Article Text

Abstract
Objective To estimate relative risk (RR) of statin-associated musculoskeletal symptoms by statin therapy intensity.
Setting Network meta-analysis assessing multicentre randomised controlled trials (RCTs) across several countries.
Participants PubMed, Web of Science, Cochrane database and ClinicalTrials.gov were searched through January 2021 for doubled-blinded RCTs testing the effect of statin therapy on lipids with at least 1000 participants and 2 years of intended treatment. Two coders assessed articles for final inclusion, quality and outcomes. Treatment intensity was categorised according to American Heart Association definitions.
Outcomes Pairwise and network meta-analysis (NMA) estimated RR and risk difference with random effects modelling. Heterogeneity was evaluated with the I2 statistic. Outcomes included muscle symptoms (any, myalgia and attrition due to muscle symptoms), rhabdomyolysis and elevated creatine kinase (CK) (>10 × upper limit of normal).
Results Of 2919 RCTs, 24 (n=152 461) met inclusion criteria. NMA results indicated risk was significantly greater for high compared with moderate intensity statin therapy for any muscle problem (RR=1.04, 95% CI 1.00 to 1.07; I2=0%), myalgia (RR=1.04, 95% CI 1.00 to 1.08; I2=0%, number needed to harm (NNH)=173), attrition due to muscle problems (RR=1.37, 95% CI 1.09 to 1.73, I2=0%, NNH=218) and elevated CK (RR=4.69, 95% CI 2.50 to 8.80; I2=7%, NNH=527). Risk also was significantly higher for high intensity compared with placebo for any muscle problem (RR=1.05, 95% CI 1.01 to 1.09, I2=0%), myalgia (RR=1.13, 95% CI 1.05 to 1.23; I2=0%, NNH=182), attrition due to muscle problems (RR=1.55, 95% CI 1.15 to 2.08, I2=0%, NNH=187) and elevated CK (RR=5.37, 95% CI 2.48 to 11.61; I2=7%, NNH=589). Due to inconsistency of results across sensitivity analyses, estimates were inconclusive for rhabdomyolysis and CK. There were no significant differences in risk between moderate intensity therapy and placebo for all outcomes.
Conclusions For approximately each 200 patients on high intensity statins, one additional patient may experience myalgia or discontinue therapy due to muscle problems compared with moderate intensity therapy.
Trial registration number CRD42019112758.
- cardiac epidemiology
- coronary heart disease
- clinical pharmacology
- general medicine (see internal medicine)
- health & safety
- cardiology
Data availability statement
Data are available in a public, open access repository. Extra data can be accessed via the Dryad data repository at http://datadryad.org/ with the doi.org/10.5061/dryad.kprr4xh2q.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- cardiac epidemiology
- coronary heart disease
- clinical pharmacology
- general medicine (see internal medicine)
- health & safety
- cardiology
Strengths and limitations of this study
High-quality, large randomised controlled trials (RCTs) analysed with low risk of heterogeneity bias.
Novel use of network meta-analysis to compare treatment intensities allows for large analysis of dose-dependent effect.
Coding of outcome terms directly as reported by investigators to minimise bias.
Study-level data preclude meta-analysis with regression for relevant covariables affecting risk of outcome.
Heterogeneity of terms across trials prevented analysis of full trial set for each outcome.
Introduction
The Cholesterol Treatment Trialists’ Collaboration meta-analysis (MA) on patient-level data from large randomised controlled trials (RCTs) demonstrated that statin therapy is efficacious in reducing major vascular events.1 2 Statin therapy is now prominent in cholesterol management guidelines.3–8 Statin-associated muscle symptoms (SAMS), however, may lead to non-adherence or discontinuation with therapy and ultimately to poorer cardiovascular outcomes.7 Most RCTs have shown small, insignificant increases in risk for SAMS, although patients taking statins may complain of muscle problems and may discontinue therapy due to muscle problems.3 For example, a 2016 MA found a non-significant increase in myopathy. However, it did not report on the more mundane myalgias that often cause statin attrition.3 These milder symptoms are the major public health concern, as statin non-adherence can lead to significant increases in risk of major adverse cardiovascular events.3 Observational studies suggest that these mild SAMS may occur as often as 7%–29% of patients.7 One review9 suggested that clinical observations of increased muscle problems with statin therapy may be due to patient expectations.
SAMS also may be more likely with higher intensity therapy. Although this is assumed to be true, especially with the evidence against simvastatin 80 mg,10 11 few RCTs have examined high intensity therapy.12 13 This study used a network meta-analysis (NMA) to combine evidence across trials to estimate the risk of SAMS by treatment intensity. In contrast to pair-wise MA that directly estimates causal effects, an NMA can indirectly estimate risk between placebo and moderate, moderate and high, and between placebo and high intensity treatment, even though placebo, moderate and high intensity treatment levels were not compared within a single trial. Results contribute to the debate about whether muscle adverse events are due solely to patient expectations or whether statins might have an independent effect on symptoms. Finally, this study contributes to the ongoing debate as to whether statins cause myalgias and attrition due to muscle problems without marked creatine kinase (CK) elevations.
Methods
The trials
PubMed, Cochrane Database, Web of Science and ClinicalTrials.gov were searched for “systematic reviews” and “meta-analysis” in the title, abstract or keywords prior to 31 January 2021 to identify eligible trials (Prospero #CRD42019112758; see online supplementfor search terms and strategy). Double-blinded RCTs to improve lipid levels comparing statin therapy with placebo or higher lower dose statin therapy were selected. In order to detect most adverse events, RCTs were selected that had at least 1000 participants with 2 years of intended follow-up, where statin treatment was not given with other prescription drug therapies, and results contained reports on muscle-related adverse events. Both authors independently reviewed trials for final inclusion and coded each for quality with Oxford Center for Evidence-based Medicine ratings14 and a five-point Jadad quality score.15 Any disagreements were reconciled by joint review and discussion.
Supplemental material
Patient and public involvement
Patients were not involved in design or implementation of this study.
Exposure variable
Studies were classified by intensity of statin treatment (‘high’ or ‘moderate’) according to American Heart Association definitions for potency in reduction of lipid levels.16 High intensity signifies an expected 50% or greater reduction in Low-density lipoprotein cholesterol (LDL-C) levels when taking that statin (ie, 80 mg atorvastatin) and moderate signifies 30%–50% reduction in LDL-C.16
Outcome variables
Adverse muscle-related events were coded into five main outcomes. The first outcome was for any patient-reported muscle complaint coded from reports of ‘muscle aches’, ‘pains’, ‘cramps’, ‘stiffness,’ ‘musculoskeletal disorders’, etc. The second focused on only myalgia or muscle pain. The third focused on attrition due to musculoskeletal complaints. A fourth captured explicit reporting of rhabdomyolysis, with or without a trial definition. The fifth was elevated CK, greater than 10 times the upper limit of normal (CK>10 × ULN). This threshold was used to distinguish this outcome from less meaningful CK increases and also because CK>10 × ULN is commonly reported in RCTs. All outcomes were coded as reported by original investigators in published and online reports and were independently coded by both authors. Ambiguities were resolved by contacting trial investigators.
Analysis
Published aggregate data from each trial were used. A crude estimate of incidence was calculated from the total number of cases observed divided by the total person-years (using the median or mean follow-up time for each study), and a χ2 test was used to test for homogeneity in the proportion of incident cases across studies, within each arm, although these crude estimates ignored randomisation. To facilitate interpretation and comparison of results to the original trials, risk of adverse effects was estimated with pooled relative risk (RR). A 0.50 continuity correction was added to aggregate frequencies for trials that observed zero cases of an outcome in either treatment arm. A pairwise MA was used to estimate the RR (Mantel-Haenszel method, random effects as implemented in the meta package in R)17 18 for a statin effect by treatment intensity from direct (head–head comparison) trials (online supplement contains detailed results for random effects with Mantel-Haenszel and inverse variance methods). Because aggregations across studies are only meaningfully interpreted when results are consistent across studies, heterogeneity among RCTs was assessed with an index of consistency across trials (I2 Q)19 20 and funnel plots. When I2 <25%, results are considered to be at low risk of bias due to heterogeneity; high values (>75%) indicate high risk of bias due to heterogeneity.19 20 Residual I2 represents the heterogeneity remaining after accounting for subgroups of treatment intensity. Cochrane’s Q (a subcomponent of I2) indicates the probability that the observed heterogeneity is due to chance. Sensitivity analyses included omitting outliers identified in funnel plots and using a 0.10 as a ‘continuity correction’. In addition, analyses were conducted excluding the simvastatin 80 mg studies because of US Food and Drug Administration (FDA) muscle-related safety warnings.21
An NMA, conducted in R,22 used all available pairs of comparisons for each outcome to estimate increased risk between the three levels of treatment exposure. Prespecified comparisons were between placebo and moderate intensity, between moderate and high intensity therapy and between placebo and high intensity. The RR was used to estimate effect size (frequentist, inverse variance method and random effects), so that results would be comparable across original studies and the pairwise MA previously. In contrast to an MA that provides a direct estimate of the RR, an NMA provides estimates by combining direct and indirect evidence from all data. A ratio test was used to test for consistency between NMA direct and indirect estimates.23 Heterogeneity was assessed with and I2 and Q statistics.19 20 Number needed to harm (NNH; the inverse of the absolute difference in incidence) was estimated when the pooled RR was significantly greater than 1.0 and the pooled absolute risk reduction (risk difference (RD)) was significantly greater than 0.0. Sensitivity analyses included replacement of zeros with 0.10 and with 0.0001.
Results
Searches yielded 134 relevant reviews, including 2919 RCTs that reduced to 24 unique RCTs that met eligibility requirements (see online supplement). Of the 24 RCTs: 17 were placebo-moderate intensity comparisons,24–44 3 were placebo-high intensity comparisons45–47 and 4 were moderate to high intensity comparisons10–13 (table 1). The active blood pressure treatment arm of the HOPE-3 trial37 was excluded, but the statin only and placebo only arms were retained, allowing for a statin and placebo comparison. Two trials compared moderate and high intensity therapy using 80 mg/day of simvastatin.10 11 All 24 RCTs scored the highest quality (1) on the Oxford rating and on the Jadad scale 18 scored 5/5 and 6 scored 4/5 (missing detail on random assignment). The RCTs included heterogenous patient populations, for example, healthy middle-aged adults26 37 43 46 to end-stage renal disease (ESRD) patients. Sample sizes ranged from 125524 to 20 53640 with follow-up periods from 1.946 to 6.710 years. Of the 24 RCTs, 6 were included in the 2006 MA,48 17 in the 2014 systematic review,49 23 in the 2016 MA3 and 18 in the 2013 NMA.50 None of the previous analyses separated trials into subgroups by treatment intensity. Crude estimates of incidence increased with intensity of treatment from placebo to moderate intensity to high intensity therapy but with heterogeneity across trials (online supplemental file 1).
Description of the trials
Any muscle symptoms
Twenty-three trials reported some type of muscle symptom,10 13 25–29 31 35 39 40 46 47 myositis,34 myalgia,12 24 30 32 33 42 45 myopathy,24 38 or discontinuation due to muscle-related symptoms.11 13 36 The pairwise MA pooled across subsets of trials indicated consistent trial results with a 1% non-significant increase in risk between placebo and moderate intensity therapy, a 3% non-significant increase between placebo and high intensity therapy (figure 1) and a 5% significant increase between moderate and high intensity therapy (RR=1.05, 95% CI 1.01 to 1.09; p=0.027, four RCTs, n=30 720; I2=0%). Sensitivity analyses indicated that RRs were essentially unchanged without an outlier30 identified on the funnel plot, with a 0.10 correction, or without the simvastatin 80 mg trials (online supplemental file 1).

Any muscle problems. RR, relative risk.
The NMA pooled direct and indirect evidence from all 23 trials and suggested increased risk with higher intensity therapy. Results (table 2) indicated a 1% non-significant increase in risk between placebo and moderate intensity therapy, a 4% significant increase between moderate and high intensity therapy (RR=1.04, 95% CI 1.00 to 1.08; p=0.031) and a 5% significant increase between placebo and high intensity therapy (RR=1.05, 95% CI 1.01 to 1.09; p=0.012). The RRs were consistent across studies (I2=0%; Q, p=0.54), were not significantly different between direct and indirect estimates (p=0.48) and were not sensitive to substitutions for zero values. Pooled RDs between pairs of treatment groups were not significantly different from zero. There were no outliers in the NMA analysis. Exclusion of the two simvastatin 80 mg trials did not meaningfully change risk, but comparisons with high intensity were not statistically significant, likely due to the decreased sample size (online supplemental file 1).
RR and RD results for comparisons of treatment intensity pairs
Myalgia or pain
Thirteen RCTs reported cases of myalgia,25 29–32 42 44–47 attrition due to myalgia26 28 or pain and/or weakness.40 The pairwise MA indicated (figure 2) a 13% non-significant increase in myalgia between placebo and moderate intensity, a 9% non-significant increase between placebo and high intensity and a 4% significant increase between moderate and high intensity (RR=1.04, 95% CI 1.00 to 1.09, p=0.040, two RCTs, n=22 065; I2=0%). The three trials comparing placebo and high intensity therapies suggested moderate heterogeneity in results (I2=45%). Funnel plots did not suggest bias by any of the studies, and there were no zero cells (online supplement). Exclusion of the simvastatin 80 mg trial did not meaningfully change the magnitude of risk, although results were non-significant for high intensity compared with moderate intensity therapy possibly due to decreased sample size (online supplemental file 1).
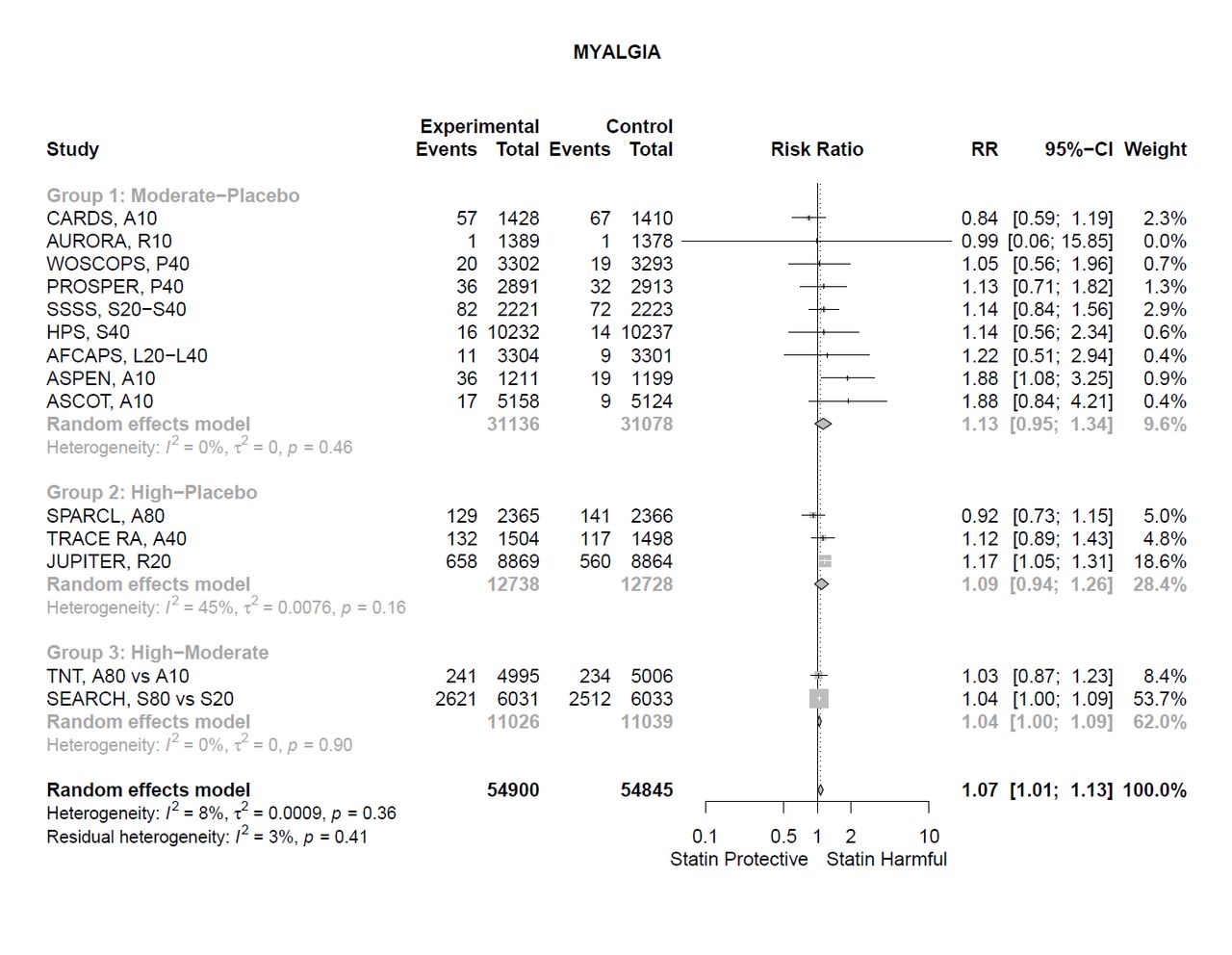
Myalgia or pain. RR, relative risk.
The NMA results combining evidence for all 13 trials suggested an increase in myalgia with increased therapy intensity (table 2). There was a 9% non-significant increase in risk between placebo and moderate intensity therapy, a 4% significant increase between moderate and high intensity therapy (RR=1.04, 95% CI 1.00 to 1.08; p=0.046) and a 13% significant increase in risk for high intensity therapy compared with placebo without heterogeneity (RR=1.13, 95% CI 1.05 to 1.23; p=0.002). The RRs were consistent across studies (I2=0%, Q, p=0.48) and direct and indirect estimates were not significantly different (p=0.63). The pooled RD was significant between high and moderate intensity (NNH=173) and between high intensity and placebo (NNH=154) with low heterogeneity (I2=20%; Q, p=0.25). Exclusion of the simvastatin 80 mg trial did not change the magnitude of risk although results were not significant for high intensity compared with moderate intensity therapy (online supplement).
Attrition
Attrition due to muscle problems was reported by eight RCTs that compared moderate intensity statin therapy with placebo,25 26 28 32 36–38 40 44 three that compared moderate with high intensity therapy10 11 13 and none that directly compared high intensity to placebo. In the pairwise MA (figure 3), patients on moderate intensity statin therapy had a 13% non-significant increase in attrition due to muscle problems compared with placebo. Patients on high intensity therapy had a 38% significantly higher attrition rate than those on moderate intensity (RR=1.38, 95% CI 1.04 to 1.82; p=0.024, three RCTs, n=20 719) with moderate heterogeneity across trials (I2=31%). Funnel plots did not suggest bias, and there were no zero cells. Exclusion of the two simvastatin 80 mg trials left only one moderate to high intensity comparison RCT (online supplemental file 1).

Attrition due to muscle symptoms. RR, relative risk.
The NMA results for the 11 trials suggested that risk for attrition increased with intensity of therapy. There was a 13% non-significant increase in risk between placebo and moderate intensity therapy (table 2), a 37% significant increase in risk between moderate and high intensity (RR=1.37, 95% CI 1.09 to 1.73; p=0.007) and a 16% significant increase in risk between placebo and high intensity therapy (RR=1.16, 95% CI 1.15 to 2.08; p=0.004). The RRs were consistent across studies (I2=0%; Q p=0.72) and closely paralleled direct results provided by the MA, but the NMA provided an estimate for the placebo-high intensity comparison for which there were no head-to-head trials. The pooled RD between moderate and high intensity therapy was significant, and the NNH was 218. The pooled RD between high intensity therapy and placebo also was significant, and the NNH was 186. Exclusion of the two simvastatin 80 mg trials resulted in a slightly lower risk estimate for the moderate to high comparison and a slightly higher estimate for the placebo to high comparison, and both were non-significant (online supplemental file 1).
Rhabdomyolysis
Rhabdomyolysis was reported on by 14 moderate intensity-placebo comparison RCTs,24–28 30–32 35 36 39–42 four moderate to high intensity comparison RCTs10–13 and three high intensity-placebo comparison RCTs.45–47 Incidence of rhabdomyolysis was very low, and statistical comparisons were not conclusive. Pairwise MA indicated a 39% non-significant increase in rhabdomyolysis incidence between placebo and moderate intensity therapy, 145% non-significant increase between moderate and high intensity and a 4% non-significant decrease between placebo and high intensity therapy (figure 4). Results were inconclusive as estimates were not robust across sensitivity analyses. Approximately half (22/42) of the cells were zeros, and RR increased for the moderate-high intensity comparison with a smaller correction and removal of the simvastatin 80 mg trials meaningfully changed effect sizes (online supplemental file 1).

Rhabdomyolysis. RR, relative risk.
NMA results based on all 21 trials indicated increased risk for rhabdomyolysis with increased intensity of therapy (table 2). There was a 22% non-significant increase in risk between placebo and moderate intensity therapy, a 33% non-significant increase between moderate and high intensity and a 66% non-significant increase between placebo and high intensity therapy with consistency across trials (I2=0%, Q p=0.99). Direct and indirect RR estimates were not significantly different (p=0.31). Results were not consistent after exclusion of simvastatin 80 mg trials or replacement of zeros but remained non-significant (online supplemental file 1).
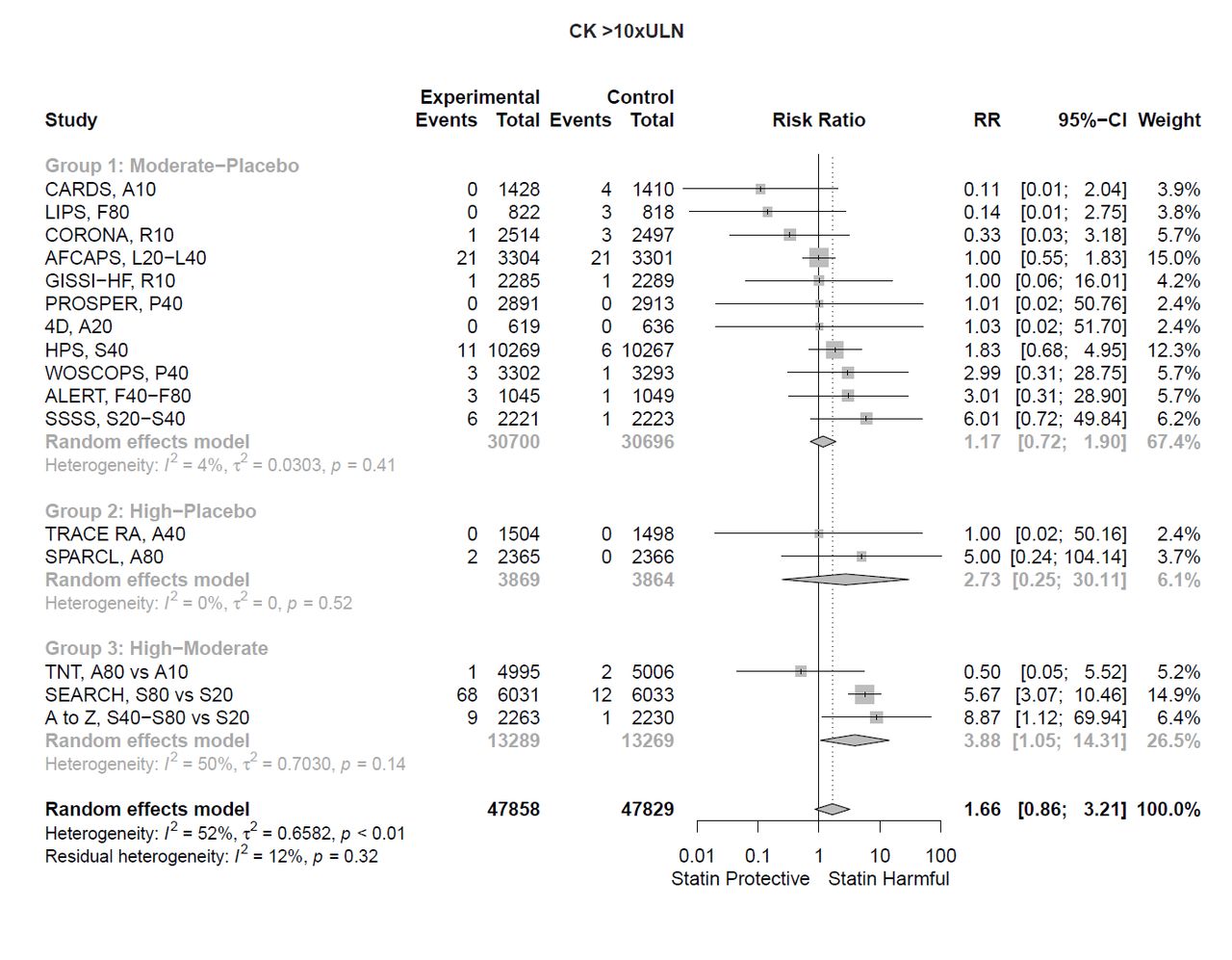
Elevated CK
Of 16 RCTs, 11 compared rates of elevated CK (CK>10 × ULN) between placebo and moderate intensity therapy,24–27 32 35 36 39–43 three compared moderate to high intensity therapy10–12 and two compared high intensity therapy with placebo.45 47 Incidence of elevated CK was low. Pairwise MA indicated (figure 5) a 17% non-significant increase in CK elevation between placebo and moderate intensity therapy, a 173% non-significant increase between placebo and high intensity therapy and a 288% significantly higher risk for high compared with moderate intensity (RR=3.88, 95% CI 1.05 to 14.31; p=0.042, three RCTs, n=26 558) with some heterogeneity among the three trials (I2=50%). Estimates were not stable across sensitivity analyses. Removal of two possible outliers,10 26 exclusion of simvastatin 80 mg trials and adjustment for cells with zeros (9/32) meaningfully changed RR estimates (online supplemental file 1).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CK >10 × upper limit of normal (ULN). RR, relative risk.
Using evidence from all 16 trials, the NMA estimates indicated increased risk with increased intensity. NMA results indicated a 14% non-significant increase between placebo and moderate intensity therapy (table 2), a 359% significant increase in CK elevation between moderate and high intensity (RR=4.59, 95% CI 2.32 to 9.10; p<0.0001) and a 425% significant increase between placebo and high intensity (RR=5.25, 95% CI 2.29 to 12.03; p<0.0001). Results were consistent across trials (I2=7%, Q p=0.37), and direct and indirect RR estimates were not significantly different (p=0.57). The pooled RD between moderate and high intensity therapy was significantly different from zero, and the NNH was 527. The pooled RD between high intensity therapy and placebo also was significant, and the NNH was 589. There were no outliers in the NMA analysis. Although results were homogeneous with the simvastatin 80 mg trials, exclusion of these trials meaningfully reduced risk associated with statin therapy between moderate and high intensity and between placebo and high intensity therapy, and smaller zero replacement values increased risk estimates (online supplemental file 1).
Discussion
A novel contribution of this study was the application of NMA to estimate the dose–response effect of statin therapy on muscle symptoms using clinically meaningful categories of treatment intensity. The NMA RR estimates closely paralleled the direct estimates, indicating reliability of estimates and increased risk with high intensity statin therapy. The NMAs provide information about risk by using all available evidence, whereas traditional meta-analyses are limited only to direct, head-to-head comparisons. For patient-reported symptoms, there were non-significant increases in SAMS between placebo and moderate intensity therapy and significant increases between moderate and high intensity therapy. Because simvastatin 80 mg therapy is now restricted because of muscle injury,51 analyses also were run with and without those trials. This did not meaningfully affect results for patient-reported outcomes. Rhabdomyolysis and elevated CK also showed increased risk with higher intensity, but because of low incidence (with 25%–50% zero cells) and inconsistency across sensitivity analyses, results were inconclusive.
Double-blinded RCTs and traditional meta-analyses3 48 49 suggest no significant increase in risk of muscle adverse events with statin therapy. Since most evidence comes from moderate intensity trials, possible adverse effects of high intensity therapy may be masked in aggregate estimates. In this study, high intensity therapy and focused definitions of patient-reported muscle problems detected higher risk. However, the absolute excess of SAMS was less than 1% for all outcomes. In previous meta-analyses, absolute excess of muscle problems also was small but non-significant.3 49 The 2016 MA estimated risk for extreme outcomes (myopathy and rhabdomyolysis) but did not analyse patient reports of milder SAMS that we present and that concern patients. We did not code for myopathy as an outcome, because we did not have access to patient-level data and could not determine if elevated CK co-occurred with myalgia.
Direct lower higher dose comparisons in individual RCTs were not consistent; for example, the SEARCH10 and A to Z trials found a significant increase in CK and the TNT trial12 did not. An NMA that compared dosage increments within brands50 suggested no systematic increase in risk for myalgia or discontinuation with higher dosages. These negative findings may have been due to smaller sample sizes, smaller dosage increments in restricted comparisons or exclusion of the simvastatin 80 mg trials.50 In this study, results were homogeneous including the simvastatin 80 mg trials and indicated high intensity therapy significantly increased myalgia compared with placebo even after their exclusion. The previous NMA did identify a dose–response relationship between statin dose and mildly elevated CK (2–3 × ULN) but only for lovastatin and simvastatin.50 CK>10 × ULN may be more interpretable than modest elevations, and in this study, it was significantly increased with high-intensity statin therapy. While removal of 80 mg simvastatin trials had little effect on patient-reported symptoms, their exclusion resulted in smaller non-significant increases in risk for elevated CK. It is unclear if simvastatin 80 mg was responsible for the significant increases in CK.
A practical question concerns how large an excess of cases might be observed with statin therapy for myalgia/pain, attrition due to muscle problems, and elevated CK or rhabdomyolysis. Although estimates based on observational studies suggest that incidence of mild SAMS might be as high as 30% among statin users,52 RCTs suggest a much lower rate. In this study, pooled risk estimates suggested that for each 173 patients on high intensity therapy, one additional patient will experience statin-caused myalgia, and for each 218 patients, one additional patient will discontinue therapy due to muscle problems compared with those on moderate intensity therapy. This represents numerous patients who are at greatest risk for major vascular events as these are often higher risk patients. Discontinuation of statins in the elderly (>75 years) may result in 33% increased risk of a cardiovascular event within 3 months53 and adherence to statins in those 65 years and older may reduce mortality by a third.54
Myalgias and attrition due to SAMS are important outcomes for the average patient but have not received as much attention as rhabdomyolysis and myopathy. This study provides evidence that while blinded, moderate intensity statin takers did not report significantly more general muscle problems or myalgias, but those on high intensity therapy did. Because many myalgia cases occurred without CK elevation increases, this also serves as evidence that SAMS occur in the absence of large elevations in CK. Clinicians with patients who are ‘statin intolerant’ may consider encouraging the patient to first decrease intensity of statin therapy, rather than discontinuing it, in light of these findings.
This analysis also contributes to the ‘nocebo’ debate. A large, unblinded follow-up of RCT patients suggested SAMS are expectation related.29 They observed an incidence of 2.03% and 2.00% muscle-related adverse events in statin and placebo groups, respectively, when double blinded (HR=1.03) and 1.26% and 1.00% in the statin and usual care groups when unblinded (HR=1.41).29 Both comparisons indicate absolute differences less than 1%. A recent N-of-1 trial55 also found minimal differences in muscle symptoms when patients took statin versus placebo (blinded) but significantly more muscle symptoms when taking a placebo versus taking nothing (unblinded). Both nocebo and causal effects are small, although they can result in increased SAMS. In a clinical setting, SAMS with moderate intensity therapy may be the result of patient expectations, but with high intensity therapy, SAMS may be due to expectations and statin therapy. Intensity of treatment and patient expectations may need to be considered before making changes in statin therapy in the absence of CK elevations.
A limitation of study-level meta-analyses is that definitions,56 assessment and variable reporting of muscle-related outcomes may differ across studies. Aggregation of heterogeneous outcomes and estimated outcomes (eg, myopathy) not explicitly reported by investigators can mask an effect. Protocol differences may partially explain incidence disparities across studies. However, use of the RR to estimate effect size minimises bias due to between-study variations in protocol (eg, using a symptom checklist vs recording spontaneous mention of symptoms and then categorising responses).
Estimates in this analysis may have underestimated SAMS by excluding patients with statin hypersensitivity, as four studies12 37 40 45 (n=48 950) employed statin ‘washout’ phases and eight trials24 25 30 32 34–37 47 (n=34 042) excluded patients with known statin hypersensitivity. Collins et al3 noted that ‘statin hypersensitivity’ exclusion was a rare occurrence across these trials, as almost all patients enrolled were statin naïve at screening. The risk of attrition due to SAMS and rhabdomyolysis was actually highest in SEARCH, where an 8-week long, active run-in phase was conducted,3 10 although no patients were excluded for elevated muscle enzymes.10 Also, an N-of-1 trial in patients who were considering stopping or who had stopped statin therapy because of muscle symptoms found no difference in severity of patient-reported muscle symptoms between statin and placebo groups.57 Because simvastatin 80 mg trials comprise a high proportion of high intensity treatment evidence, this may limit interpretation of CK and rhabdomyolysis risk. Also, adverse events may have been increased due to the presence of comorbidities; only three trials studied healthy adults (n=30 756).26 37 46 A final limitation is that although risk estimates are based on the best available evidence and should provide relatively unbiased estimates, CIs and alpha significance levels may be approximate due to multiple comparisons.
Conclusion
Statins may cause SAMS but at much lower rates than observational data suggest. We found significant but small increases in risk for patient-reported muscle problems on high-intensity statins. Complaints of SAMS in observational studies may be related to statin therapy or patient expectations but more likely may be due to methodological biases or the generally high prevalence of muscle problems.
Data availability statement
Data are available in a public, open access repository. Extra data can be accessed via the Dryad data repository at http://datadryad.org/ with the doi.org/10.5061/dryad.kprr4xh2q.
Ethics statements
Acknowledgments
We would like to thank Julie Trumble, our research librarian, for performing the search and providing guidance in optimising the search strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Both authors are responsible for the design and implementation of the study. The first author (JD) selected studies for inclusion, compiled the data for the outcomes of interest, analysed the data in R and is responsible for the final manuscript in its entirety. SCW was responsible for the oversight and implementation of the project. She was the second coder for all trials and offered guidance and support in all decisions regarding design and implementation of the analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.