=link}
Confounding by perceived susceptibility to COVID-19.
Data security: CASI data are collected in REDCap which is a Health Insurance Portability and Accountability Act (HIPAA)-compliant platform. All hard copy data are kept in locked file cabinets in secure buildings. The final dataset for analysis will be de-identified and published in aggregate so confidentiality is protected. Fully de-identified datasets will be shared with properly trained investigators after assessment of institutional policies, Medical College of Wisconsin Human Protections Committee rules, as well as local, state, and Federal laws and regulations.
Ethics and dissemination
Persons not eligible are provided anal cancer educational resources (eg, https://analcancerinfo.ucsf.edu/). As a result of the COVID-19 pandemic, study activities previously conducted face-to-face were moved online whenever possible including consenting and surveys. A written consent form is used by trained staff and emphasises that (1) there is no FDA-approved HPV test for anal cancer screening; (2) persons will not be notified of baseline HPV DNA genotyping results due to high cross-sectional prevalence24 and (3) persons will be made aware of results after the 12-month swab and HRA if there is evidence of 12-month high-risk persistence. Safety monitoring of participants is conducted by clinicians and staff. The low-risk of the study activities to participants does not necessitate a data monitoring committee. This protocol is version 4.0 and was approved by the Medical College of Wisconsin Human Protections Committee. Protocol modifications which may impact on the conduct of the study, potential benefit of the participant or may affect participant safety, including changes of study objectives, study design, participant population, sample sizes, study procedures or significant administrative aspects require a formal amendment to the protocol. Study findings will be disseminated to communities where recruitment occurred and through peer-reviewed literature and conferences.
Patient and public involvement
Given that neither the feasibility of a mailed HPV self-sampling kit nor the optimal form and procedures for such a kit have been established, we employed a 10-member community advisory board (CAB) for guidance.49 Comprised of both HIV-positive and HIV-negative members of the study population, the CAB advised on the cultural competency of study materials for middle-aged, older and racial and ethnic minority SMM and transpersons. After training on anal cancer and study objectives, the CAB meets at least quarterly and provides guidance on recruitment, recruitment materials, internet webpage design, kit design, kit dissemination and interpretation of results.
Discussion
The annual incidence of SCCA among HIV-positive and HIV-negative SMM is approximately 85/100 000 and 19/100 000, respectively.3 In comparison, the current incidence of cervical cancer is approximately 7/100 000 in countries with established cervical cancer screening programmes.50 Given this achievement and given the same pathogens (and similar epidemiology, cytology and histology), initial anal cancer screening modalities have mimicked cervical cancer screening approaches51; however, while it would be optimal to detect precancers, rather than early invasive cancer, the success of this model is not certain. Indeed, the success of cervical cancer programmes is uneven with high rates of cervical cancer persisting in some high-resource countries, for example, in Eastern Europe.50 Thus, the success of an anal cancer model that mimics a cervical cancer model is not assured, especially in the context of the lack of current infrastructure for the model, for example, limited availability of HRA.
Although HPV testing is replacing cervical cancer Pap testing,52 HPV testing for anal cancer screening among SMM is often dismissed as lacking specificity given that half or more of SMM may already harbour HPV; however, screening for common cancers like cervical cancer or colorectal cancer is usually a repeated affair. Repeated HPV testing may be an acceptable screening feature among persons at increased vulnerability to anal cancer and may also support increased specificity for HSIL through the detection of persistence; however, the lack of utility for a one-time HPV test and the importance of HPV persistence in a screening programme will require education for persons who screen.
There has been little investigation of DNA testing for anal cancer screening even though DNA tests are increasingly used in cervical cancer screening.53 54 The movement to DNA tests also provides increased opportunity for self-screening since self-collected specimens better support DNA assessment compared with cytological assessment, that is, compared with Pap cytology, DNA assessment is more sensitive for high-grade cervical precancer detection.52 Home-based, self-swab programs may also increase access for those less likely to visit clinics and are cost-effective55–57; thus, our hypothesis recognises the tendency of some to avoid doctors and avoid anogenital examinations, for example, due to embarrassment.17 18 58 59
Current assessments of anal cancer screening options may support subsequent programmes that are more robust. To inform future policy, this protocol can assess some of these options including individual preference for self-screening or clinician screening, individual competency in collecting adequate specimens, home-based versus clinic-based screening impact on subsequent follow-up with HRA, and the association of two biomarkers, HPV persistence and host-viral methylation to assess risk for HSIL.
Ethics statements
Acknowledgments
The authors acknowledge the contributions of the PAC Self-Swab Community Advisory Board, Dave Wenten, Andrew Petroll, Brian Hilgeman, Sarah Lundeen, Leslie Cockerham, Maritza Pallo, Martha Abrahamsen, Bradley Sirak and Timothy McAuliffe. Thanks also to COPAN for donation of swabs and collection tubes, John Schneider, Kayo Fujimoto, April Johnsen, Winsome Panton, Jonathan Weimer, Kartikey Acharya, Sol Aldrete, Sharon O'Dwyer, Christine Hogan, Janaki Shah, Kathryn Hoffman, Thom Ertl, Dottie Wiley, Pamela Wilson, Pedro Perez, Jennifer Ward, Nicole Gerboth, Kathryn Kerhin, Anne Lakatos, Kevin Robertson, Sally Anderson, Adrienne Parnon, Stacie Ciesielski and Mary Kay Schuknecht.
References
Footnotes
Twitter @DrAlanNyitray
Collaborators Sarah Lundeen, Andrew Petroll, Brian Hilgeman, Dave Wenten, Leslie Cockerham, Martha Abrahamsen, Bradley Sirak, Timothy McAuliffe.
Contributors AGN: designed the study. EYC, VS, ARG, MEF, AAD, MS, TJR, BN and JSS: supported the technical design of study activities, laboratory protocols and instruments. MDS: supported randomisation and data analysis design. CA and BB: supervised and implemented study activities. All authors read and approved the final manuscript.
Funding The study is possible through funding from the National Cancer Institute through the National Institutes of Health to AGN (R01CA215403) and from the Medical College of Wisconsin. This study supported by funding from the Cancer Prevention Research Institute of Texas to MDS (RP170668). Copan Italia has donated swabs and collection vials to the study. None of these funding entities has any role in the design, collection, management, analysis, or interpretation of data; writing of the report; and the decision to submit this work for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.