Article Text

Abstract
Introduction Rational prescribing for older adults is a challenge because they usually exhibit multimorbidity and multimedication. One available and reliable tool to tackle this issue consists of the Screening Tool of Older People’s Prescriptions (STOPP) and the Screening Tool to Alert to Right Treatment (START), which has been associated with improvements in clinical outcomes. Our goal here is to translate and validate the STOPP-START screening tool for use with Portuguese general practitioners/family physicians.
Methods and analysis The study will be conducted in four phases: phase I—translation of the STOPP-START screening tool to Portuguese; phase II—data collection of patient data; phase III—intrarater reliability and agreement study; and phase IV—inter-rater reliability and agreement study.
Ethics and dissemination This study was approved by the Ethics Committee of the Central Health Region of Portugal (where the study will take place). Every participant will sign a written consent form. We intend to publish the full article in a related peer-reviewed journal, conference presentations, reports and in a PhD thesis.
- geriatric medicine
- quality in healthcare
- general medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study will develop the first Portuguese version of the Screening Tool of Older People’s Prescriptions and the Screening Tool to Alert to Right Treatment criteria.
This is the first study in a Portuguese primary care setting that aims to develop a useful tool for the appropriate prescription of older patients.
The main limitation of the study is that it is focused on Portugal and it may not apply to other countries where Portuguese is not the main language.
Introduction
In Organisation for Economic Co-operation and Development countries, the number of older adults is increasing1 as well as their life expectancy.2 3
Caring for older adults is a challenge for healthcare systems4 because older adults are more likely to have more than one chronic disease.5 6 For example, multimorbidity in the elderly can be higher than 90% in Portugal.5 Therefore, adults aged ≥65 years are more likely to be prescribed with multiple drugs7–9 and may be more susceptible to inappropriate medication use.10–12
Potentially inappropriate medications (PIMs) can be described as the use of medications that potentially have more risks than benefits even though safer pharmacological and non-pharmacological alternatives are available.10 Potentially inappropriate prescription is a different concept than PIM, and includes the overprescription, underprescription and misprescription of medications (eg, inappropriate dose or duration).13
There are various tools to help physicians identify PIM such as the Beers Criteria14 and the Potentially Inappropriate Medications in the Elderly list.15 The combination of the Screening Tool of Older People’s Prescriptions (STOPP) and the Screening Tool to Alert to Right Treatment (START)16 17 is another widely used tool. One of the advantages of this tool is that it not only considers PIM, but also the indications to start an appropriate medication (START).
Versus other tools, some studies have shown that the STOPP-START tool can identify a significantly higher proportion of patients requiring hospitalisation as a result of PIM-related adverse events,16 can reduce the highest number of medications and can identify more potential major clinical issues.18 The criteria for STOPP-START have been associated with improvement in prescribing quality and clinical outcomes.19 These criteria have been adapted for other languages, such as French.20 In this adaptation, 50 data sets of patients hospitalised in an academic geriatrics department were analysed independently by one geriatrician and one general practitioner. They considered 87 STOPP-START criteria of the original version. The data sets involved 418 prescribed medications. The proportions of positive and negative inter-rater agreements were 99% and 95%, respectively, for STOPP and 99% and 88% for START; Cohen’s κ coefficients were 0.95 for STOPP and 0.92 for START. The results indicated an excellent inter-rater agreement.
Inter-rater reliability of STOPP and START criteria was also tested between multiple physicians practising independently in Europe.21 After translation of the criteria into their local language, doctors in Belgium, Czech Republic, Italy, Spain and Switzerland applied the criteria to 20 data sets selected from 200 patients aged ≥65 years of a university teaching hospital in Ireland. The median κ coefficients between raters were 0.93 (0.90 to 0.96) for STOPP criteria and 0.85 (0.82 to 0.91) for START criteria. The results demonstrated good inter-rater reliability of STOPP-START criteria. Therefore, the authors concluded that STOPP and START criteria are generalisable across different European countries and languages.21
Reliability and agreement are different concepts but have been used without distinction in many studies.22 Reliability can be defined as the ratio of variability between scores of the same subjects (by different raters or at different moments) to the total variability of all scores in the sample. Agreement is connected to the question about whether observations are similar or the degree to which they differ.
We aim to make the first translation and validation23 of the English STOPP-START tool for Portuguese family doctors. In the validation study, we deal with two aspects of reliability and agreement concepts: inter-rater reliability and agreement (different raters using the translated STOPP-START tool assess the same patients), and intrarater reliability and agreement (the same rater using the translated STOPP-START tool assesses the same subjects at two different moments).
Methods and analysis
Study design
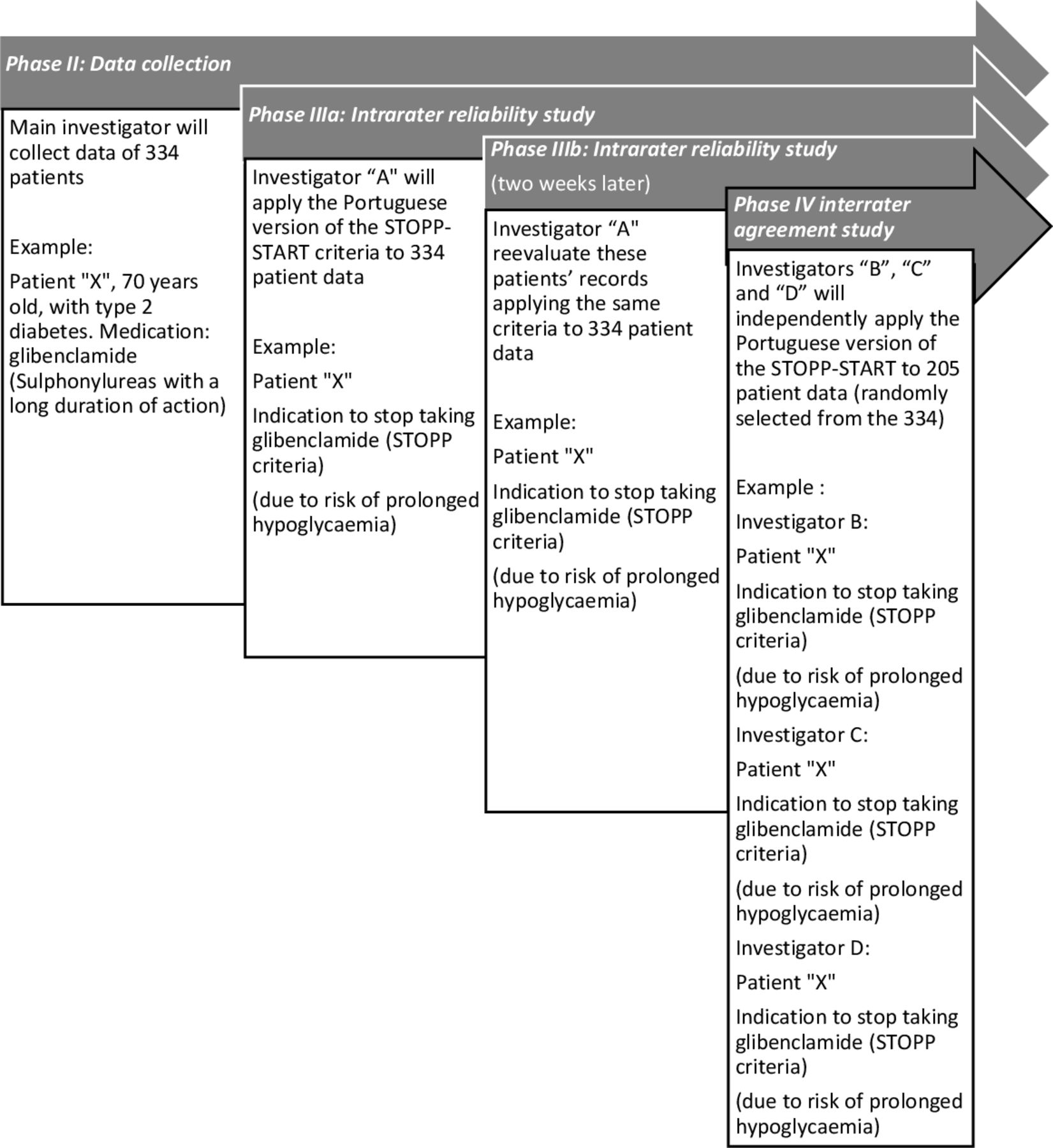
This study will be conducted in four phases as illustrated in figure 1 (timeline available in online supplemental appendix I). The first phase (phase I) is the translation to the Portuguese language followed by data collection (phase II).
Supplemental material

{kind=link}
Flow chart and example. START, Screening Tool to Alert to Right Treatment; STOPP, Screening Tool of Older People’s Prescriptions.
Phase III consists of an intrarater reliability and agreement study, and phase IV is an inter-rater reliability and agreement study. We made a preregistration on ‘Open registries Network’ (DOI 10.17605/OSF.IO/SK2RJ).
Phase I: translation to Portuguese
The translation of the STOPP-START screening tool will follow the Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes Measures.20 We have already obtained permission from STOPP-START’s authors to translate and validate the tool for Portuguese. We will recruit a key in-country consultant who is a native Portuguese and fluent English speaker and will be the main contact to perform and help with the translation. This consultant will also have a background in health research and experience in translating English documents. We will obtain two independent translations of the STOPP-START. One will be done by the key in-country consultant, and the other will be performed by a forward translator who is also a native Portuguese and fluent English speaker.
The two translations will be reconciled by the research team to obtain a final consensus translation that will be back-translated.
The back-translation (from Portuguese to English) will be done by a professional translator who is a native speaker of English and fluent speaker of Portuguese. This translator will have no prior knowledge of the original English version. Afterwards, the back-translation will be compared with the original to identify any relevant differences.
In the final step, the reconciled Portuguese STOPP-START version will be distributed to a group of 15 general practitioners to verify if there are any interpretation issues. The research team will analyse the results from the application of the STOPP-START tool to prepare the final version.
Phase II: data collection
Design
This will be a cross-sectional, analytical study.
Setting
The study will be conducted in a primary care centre in the Centre Region of Portugal.
The health unit is located in Aveiro. Five family doctors follow a total of 8165 patients; 1625 patients aged ≥65 years.
Sample size
To calculate the sample size for the validation study, we used the function CIBinary of the kappaSize package of R software.24 For the intrarater study, we obtained a sample size of 334 subjects considering the following parameters: estimated κ value: 0.6825 ; error margin: 0.1; prevalence of each item of the START criteria: 0.25; number of moments: 2; and significance level: 5%. In the inter-rater study, we obtained a sample size of 205 subjects considering the following parameters: estimated κ value: 0.6825 ; error margin: 0.1; prevalence of each item of the START criteria: 0.25; number of raters: 3; and significance level: 5%. The 205 patients for inter-rater assessment will be randomly selected from the 334 subjects used for the intrarater evaluation.
Study procedures
Recruitment of patients
Patients will be randomly selected (independent random sampling using computer-generated random digits) from a list of patients aged ≥65 years from a primary care centre. They will be invited by telephone to participate in the study. The investigator or a previously trained research associate will then interview the patients in the general practitioner office. Recruitment will continue until 334 patients are enrolled.
Exclusion criteria include incapacity or unwillingness to provide written informed consent, diagnostic of psychotic disorder, institutionalisation and the presence of terminal illness.
At inclusion, the main investigator will collect sociodemographic patient data such as age, gender, educational level, labour status and marital status. Clinical data collection will include identification of total number of medications for chronic diseases, any prescribed drugs, dosage, pharmaceutical dosage form and route of administration, the reason for taking medication, allergies, drug-related conditions and history of adverse drug reactions, and current or past conditions/diseases. A detailed list of current or past conditions/diseases that will be included is given in the online supplemental appendix II.
Supplemental material
The investigator will also collect the following information: presence or absence of ankle oedema, bone mineral density T-scores, history of influenza and pneumococcal vaccination, heart rate (beats per minute), and systolic blood and diastolic blood pressure (mm Hg).
The data are summarised in table 1.
Patients’ data (phase II)
Data source
We will collect data using electronic health record consultations and clinical patient interviews.
Database
The information collected will not include information that might identify the patients. Each patient will be numbered from 1 to 334 to protect their identity.
To evaluate data obtained throughout the study, a data safety monitoring board will be set up that will be composed of two external investigators with board expertise in this clinical field and academic and scientific activities.
Following the Portuguese Clinical Research Law, all data recorded during the study will be stored for 5 years in a safe and proper place in the primary investigator’s health centre after the closure of the investigation. All data containing participant codes will be destroyed after this period.
Phase III: intrarater reliability and agreement study
An independent researcher/family doctor (named investigator ‘A’) will apply the Portuguese version of the STOPP-START criteria to all the patients using the information collected in phase II.
Investigator ‘A’ is an independent researcher with more than 10 years of experience of clinical practice.
To ensure intrarater reliability and agreement, the same doctor will re-evaluate these patients’ records applying the same criteria 2 weeks later to avoid recall bias.26 27
Phase IV: inter-rater reliability and agreement study
Three independent investigators/family doctors (named investigators ‘B’, ‘C’ and ‘D’) will independently apply the Portuguese version of the STOPP-START using the data, collected in phase II, of 205 randomly selected participants.28 These three physicians are based in different health units and they will only have contact with the corresponding author who will give them the comprised data. Investigators ‘B’, ‘C’ and ‘D’ will independently assess the STOPP and START criteria in each of the 205 data sets and will be invited to give written comments if necessary. Inter-rater agreement will be assessed by comparing the results of the three raters.
Statistical analysis
Data will be stored with Microsoft Excel software. Data analyses will be made with SPSS Statistics V.27.0 and the software R.
Categorical variables will be described by absolute and relative frequencies.
Continuous variables will be described by mean and SD if normally distributed or by median and IQR if not normally distributed. Normality will be assessed by observation of histograms and implementation of the Kolmogorov-Smirnov test.
Intrarater/inter-rater reliability will be measured using Cohen’s κ coefficient and the respective 95% CI.22 The Cohen’s κ coefficient will be interpreted as poor (κ ≤0.2), fair (0.21 ≤ κ ≤0.40), moderate (0.51 ≤ κ ≤0.6), substantial (0.61 ≤ κ ≤0.8) and good (0.81 ≤ κ ≤1.00).29 Intrarater/inter-rater agreement will be assessed using agreement proportions and specific (positive and negative) agreement proportions and the respective 95% CI.22
A p value less than or equal to 0.05 will be considered statistically significant.
Patient and public involvement
No patient or member of the public will be involved in the design of this protocol or the establishment of intervention and the outcome measures.
Discussion
Appropriate prescriptions for older patients are a quality standard for healthcare. General practitioners are the main prescribers and they struggle to identify PIM as well as potential prescribing omissions. The STOPP-START tool is an easy way to manage the care of older patients. It is easier for daily use when adapted for the language of the prescriber.
This study is innovative because it is the first development of a Portuguese version of the STOPP-START criteria. Our research will not be merely a translation but also an adaptation done by independent general practitioners that will potentially increase the use of this version in the primary care setting.
Our research has some limitations such as the fact that even though it will be Portuguese language adaption of the STOPP-START criteria, it is only focused on Portugal and may not apply to other countries where Portuguese is used. This adapted version of STOPP-START is exclusively focused towards primary healthcare centres.
Ethics and dissemination
Every participant will sign a written consent form (online supplemental appendix III). The identity of all participants will be protected throughout the study. The documents used to collect the data of the participants will contain only an identification code of each participant using a number from 1 to 334.
Supplemental material
This protocol was approved on 30 July 2020 by the Ethics Committee of the Central Health Region of Portugal with the reference number 034-2020.
We intend to publish the full article in a related peer-reviewed journal, and results will also be disseminated in conference presentations, reports and in a PhD thesis.
Ethics statements
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @luismonteiro140, @mgfamiliarnet
Contributors LM conceived of the original idea. LM, AT and MM-S designed the protocol. LM, LVM, IR-V, AT, MM-S and CM reviewed the protocol.
Funding This article was supported by National Funds through Fundação para a Ciência e a Tecnologia (FCT), within CINTESIS, R&D Unit (reference UIDB/4255/2020).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.